Skin nonmelanocytic tumor
Fibrous, fibrohistiocytic and myofibroblastic neoplasms
Superficial angiomyxoma
Authors: Charmaine Ilagan, M.D., Juan Putra, M.D.
Editorial Board Member: Bethany R. Rohr, M.D.


Last author update: 6 May 2025
Last staff update: 6 May 2025
Copyright: 2001-2025, PathologyOutlines.com, Inc.
PubMed search: Superficial angiomyxoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Ilagan C, Putra J. Superficial angiomyxoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticsuperficialangio.html. Accessed September 15th, 2025.
Definition / general
- Superficial angiomyxoma (cutaneous myxoma) is a rare, benign lobulated / multinodular lesion composed of bland spindled and stellate cells in myxoid stroma with arborizing, thin walled vessels
- Initially described by Carney et al. in 1985 in association with Carney complex (Medicine (Baltimore) 1985;64:270)
Essential features
- Rare, benign cutaneous neoplasm with a propensity for local recurrence, ~30 - 40% after incomplete excision
- Presents as a slow growing, painless mass
- Well circumscribed mass (~1 - 5 cm) with yellow gelatinous cut surface
- Multiple lesions may occur in the setting of Carney complex
Terminology
- Cutaneous myxoma
ICD coding
- ICD-O: 8841/0 - superficial angiomyxoma
- ICD-10: D21.9 - benign neoplasm of connective and other soft tissue, unspecified
- ICD-11: 2E84.0 & XH58A9 - benign fibrogenic or myofibrogenic tumor of skin & superficial angiomyxoma
Epidemiology
- Rare (0.0008 - 3%) (J Cutan Pathol 2009;36:56, Ear Nose Throat J 2024;103:478)
- Represents < 0.3% of all soft tissue neoplasms (J Cutan Pathol 2009;36:56)
- M > F
- Most commonly seen in middle aged adults (mean age: 20 - 40 years) (Am J Surg Pathol 1988;12:519, Am J Surg Pathol 1999;23:910)
- Rare in children (Pediatr Dermatol 2011;28:200, Turk Patoloji Derg 2018;34:262, J Pediatr Adolesc Gynecol 2020;33:727)
Sites
- Head and neck, trunk, lower extremities and genital region (Am J Surg Pathol 1988;12:519, Arch Craniofac Surg 2021;22:62, Ear Nose Throat J 2024;103:478, Int J Surg Pathol 2023;31:852)
- Common sites in patients with Carney complex: external ear canal, eyelid, nipples (Semin Dermatol 1995;14:90, Am J Surg Pathol 1994;18:274, Am J Surg Pathol 2023;47:296)
Pathophysiology
- Unknown
Etiology
- Unknown
- Multiple lesions may arise in the setting of Carney complex
- Carney complex is due to either mutations in PRKAR1A gene that encodes protein kinase A regulatory subunit 1 alpha or MYH8 gene that encodes perinatal myosin (Lancet Oncol 2005;6:501)
Clinical features
- Presents as soft, slow growing, painless papule or polypoid cutaneous mass
- Multiple lesions may arise in the setting of Carney complex (J Dermatol 2002;29:790)
- Carney complex inherited in an autosomal dominant manner is characterized by skin pigment abnormalities, cutaneous, cardiac and breast myxomas, endocrine tumors or overactivity and psammomatous melanotic schwannomas (GeneReviews: Carney Complex [Accessed 19 December 2024])
Diagnosis
- Definitive diagnosis is based on the excision specimen
Radiology description
- Ultrasound: well defined, heterogenous and mildly echogenic ovoid mass with posterior acoustic enhancement (Clin Case Rep 2023;11:e7374, Jpn J Radiol 2015;33:216)
- Computed tomography (CT): well defined, slightly enhancing, low density mass (Clin Case Rep 2023;11:e7374, Jpn J Radiol 2015;33:216)
- Magnetic resonance imaging (MRI): well defined border with isointense signal relative to skeletal muscle on T1 weighted imaging and a markedly high signal intensity on T2 weighted imaging (Clin Case Rep 2023;11:e7374, In Vivo 2023;37:503)
Radiology images
Images hosted on other servers:

Ultrasound

CT


MRI
Prognostic factors
- Overall good prognosis
- Local recurrence after incomplete resection is 30 - 40% (Am J Surg Pathol 1988;12:519, Am J Surg Pathol 1999;23:910, Ann Diagn Pathol 2000;4:99)
- Average recurrence time is 18 months (Ann Diagn Pathol 2000;4:99)
- No metastatic potential
Case reports
- 6 year old boy with a posterior neck mass (Arch Craniofac Surg 2021;22:62)
- 24 year old woman with a left shoulder nodule (Cureus 2024;16:e67521)
- 24 year old woman with a left ear pinna mass (Arch Clin Cases 2023;10:128)
- 42 year old man with a left axillary mass (Cureus 2023;15:e48472)
- 56 year old man with a mass in the left prescrotal area (Jpn J Radiol 2015;33:216)
Treatment
- Primary treatment is complete surgical excision (Am J Surg Pathol 1988;12:519, Am J Surg Pathol 1999;23:910)
- Long term follow up due to risk of recurrence (Am J Surg Pathol 1988;12:519, Am J Surg Pathol 1999;23:910)
- Chemotherapy or radiation are not indicated
Clinical images
Images hosted on other servers:

Left shoulder mass

Protruding pinna mass

Left axillary mass
Gross description
- Usually 1 - 5 cm (Am J Surg Pathol 1988;12:519)
- Usually a well circumscribed solitary lesion with yellow gelatinous cut surface
- Vaguely multinodular due to presence of thin fibrous septa
- May be poorly circumscribed
Gross images
Images hosted on other servers:

Well defined, yellow mass

Well defined, encapsulated mass

Well encapsulated, yellow mass
Microscopic (histologic) description
- Well circumscribed lobulated / multinodular lesion located in dermis; it can extend into underlying subcutis
- Vague lobules divided by thin fibrous septa
- Hypocellular lesion composed of haphazardly arranged, bland spindled and stellate cells embedded in myxoid stroma, sometimes forming irregular clefts
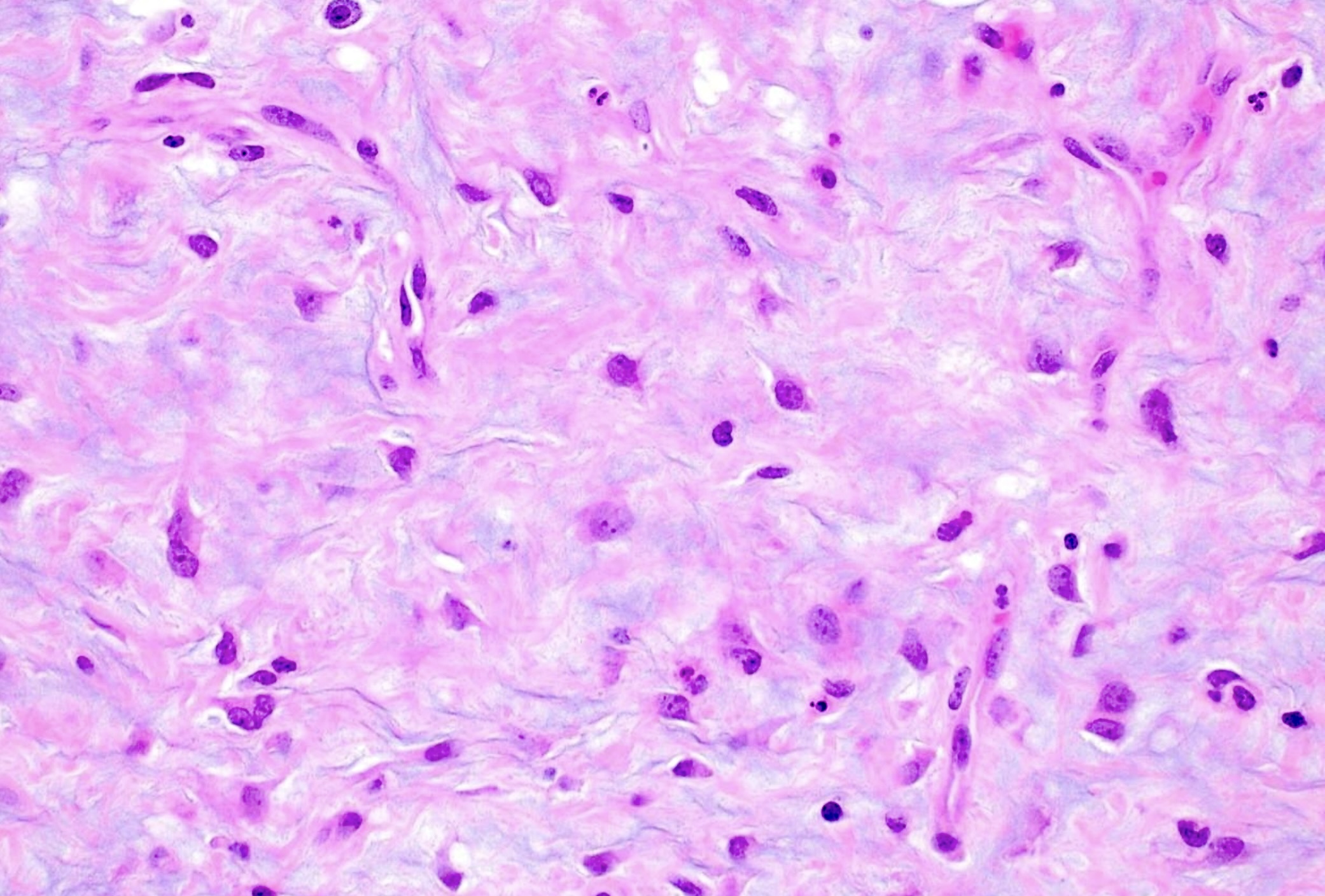
- Spindled and stellate cells with bland nuclei often with intranuclear vacuoles and inconspicuous nucleoli
- Binucleated or multinucleated cells may be seen
- Arborizing, thin walled vessels, often prominent
- Scattered mixed inflammatory infiltrates in stroma, predominantly neutrophils
- Mast cells often present
- No significant atypia, necrosis or increased mitotic figures
- Entrapped benign epithelial elements (epidermoid cyst or strands of squamous or basaloid cells) likely represent entrapped adnexa in up to 25% of cases (Ann Diagn Pathol 2000;4:99)
Microscopic (histologic) images
Contributed by Charmaine Ilagan, M.D. and Juan Putra, M.D.
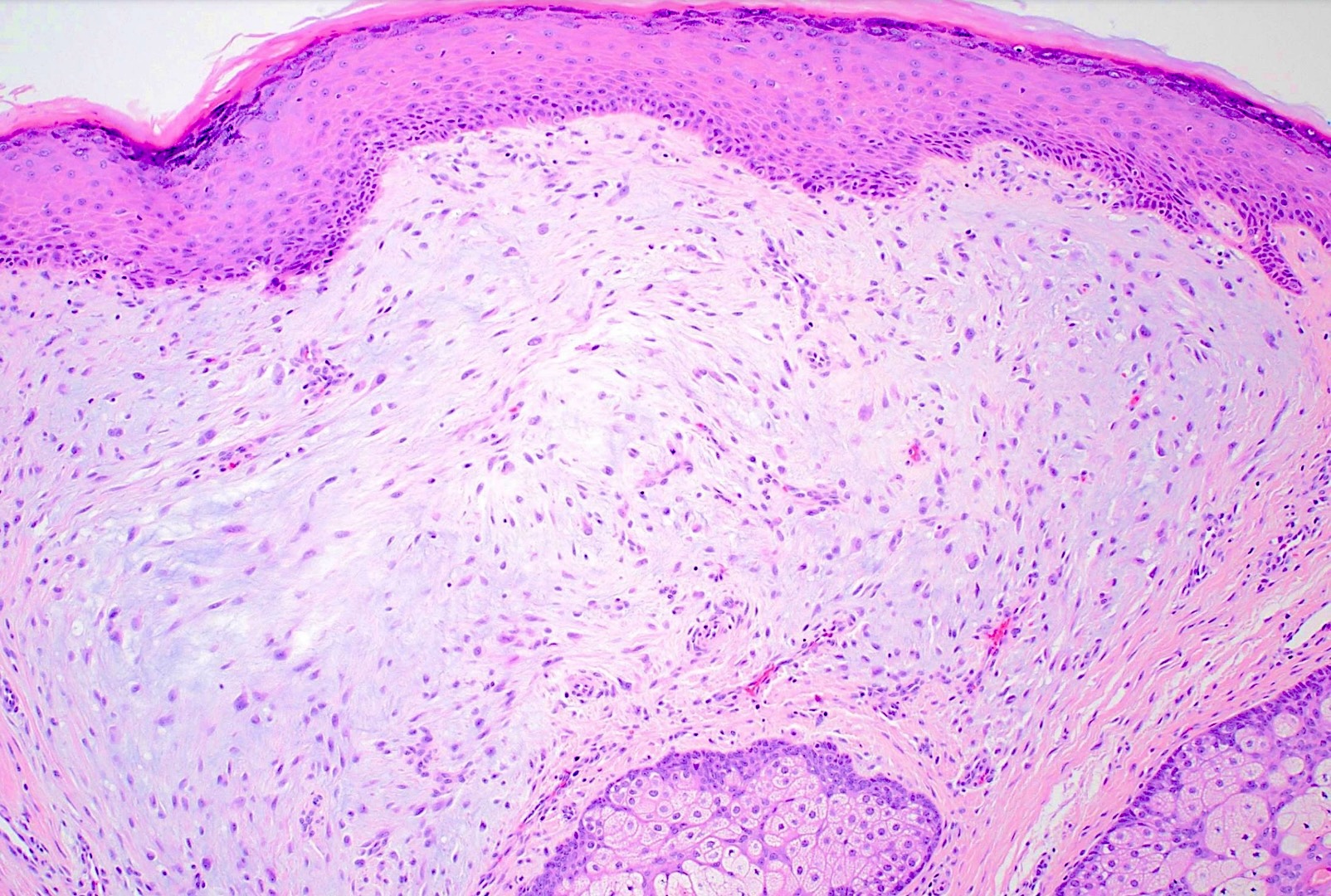
Well defined tumor
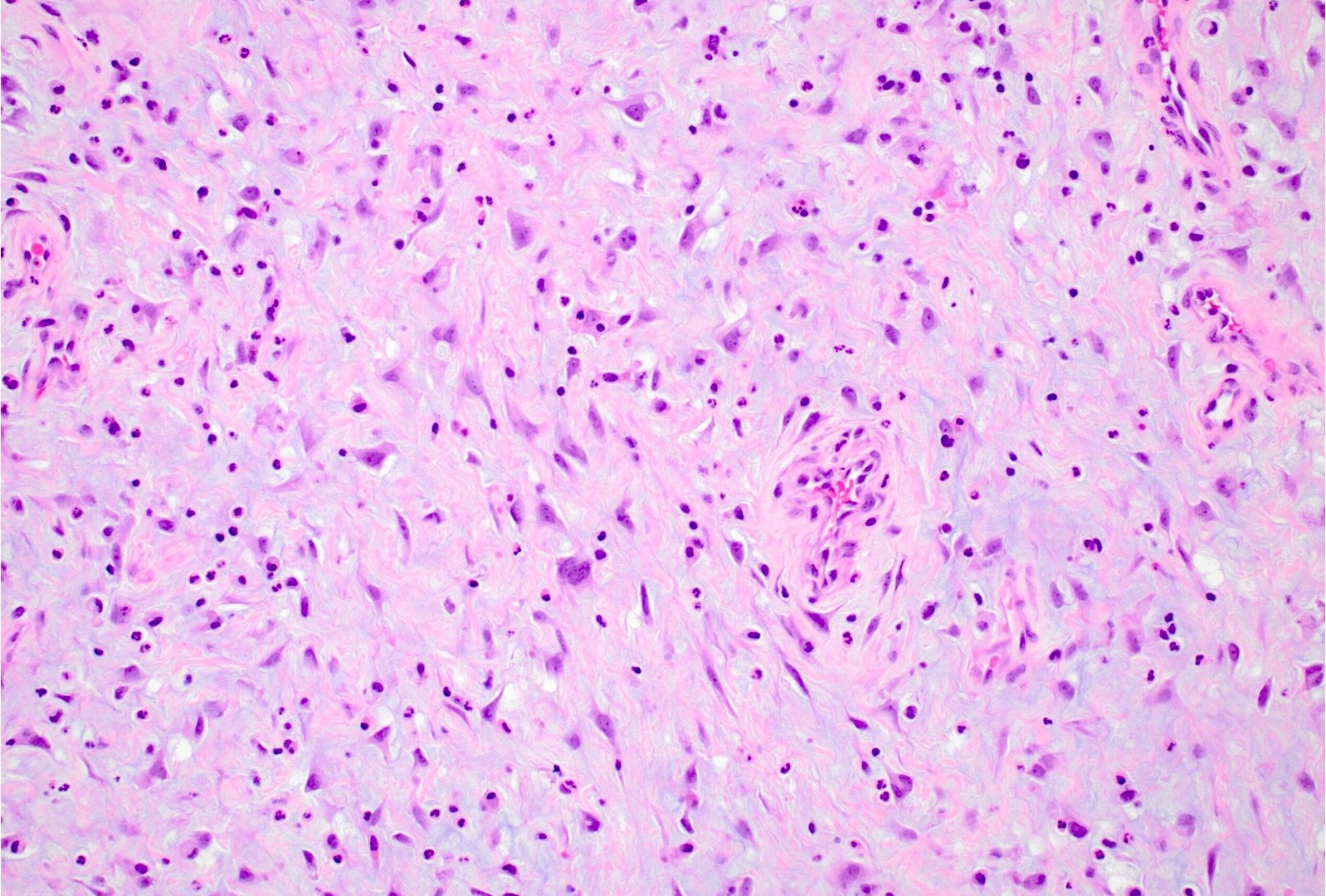
Spindled and stellate cells
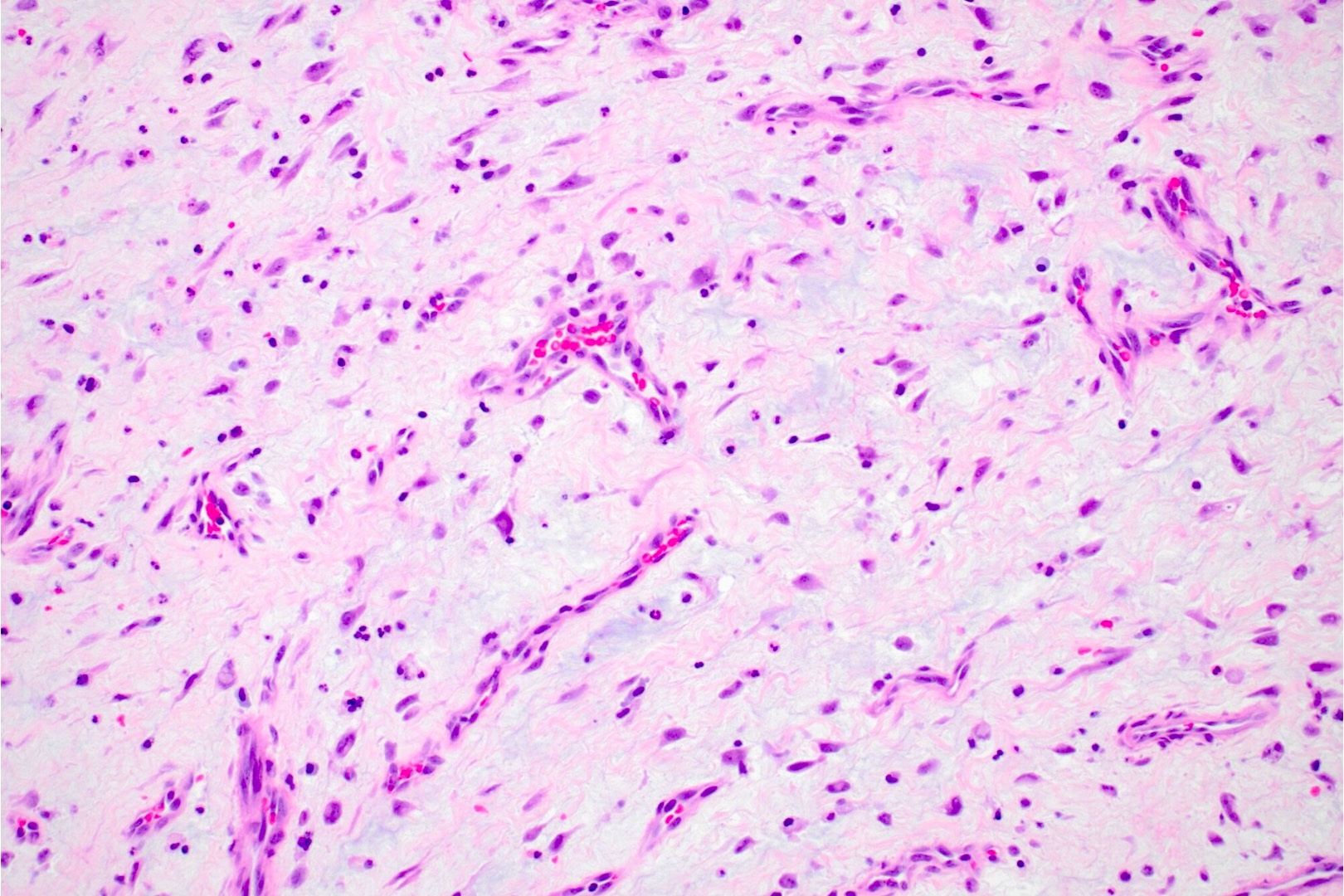
Thin walled vessels
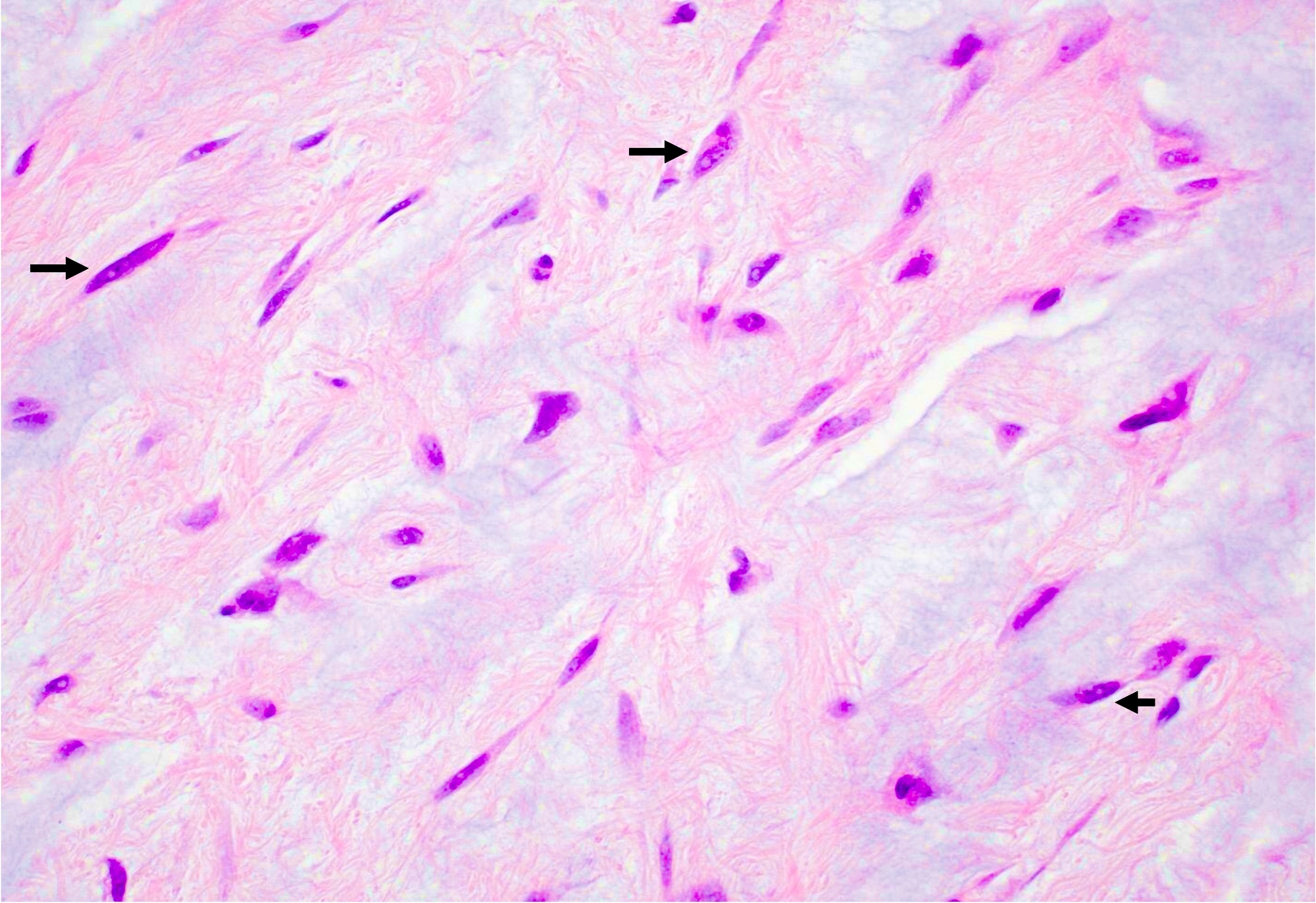
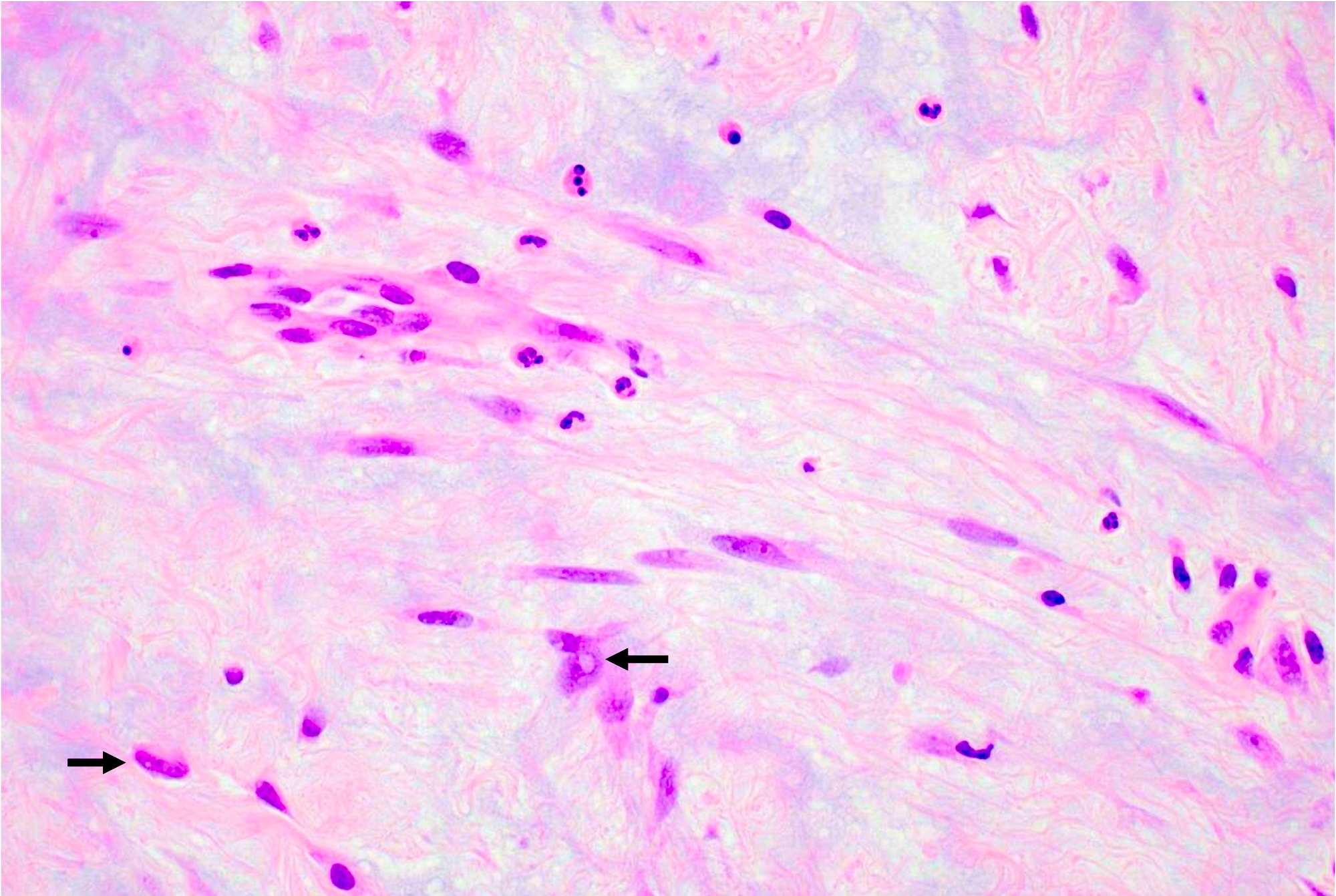
Intranuclear vacuoles
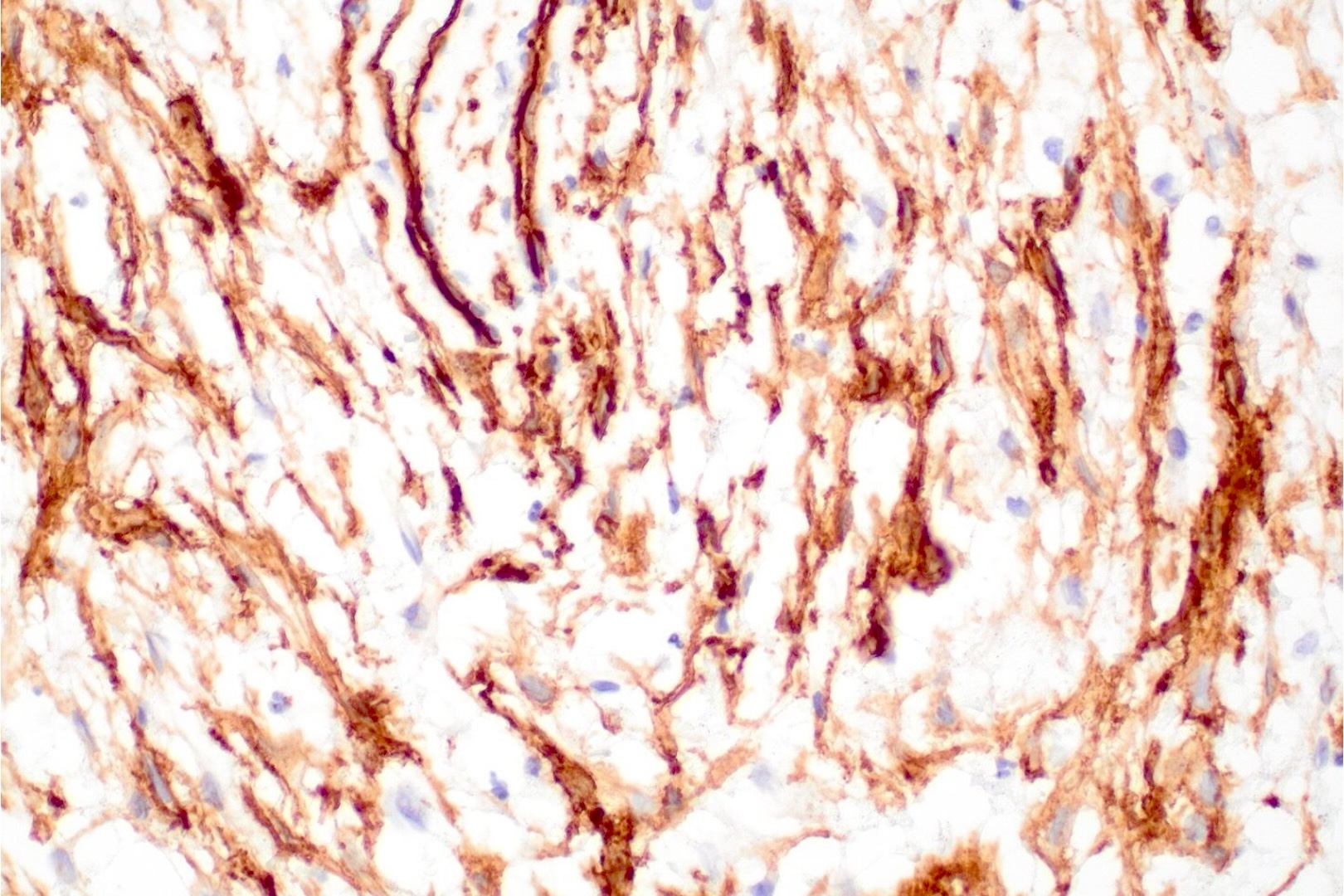
CD34
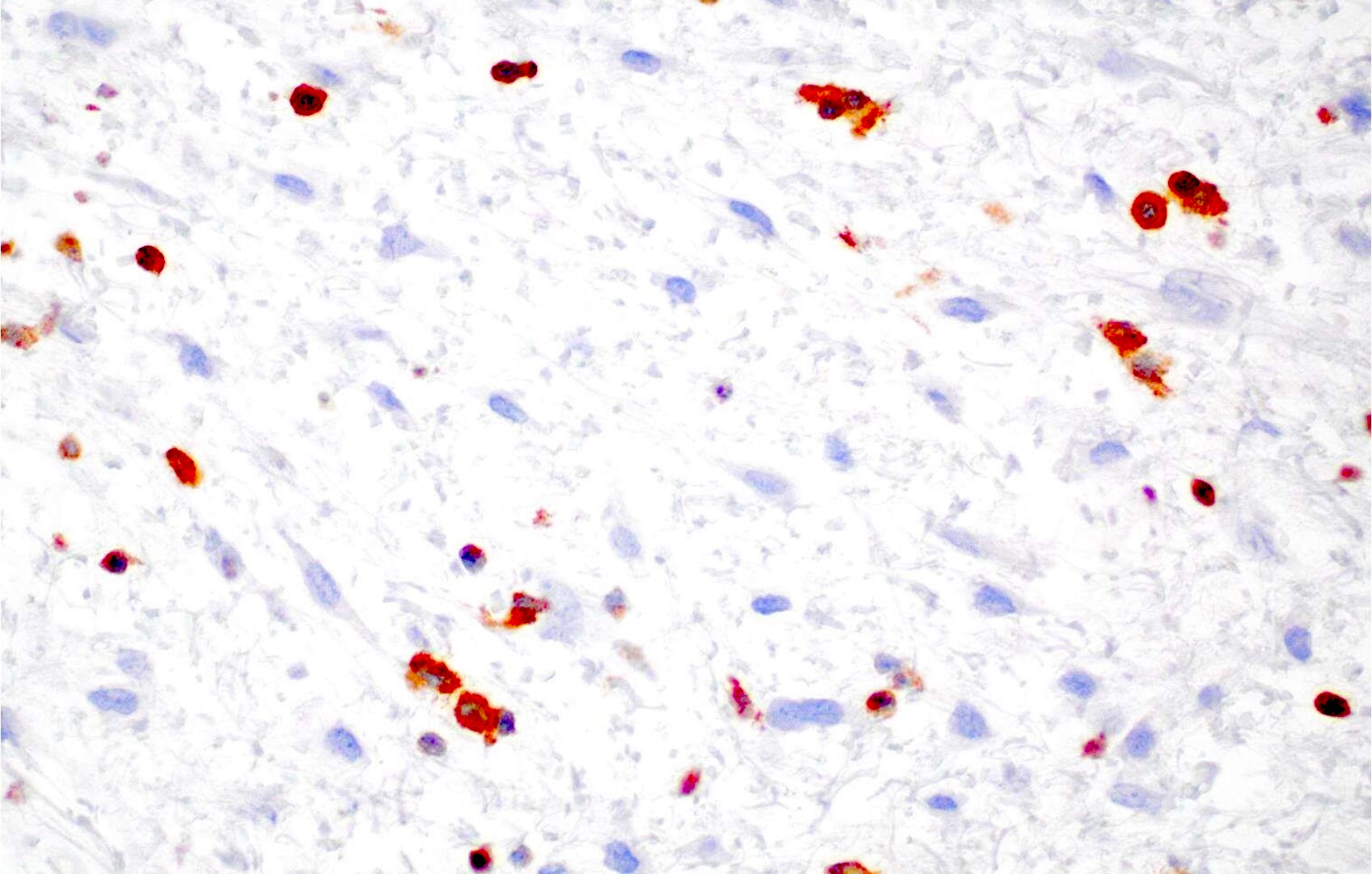
PRKAR1A
Virtual slides
Images hosted on other servers:

Soft palate mass

Right breast mass
Cytology description
- Moderately cellular with plump spindle and stellate cells on a fibrillary myxoid background with scattered neutrophils (Arch Clin Cases 2023;10:128)
- Bland spindle cells with oval to elongated nuclei and moderate amount of cytoplasm (Arch Clin Cases 2023;10:128)
Cytology images
Images hosted on other servers:

Spindle cells, myxoid background
Positive stains
- Vimentin
- Variable CD34, SMA, S100 (Int J Gynecol Pathol 1997;16:325, Hum Pathol 2022;120:71)
Negative stains
- CK AE1 / AE3, EMA, GFAP, desmin, MUC4, ER, PR (Int J Gynecol Pathol 1997;16:325, Hum Pathol 2022;120:71)
- Loss of PRKAR1A expression (not specific for Carney) in ~55.2 - 80% of cases (Am J Surg Pathol 2022;46:226, Histopathology 2022;80:1001)
Molecular / cytogenetics description
- PRKAR1A mutation for cases associated with Carney complex (Lancet Oncol 2005;6:501)
Videos
Superficial angiomyxoma (cutaneous myxoma) and other cutaneous myxoid lesions by Dr. Jerad Gardner
Superficial angiomyxoma (cutaneous myxoma) by Dr. Jerad Gardner
Sample pathology report
- Soft tissue, left axilla, excision:
- Superficial angiomyxoma (see comment)
- Comment: Sections demonstrate a well circumscribed lobulated lesion involving the dermis and extending to subcutis. The hypocellular lesion is composed of bland spindled and stellate cells with eosinophilic cytoplasm embedded in myxoid stroma. There is no significant atypia or increased mitotic activity identified. Scattered arborizing thin walled vessels and neutrophils in the stroma are identified. Immunohistochemical stains show that the lesional cells are positive for CD34 and SMA, while negative for cytokeratin AE1 / AE3, S100, GFAP, desmin, MUC4, ER and PR.
Differential diagnosis
- Cutaneous focal mucinosis (Cureus 2021;13:e18618):
- Usually smaller lesions (< 1 cm)
- Mucin deposition usually in upper dermis
- Rarely extends into subcutis
- Lacks prominent vasculature and scattered stromal neutrophils
- Intramuscular myxoma:
- Often located deep within the muscles of extremities
- Infiltrating into adjacent skeletal muscle
- Lacks prominent vasculature
- GNAS mutation
- May be associated with Mazabraud syndrome
- Myxoid neurofibroma:
- Dermal nerve sheath myxoma (Diagnostic Histopathology 2016;22:152):
- Superficial acral fibromyxoma (Diagnostic Histopathology 2016;22:152):
- Periungual or subungual region of fingers and toes
- Moderately cellular lesion composed of spindled to stellate cells arranged in loose storiform or fascicular pattern in myxoid and collagenous stroma
- Prominent microvasculature
- Positive for CD34 (diffuse), CD99 (diffuse), SMA (focal)
- Loss of nuclear Rb expression
- Aggressive angiomyxoma:
- Larger lesions (> 10 cm) in deep soft tissue of genital, pelvic and perineal regions, usually in females
- Infiltrative lesion with bland spindled and stellate cells
- Variably sized vessels with small thin walled to large thick walled vessels, often with hyalinization
- Myoid bundles near vessels
- HMGA2, ER, PR positive
- Myxoid liposarcoma:
- Usually in deep soft tissue of extremities, most common in the thigh
- Characteristic plexiform vasculature with scattered lipoblasts
- Subset may show high grade hypercellular areas
- t(12;16) FUS::DDIT3 or very rarely t(12;22) EWSR1::DDIT3
- Low grade fibromyxoid sarcoma (Diagnostic Histopathology 2016;22:152):
- Low grade myxofibrosarcoma (Diagnostic Histopathology 2016;22:152):
- Multinodular growth pattern with infiltrative margins in myxoid stroma
- Hyperchromatic pleomorphic cells with curvilinear vessels
- Necrosis and increased mitotic figures (including atypical mitotic figures) seen in intermediate and high grade tumors
Additional references
Practice question #1
A 25 year old man presents with a painless mass on the posterior neck that gradually developed over 2 months. The mass, which measures 2 cm, is well circumscribed and has a gelatinous cut surface. The tumor cells are positive for CD34, while negative for MUC4, ER, PR and SOX10. What is the diagnosis?
- Aggressive angiomyxoma
- Low grade fibromyxoid sarcoma
- Myxoid neurofibroma
- Superficial angiomyxoma
Practice answer #1
D. Superficial angiomyxoma. The image above shows superficial angiomyxoma, which is a slow growing, painless mass that usually measures 1 - 5 cm in its greatest dimension. Grossly, the tumor is well circumscribed and has a yellow, gelatinous cut surface. Microscopically, the tumor cells are bland spindled and stellate cells in myxoid stroma with prominent arborizing thin walled vessels. The tumor cells are positive for CD34, while negative for ER, PR, SOX10 and MUC4. Answer A is incorrect because aggressive angiomyxomas are usually larger (> 10 cm) and involve the deep soft tissue of the genital, pelvic and perineal regions. They are infiltrative lesions with bland spindled and stellate cells and have variably sized vessels, often with hyalinization. The tumor cells are positive for ER, PR and HMGA2. Answer B is incorrect because low grade fibromyxoid sarcomas have bland spindle cells in whorling or fascicular pattern in alternating collagenous and myxoid stroma. The tumor cells are positive for MUC4 and EMA. t(7:16) FUS::CREB3L2 or t(11;16) FUS::CREB3L1 are characteristic gene fusions for low grade fibromyxoid sarcoma. Answer C is incorrect because myxoid neurofibromas have spindle cells with wavy nuclei in myxoid stroma and less conspicuous vasculature. The tumor cells are positive for SOX10, S100 and CD34.
Comment Here
Reference: Superficial angiomyxoma
Comment Here
Reference: Superficial angiomyxoma
Practice question #2
Which of the following is true regarding superficial angiomyxoma?
- It has no metastatic potential
- Multiple lesions may be associated with Mazabraud syndrome
- t(12;16) FUS::DDIT3 gene fusion is characteristic
- Tumor cells exhibit marked pleomorphism with presence of necrosis and increased mitosis
Practice answer #2
A. It has no metastatic potential. Answer B is incorrect because multiple superficial angiomyxomas may be associated with Carney complex. Mazabraud syndrome is associated with intramuscular myxoma and fibrous dysplasia. Answer C is incorrect because t(12;16) FUS::DDIT3 gene fusion is seen in myxoid liposarcoma. Answer D is incorrect because tumor cells in superficial angiomyxoma are bland spindled and stellate cells with no significant atypia, necrosis or increased mitosis.
Comment Here
Reference: Superficial angiomyxoma
Comment Here
Reference: Superficial angiomyxoma
