Vulva & vagina
Other carcinomas
Basal cell carcinoma-vulva
Authors: Juan Pablo Pineda Reyes, M.D., Lucy Ma, M.D.
Editorial Board Member: C. Blake Gilks, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.

Last author update: 30 January 2024
Last staff update: 12 June 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Basal cell carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Pineda Reyes JP, Ma L. Basal cell carcinoma-vulva. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/vulvabasalcellcarc.html. Accessed October 4th, 2025.
Definition / general
- Basal cell carcinoma (BCC) arises from epithelial cells of either epidermis or hair follicle stem cells
- Vulvar BCC is rare
- Histologic features are identical to that of BCC occurring elsewhere on the skin
Essential features
- Characterized by the presence of nests of basaloid / hyperchromatic nuclei with minimal cytoplasm
- Predominantly seen in older (mean: seventh decade) White women
- Occurs most commonly in the labium majus but can involve any other area of vulva
- Excellent prognosis with up to 21% rate of local recurrence and very rare metastasis
Terminology
- Not recommended: basalioma of the vulva, basal cell epithelioma of the vulva
ICD coding
Epidemiology
- Accounts for < 5% of all vulvar cancers and < 1% of all basal cell carcinomas (J Am Acad Dermatol 2001;45:68, Gynecol Oncol 2005;97:192)
- Mean patient age is ~70 years (Gynecol Oncol 2005;97:192, Dermatol Surg 2023;49:13)
- Predominantly seen in White women
Sites
- Cutaneous epithelium of the vulva but may involve mucosal epithelium as well
- Most common location: labium majus followed by clitoris (Int J Dermatol 2019;58:892)
Pathophysiology
- Arises from skin epithelial cells or hair follicle stem cells (Cell Stem Cell 2015;16:400)
- Inactivating mutations in PTCH1 may contribute to BCC genesis in the absence of ultraviolet irradiation (Cancer Cell 2018;33:229)
- Mutations in TP53
- Activating mutations of SMO
- HPV independent
Etiology
- Unclear; etiology might differ from that of BCC in sun exposed skin
- Proposed risk factors include
- Chronic vulvar irritation
- History of pelvic radiation therapy (J Am Acad Dermatol 2001;45:68)
- Advanced age
- White race
- Basal cell nevus syndrome (Gorlin syndrome) due to germline PTCH1 mutations
- Xeroderma pigmentosum
- Immunosuppression (Gynecol Oncol 2005;97:192)
- Exposure to arsenic (TJ Obstet Gynaecol Br Emp 1956;63:697)
- Syphilis infection (TJ Obstet Gynaecol Br Emp 1956;63:697)
- Local trauma (Gynecol Oncol 2005;97:192, J Am Acad Dermatol 2001;45:68)
Clinical features
- Frequently asymptomatic
- In symptomatic patients, pruritus is the most frequent symptom (Int J Gynecol Pathol 2023;42:327, Gynecol Oncol 2016;142:440)
- Vulvar lump sensation, palpable vulvar mass, erythema, ulceration, irritation, pain, bleeding (Gynecol Oncol 2005;97:192)
- Clinical appearance ranges from erythematous papules and patches to plaques or nodules with or without ulceration or pigmentation (J Am Acad Dermatol 2001;45:68)
- Dermoscopy findings are identical to BCC in other body areas
- Presence of arborizing vessels and blue globules, shiny white structures (Dermatol Pract Concept 2018;8:68, Arch Dermatol 2007;143:426, J Eur Acad Dermatol Venereol 2017;31:e180)
Diagnosis
- Definite diagnosis requires biopsy / excision
Prognostic factors
- Overall prognosis is excellent
- Local recurrence rates range from 0% to 21% in different case series (Int J Gynecol Pathol 2022;41:86, Cancer 1969;24:460, Int J Dermatol 2019;58:892)
- Lymph node and distant metastasis can occur but is rare
- Features with increased risk for recurrence and metastasis
- Size > 5 - 20 mm, tumor thickness, extension into the subcutis, perineural invasion, aggressive histological subtype (morpheaform, infiltrative, basosquamous) and surgical margins < 3.0 mm (Obstet Gynecol 1997;90:765, Int J Gynecol Pathol 2022;41:86)
Case reports
- 51 year old woman with a 1.5 cm firm vulvar lesion with shallow red ulcerations at the lower mons pubis (Cureus 2021;13:e20791)
- 51 year old woman with a history of incompletely resected vulvar basal cell carcinoma, now with bilateral lung nodules and inguinal lymphadenopathy (Gynecol Oncol Rep 2016;18:32)
- 70 year old woman with vulvar basal cell carcinoma and bilateral inguinal lymph node metastases (Case Rep Oncol 2019;12:573)
- 80 year old woman with a history of repeated exposure to perineal heat lamps presents with a 1.8 cm pink pearly eroded plaque on the left vulva (JAAD Case Rep 2020;6:103)
- 83 year old woman with a history of lichen sclerosus presents with a tender, 5 mm eroded papule on the right labium majus (Int J Dermatol 2019;58:892)
Treatment
- Primary treatment is wide local excision or vulvectomy with margin assessment (Gynecol Oncol 2016;142:440)
- Surgical excision by Mohs micrographic surgery or PDEMA (peripheral and deep en face margin assessment) (J Natl Compr Canc Netw 2023;21:1181)
- Radiotherapy for nonsurgical candidates
- If not feasible, systemic therapy with HHIs (hedgehog pathway inhibitors) may be recommended (J Natl Compr Canc Netw 2023;21:1181)
Clinical images
Images hosted on other servers:

Irregularly shaped and ulcerated tumor

Well limited plaque with a pigmented border

Multiple indurated nodules
Gross description
- Pink, pearly nodule, with or without elevated borders and telangiectasias
- Ulceration or dark brown pigment may be present
- Flat, scar-like lesion in superficial BCCs
- Reference: Calonje: McKee’s Pathology of the Skin, 5th Edition, 2019
Microscopic (histologic) description
- Identical diagnostic criteria to BCC occurring elsewhere on the skin
- Basaloid tumor cells with uniform hyperchromatic / basophilic nuclei and scant cytoplasm
- Peripheral palisading of tumor cells with variety of architectural patterns
- Retraction artifact of tumor nests from surrounding stroma (also known as clefting)
- Stromal changes
- Fibromyxoid change, calcification, amyloid deposition
- May be colonized by nonneoplastic melanocytes and may contain melanin pigment
- With or without squamous differentiation
- Most frequent histologic subtype is nodular, followed by superficial and infiltrative
- References: Calonje: McKee’s Pathology of the Skin, 5th Edition, 2019, Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
Microscopic (histologic) images
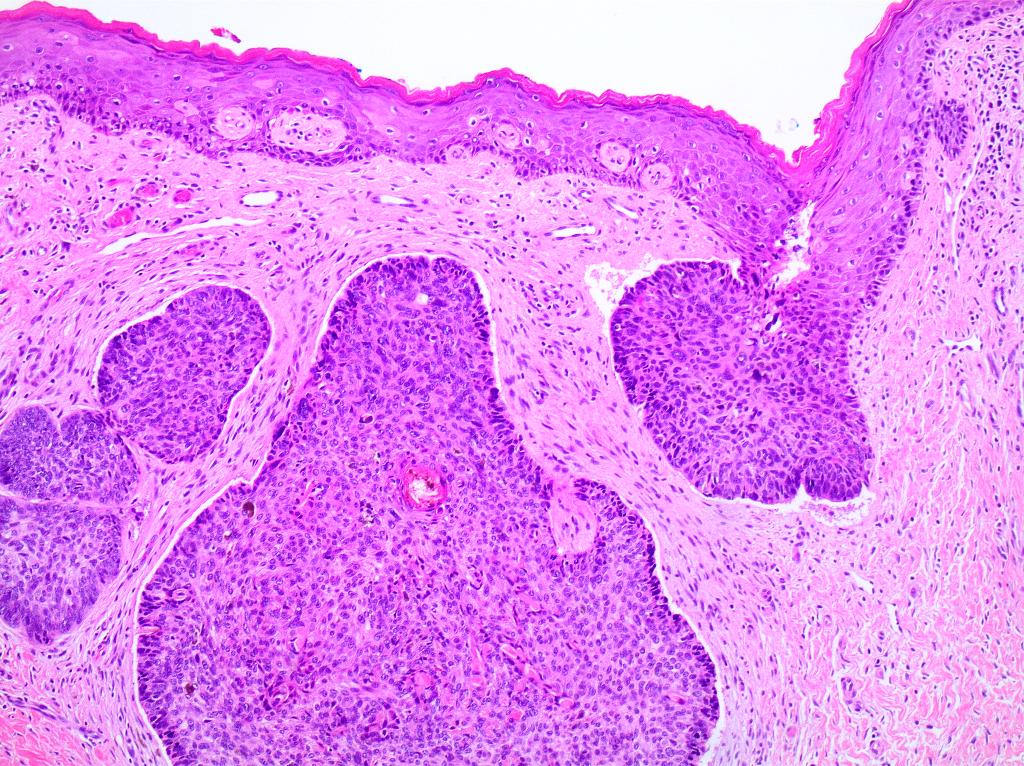
Contributed by Lucy Ma, M.D., Priya Nagarajan, M.D., Ph.D. and Stephanie L. Skala, M.D.
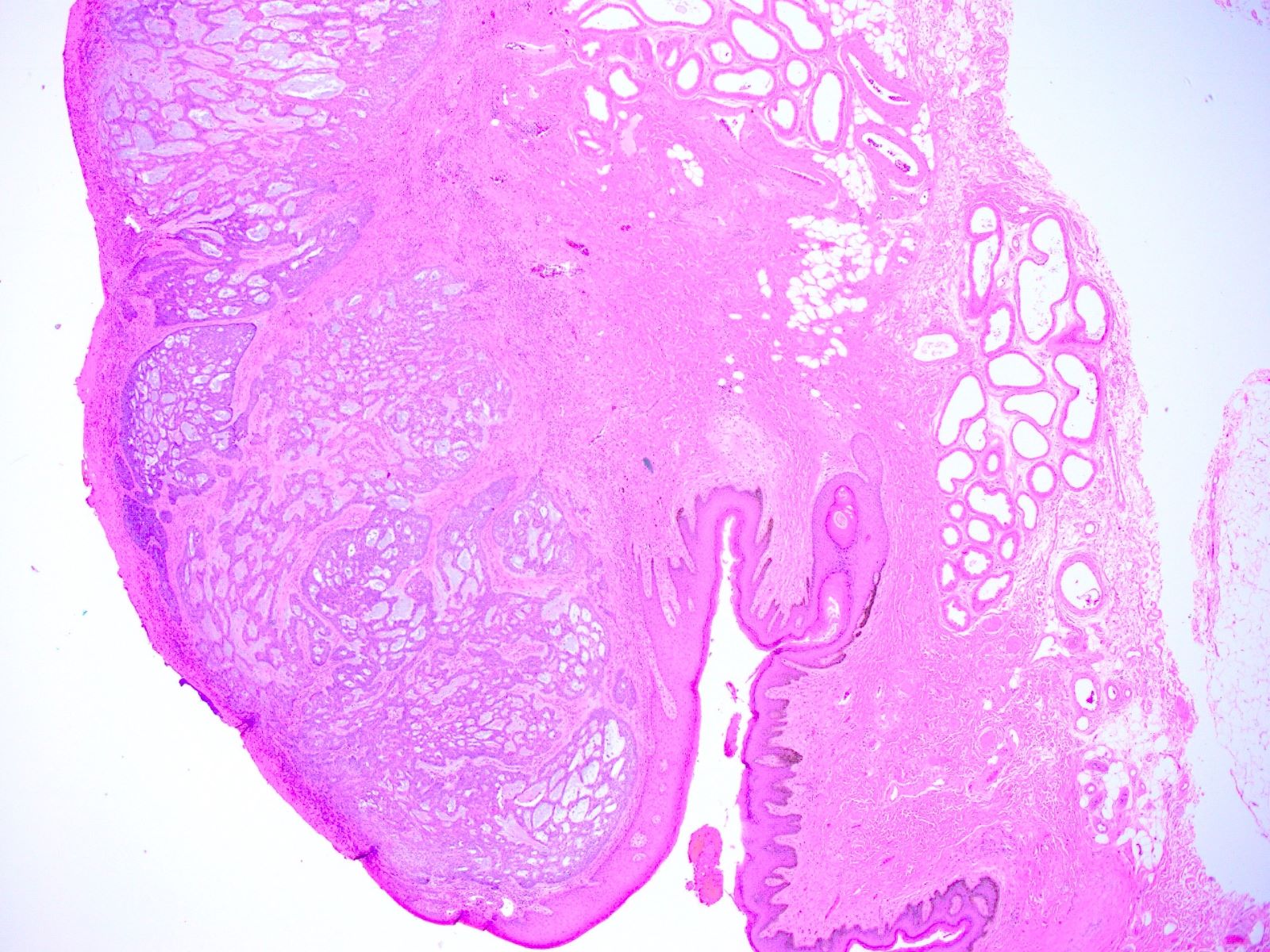
Nodular growth and cribriform tumor nests
Basaloid cells with mucin production
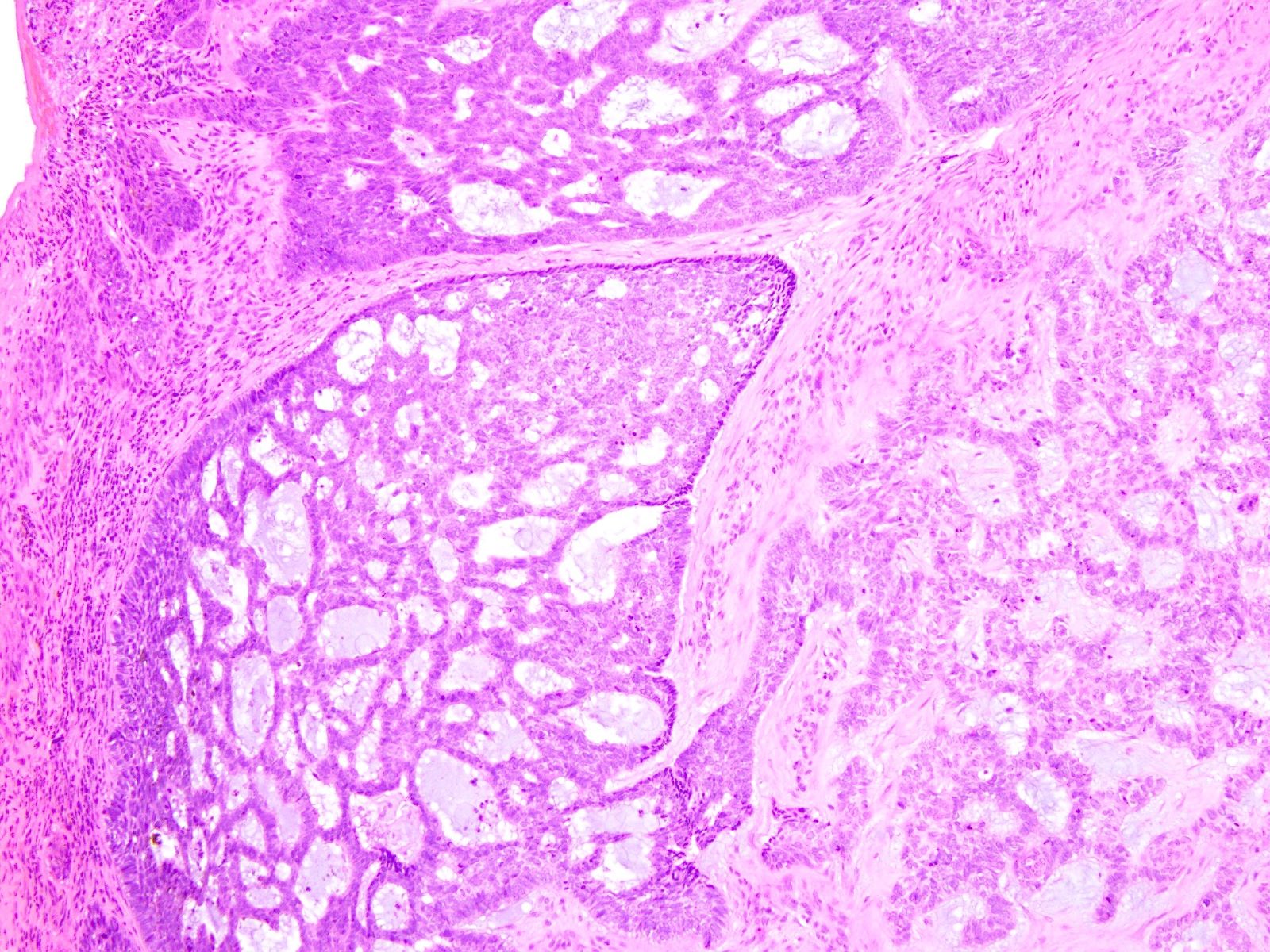
Retraction artifact
Basaloid lobules with palisading
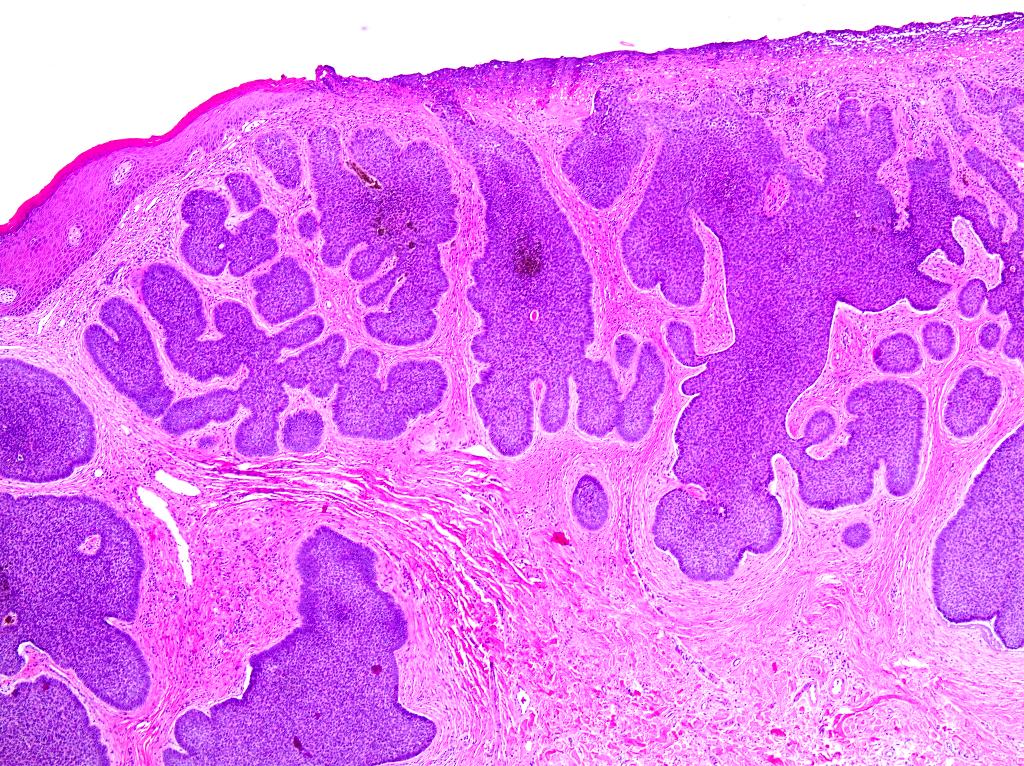
Cleft formation between basaloid tumor lobules & stroma

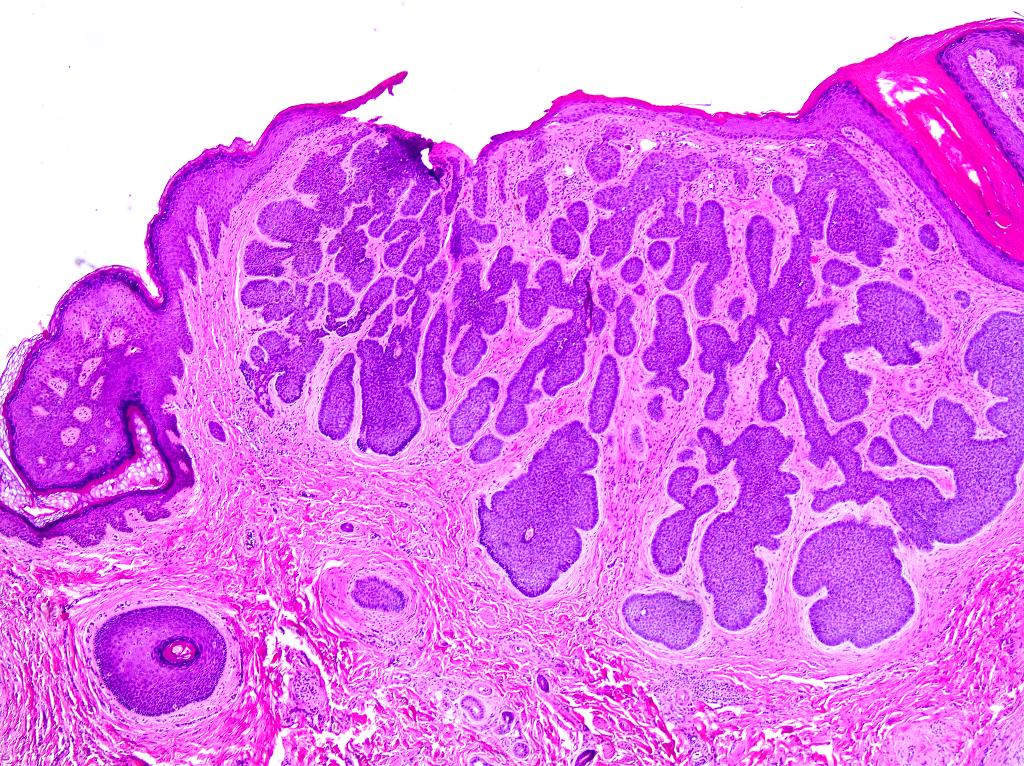
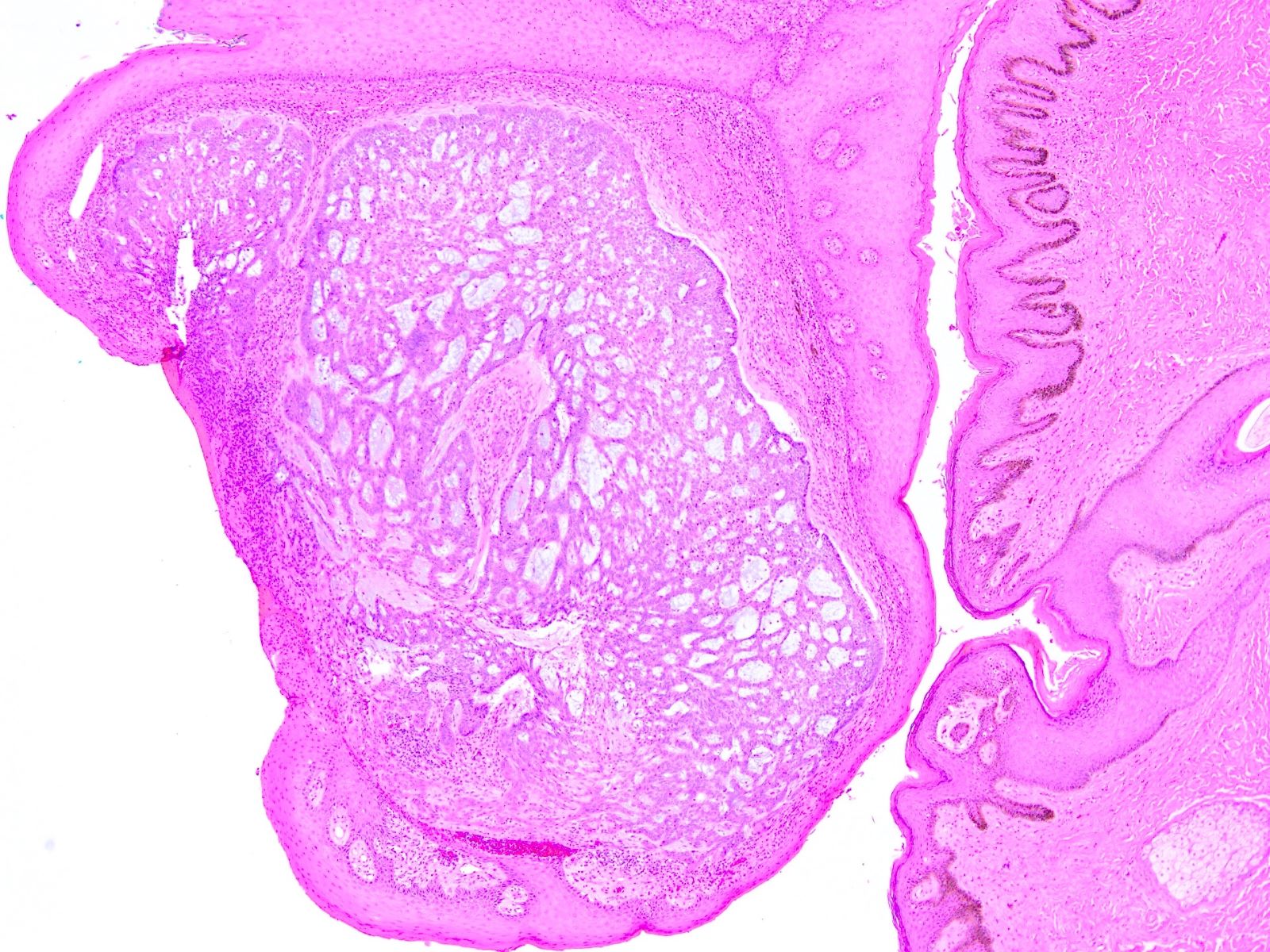
Basaloid lobules - conspicuous peripheral nuclear palisade

Cleft formation between basaloid tumor lobules & stroma
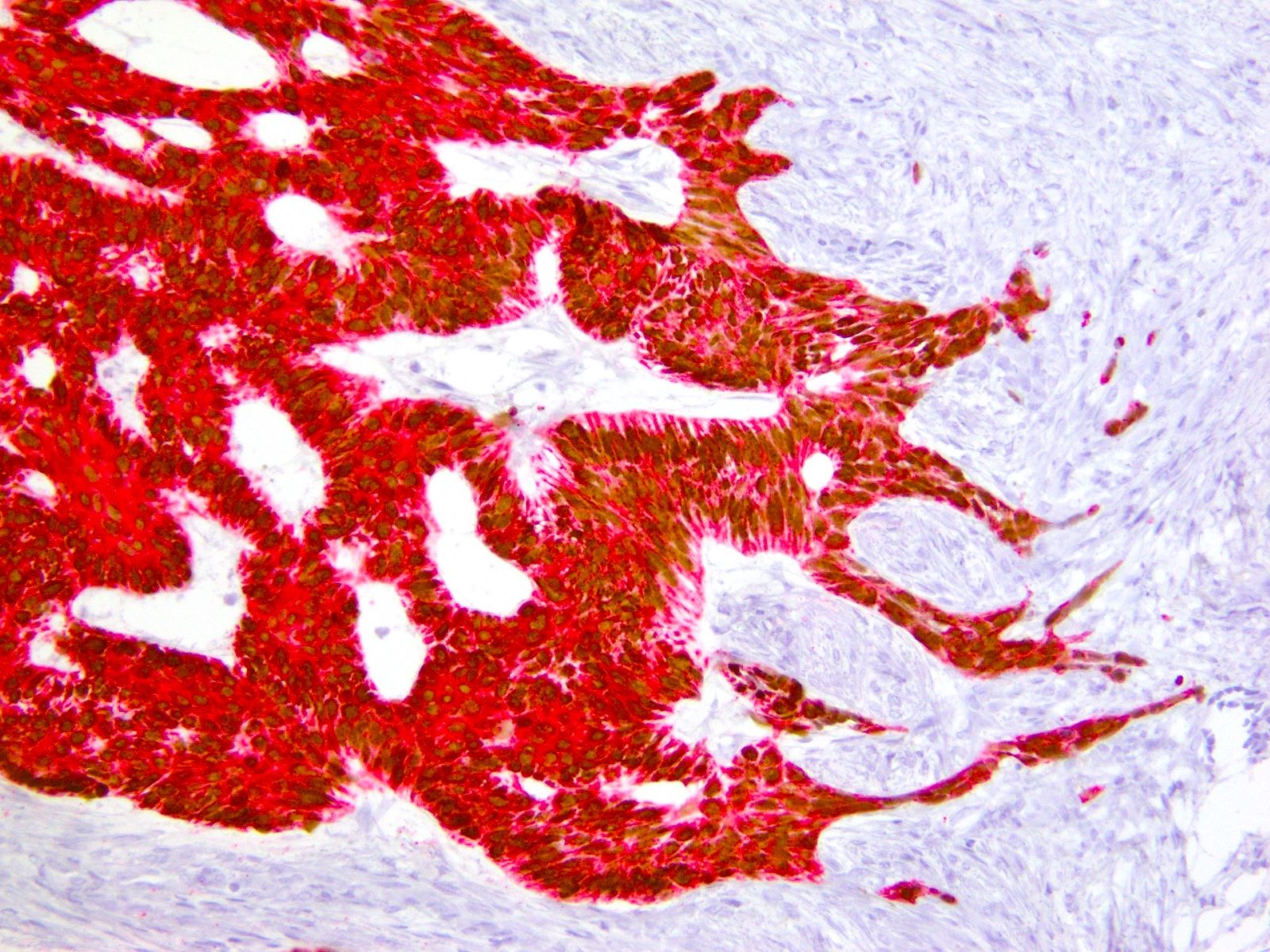
p40 - CK5/6 dual stain
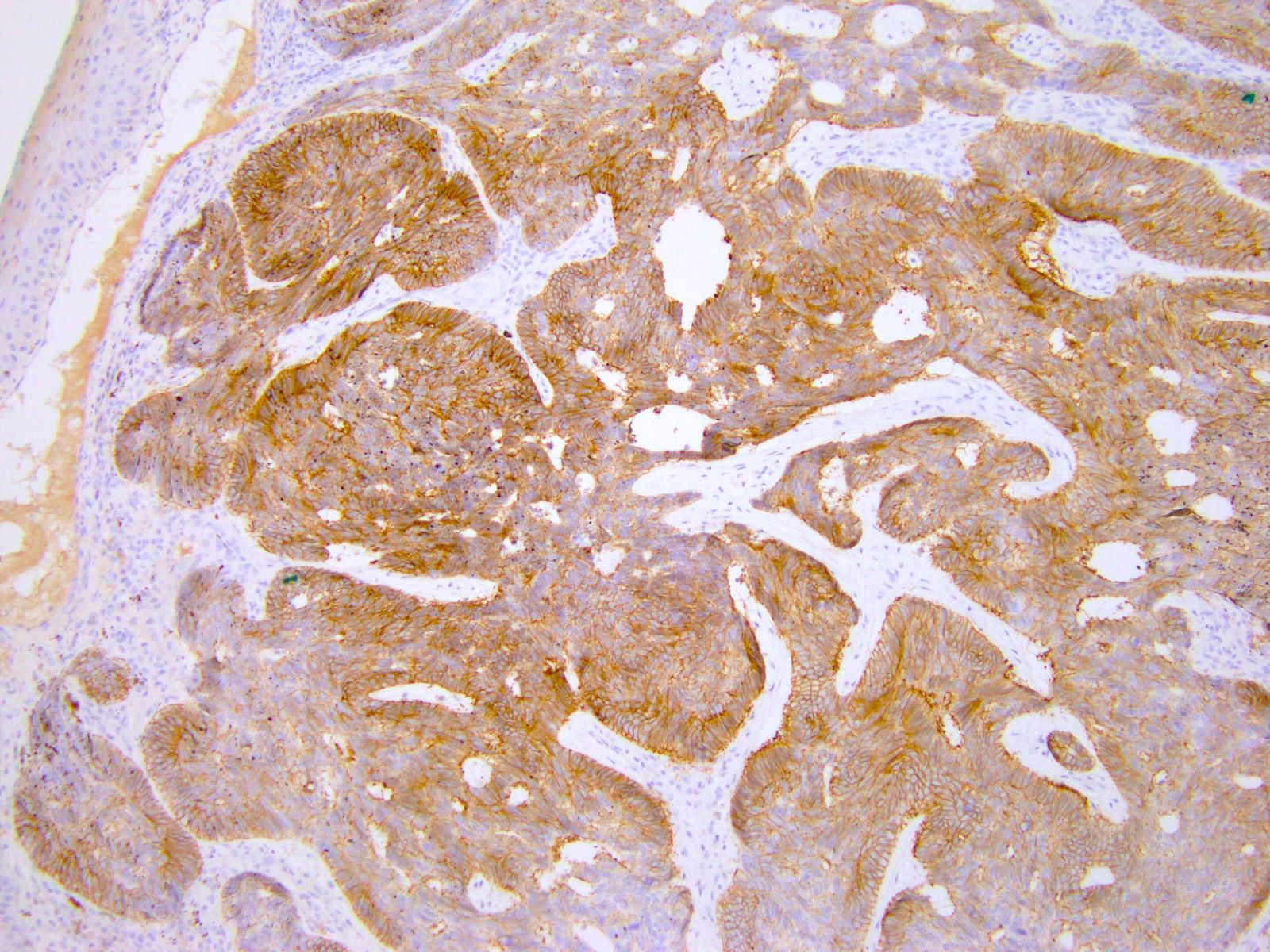
BerEP4
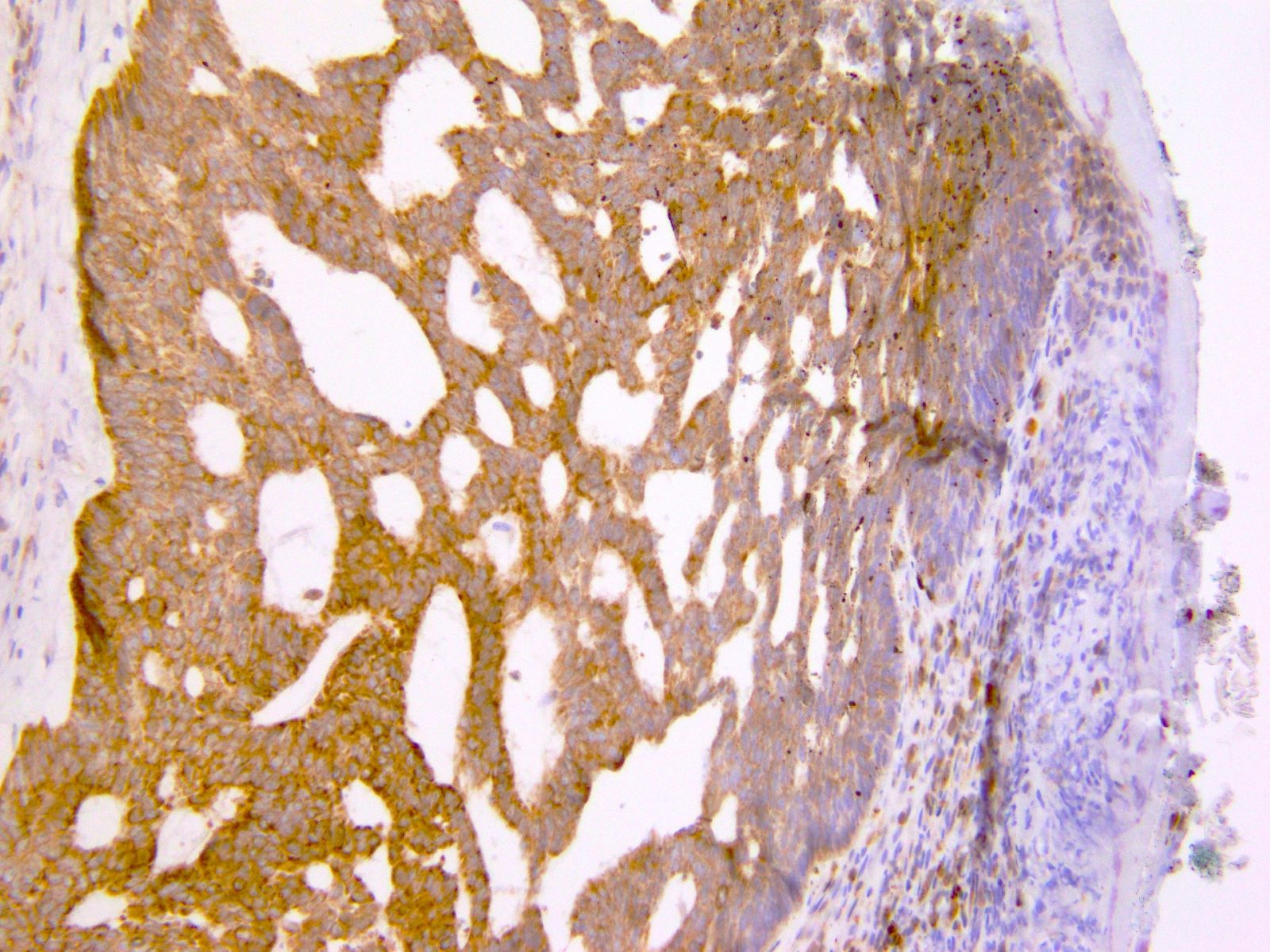
BCL2
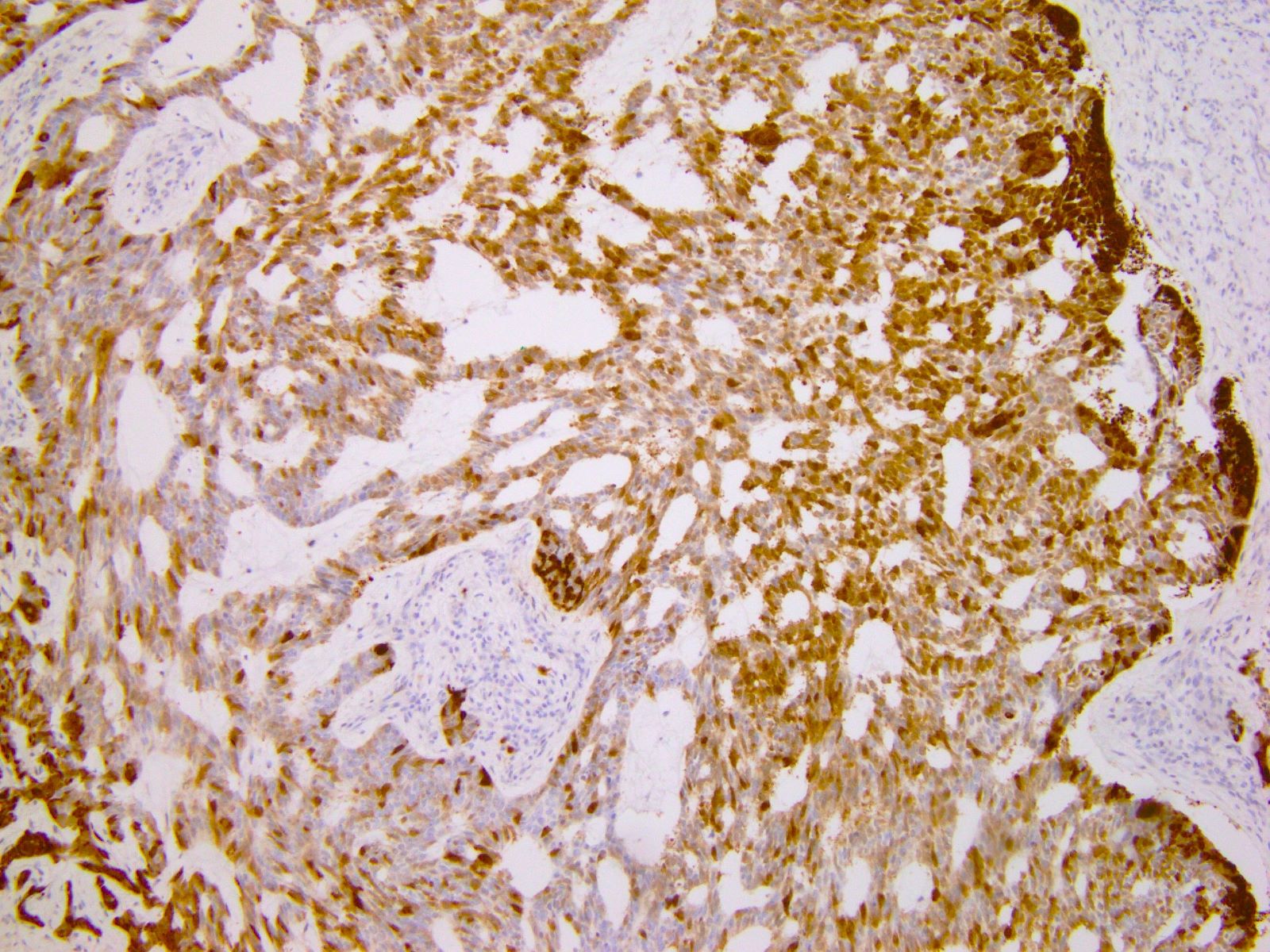
p16
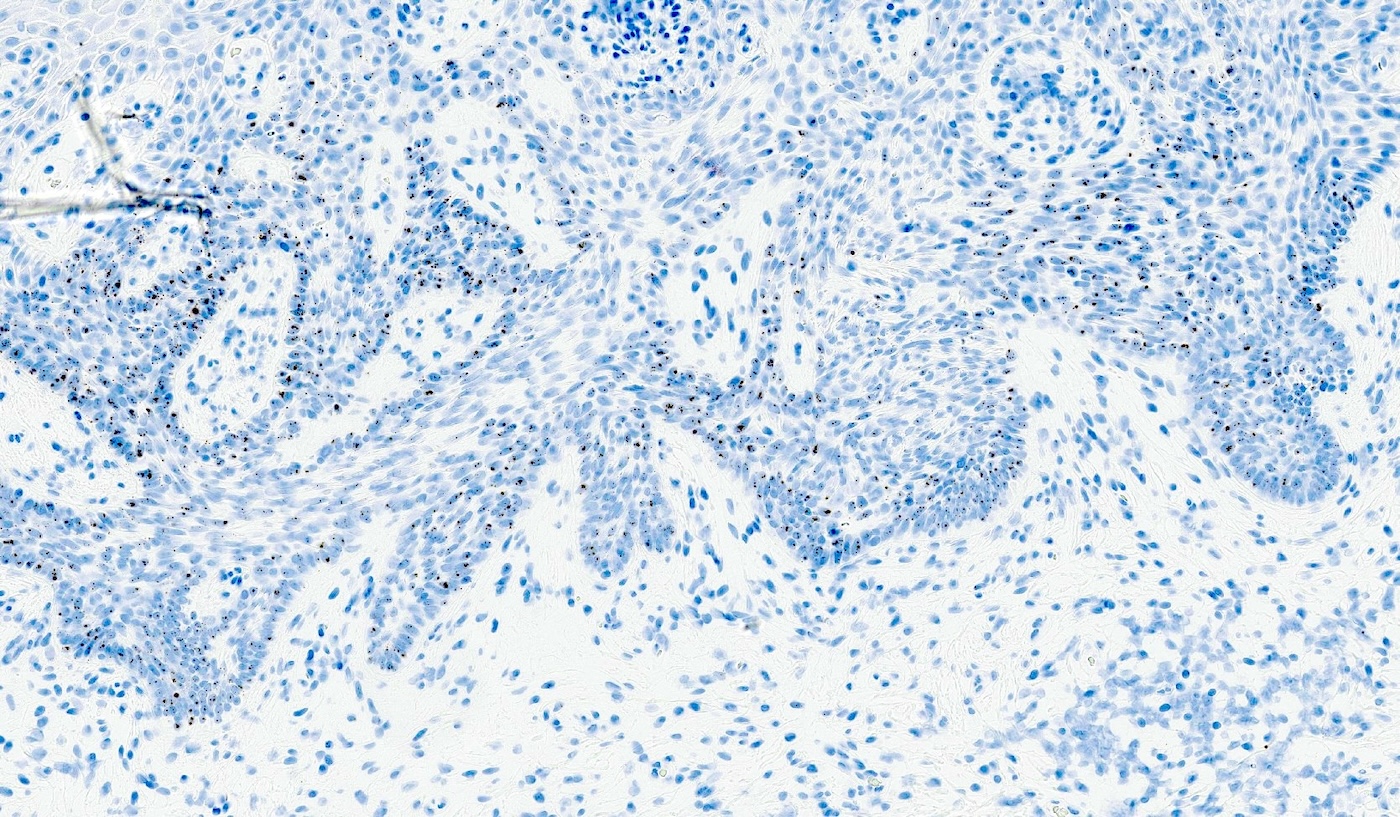
GLI1 ISH
Positive stains
- p40, p63, CK5/6
- BerEP4 (typically diffuse), BCL2 (diffuse), CD10 (tumor and stroma), AR (focal)
- CK7, CK19 (J Cutan Med Surg 2017;21:457)
- CD56 (95%), chromogranin A (28%), and synaptophysin (18%) (Med Oncol 2013;30:444, J Immunoassay Immunochem 2017;38:487)
- GLI1 ISH (Mod Pathol 2023;36:100265)
Negative stains
- EMA, CEA, CK20 (may be positive in colonizing Merkel cells)
- PHLDA1 (TDAG51) (J Cutan Pathol 2011;38:542)
- p16 (negative or patchy), high risk HPV in situ hybridization (Am J Surg Pathol 2014;38:542)
Molecular / cytogenetics description
- See Pathophysiology
Videos
BCC 101 by Dr. Jerad Gardner
Reporting BCC by Dr. Catriona McKenzie, pathCast
Sample pathology report
- Vulva, left (partial vulvectomy):
- Basal cell carcinoma, 1.3 cm
- Depth of invasion: 2 mm
- Margins are negative
Differential diagnosis
- Basaloid squamous cell carcinoma:
- Trichoepithelioma / trichoblastoma:
- Basaloid follicular neoplasm
- Presence of horn / keratin cysts and lack of retraction artifact
- CD10 expression limited to stroma
- PHLDA1 (TDAG51)+
- Merkel cell carcinoma:
- Typically no connection to overlying dermis
- Small, round, blue cell tumor with high N:C ratio, round nuclei, salt and pepper chromatin
- Conspicuous mitoses and apoptotic bodies
- CK20+, perinuclear dot-like staining
- Adenoid cystic carcinoma:
- More deeply situated; no connection to overlying epidermis
- Biphasic neoplasm with ductal and myoepithelial differentiation
- Characteristic cribriform, tubular and solid architectural patterns
- Cribriform spaces filled with basement-like material
- MYB:NFIB fusion
- Differentiated vulvar intraepithelial neoplasia:
- Differential diagnosis of superficial subtype of BCC
- Atypical cells confined to basal layer
- Large nuclei with vesicular chromatin, prominent nuclei
- Retained but abnormal maturation of epithelium
- Aberrant p53 expression
Additional references
Practice question #1
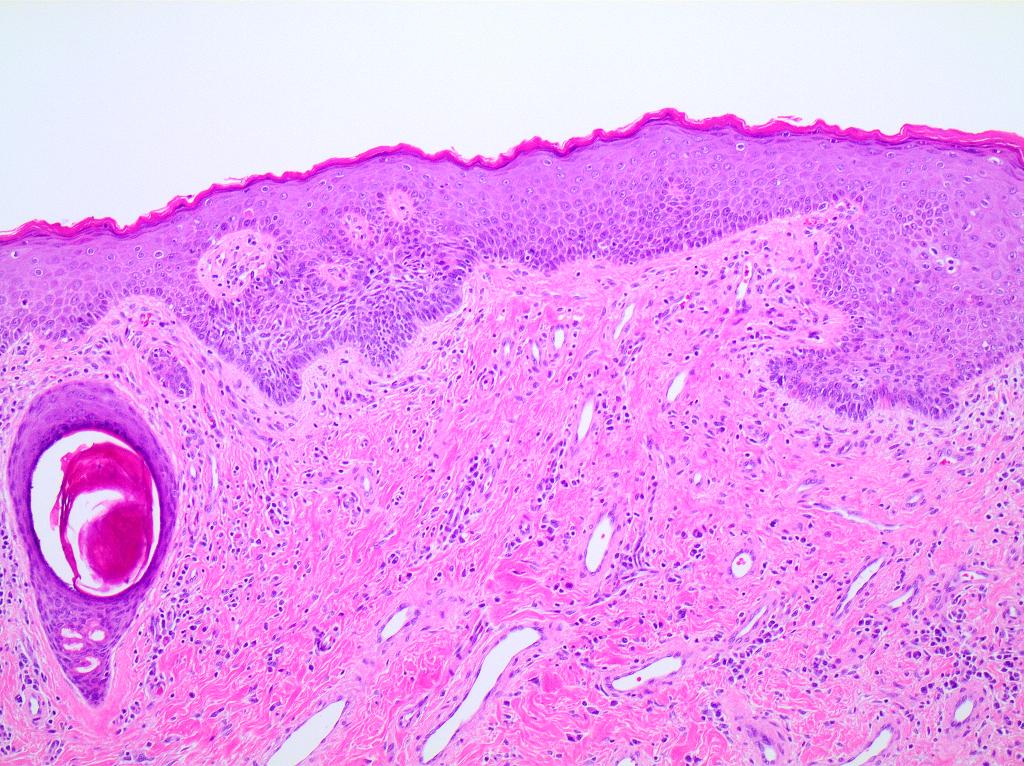
A 78 year old woman presents with a 2 cm pearly pink nodule in the right labium majus. Dermoscopy of the lesion reveals ovoid nests and arborizing fine blood vessels. A biopsy is performed and shows the image above. Which of the following is true?
- Genes usually mutated in this cancer include TP53 and NOTCH1
- Human papillomavirus (HPV) plays a major role in disease pathogenesis
- The tumor is also positive for CK20 perinuclear dot-like staining
- This neoplasm has a high rate of metastatic disease
Practice answer #1
A. Genes usually mutated in this cancer include TP53 and NOTCH1. TP53 and NOTCH1 are mutated in about half of basal cell carcinomas (BCCs). Answer D is incorrect because metastatic disease from BCC is rare. Answer B is incorrect because BCCs are HPV independent. Answer C is incorrect because the described staining pattern is seen in Merkel cell carcinomas.
Comment Here
Reference: Basal cell carcinoma-vulva
Comment Here
Reference: Basal cell carcinoma-vulva
Practice question #2
An 83 year old woman presents with a slightly erythematous and ulcerative lesion in the left vulva. A biopsy is performed and is positive for basal cell carcinoma. Which of the following immunohistochemical stains is positive in this tumor?
- BCL2
- CEA
- CK20
- EMA
Practice answer #2
A. BCL2. Basal cell carcinomas (BCCs) stain diffusely positive for BCL2. Answer D is incorrect because BCCs usually stain negative for EMA. Answer C is incorrect because BCCs usually stain negative for CK20. Answer B is incorrect because BCCs usually stain negative for CEA.
Comment Here
Reference: Basal cell carcinoma-vulva
Comment Here
Reference: Basal cell carcinoma-vulva
