Skin nonmelanocytic tumor
Carcinoma (nonadnexal)
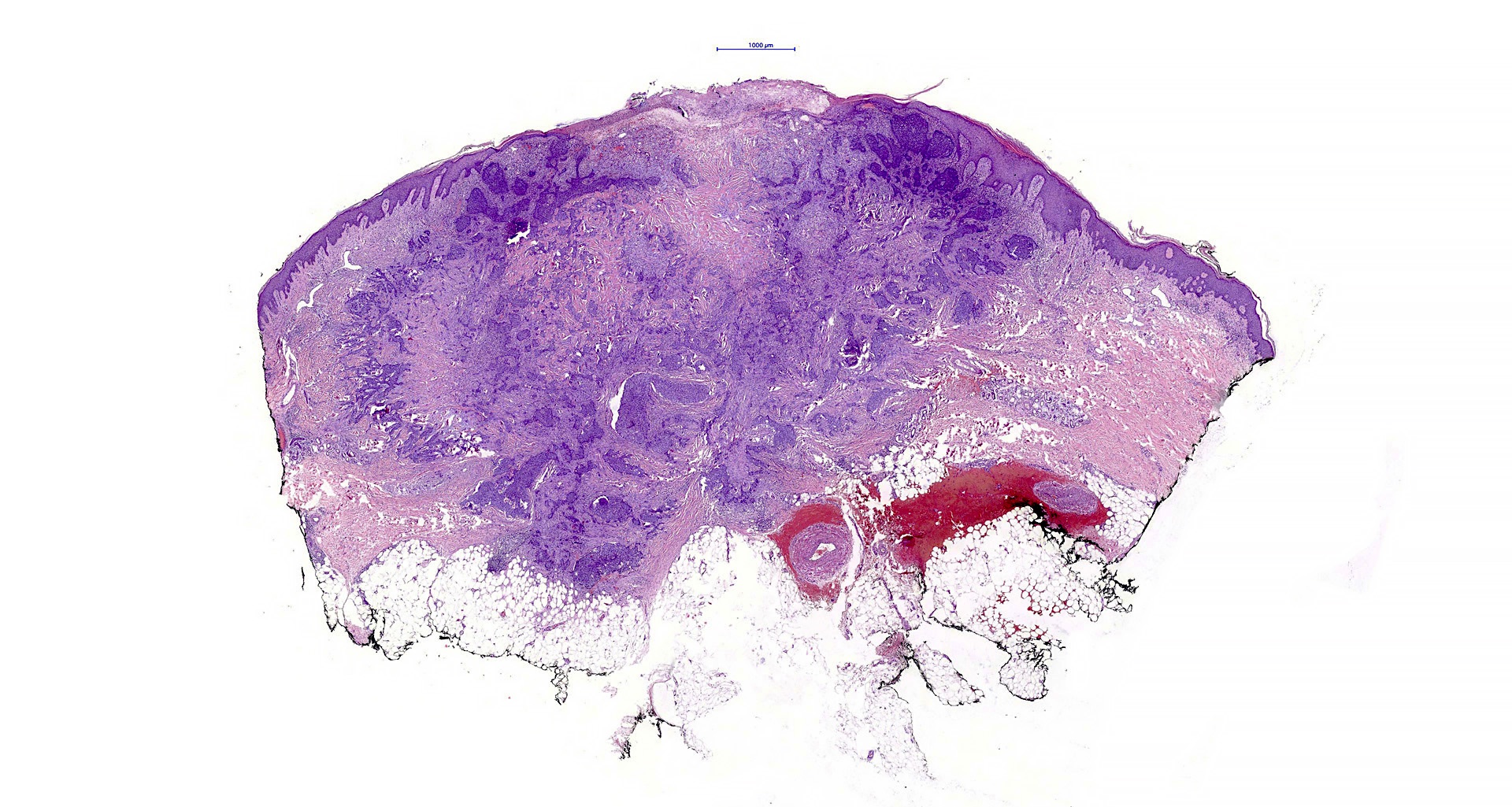
Basal cell carcinoma


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Basal cell carcinoma[TI] skin[TIAB] pathology review[PT] full text[SB]
- Basal cell carcinoma (BCC) arises from the interfollicular or follicular epithelium
- Most common malignant tumor type in humans
- Local aggressive course
- Low disease associated death rate; metastases to lung and bone exceptionally rare
- When multiple, associated with a number of genetic conditions, including basal cell nevus (Gorlin), Bazex-Dupré-Christol, Rombo syndromes and xeroderma pigmentosum
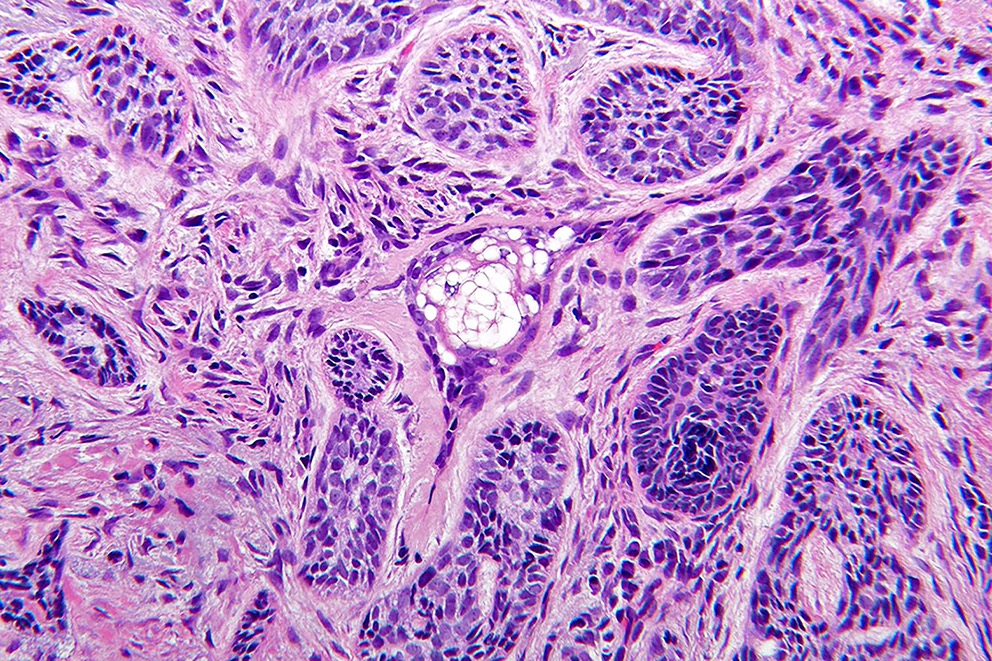
- Nests of basaloid cells with peripheral palisading associated with a fibromyxoid stroma
- Basal cell epithelioma
- Rodent ulcer
- Basalioma
- Fibroepithelioma of Pinkus
- ICD-O:
- 8090/3 - Basal cell carcinoma, NOS
- 8097/3 - Nodular basal cell carcinoma
- 8091/3 - Superficial basal cell carcinoma
- 8097/3 - Micronodular basal cell carcinoma
- 8092/3 - Infiltrating basal cell carcinoma
- 8092/3 - Morpheaform basal cell carcinoma
- 8094/3 - Basosquamous carcinoma
- 8090/3 - Pigmented basal cell carcinoma
- 8092/3 - Basal cell carcinoma with sarcomatoid differentiation (metaplastic BCC)
- 8090/3 - Basal cell carcinoma with adnexal differentiation
- 8093/3 - Fibroepithelial basal cell carcinoma
- N/A - Basomelanocytic tumor
- Most common cancer type in fair skinned people (Br J Dermatol 2017;177:359)
- Highest rate is observed in Australia (1,000/100,000 person years) (Br J Dermatol 2012;166:1069)
- More frequent:
- Middle aged adults with increasing incidence with age
- People with I - II Fitzpatrick skin phototype (Cancer Epidemiol 2013;37:534)
- Male (M:F = 1.5:1)
- Number of cases is increasing every year worldwide, especially among young age group, with a predilection for women (Br J Dermatol 2012;166:1069, Pediatrics 2014;134:e4)
- Tumors that occur in younger age group tend to behave in an aggressive fashion (Br J Plast Surg 2000;53:393)
- Sun exposed skin (G Ital Dermatol Venereol 2014;149:423)
- 64% on the head region (most often nodular variant)
- 24% on the trunk (most often superficial variant)
- Rare areas such as anogenital region, nail unit, palm and sole (J Cutan Pathol 2018 Jun 19 [Epub ahead of print])
- UV radiation induced carcinogenesis
- Mutations in TP53 gene
- PTCH1 gene mutations
- Activating mutations in SMO gene
- Other genes including mutations in the CDKN2A gene and RAS genes
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
- UV radiation (sun damage and indoor tanning) (Cancer 1990;65:2811, Am J Epidemiol 1999;150:459, Pediatrics 2014;134:e4)
- Ionizing radiation (J Natl Cancer Inst 1996;88:1848)
- Arsenic exposure (J Dermatol 2017;44:1374)
- Genetic conditions
- Nevoid basal cell carcinoma syndrome (Gorlin syndrome) (Lancet 1992;339:581)
- Xeroderma pigmentosum (J Invest Dermatol 2012;132:785)
- Bazex-Dupré-Christol syndrome (NIH: Bazex-Dupre-Christol syndrome [Accessed 15 December 2020])
- Oculocutaneous albinism (BMC Cancer 2014;14:157)
- Muir-Torre syndrome
- Smoking (J Am Acad Dermatol 2002;46:706)
- Nevus sebaceus (J Am Acad Dermatol 2000;42:263)
- Immunosuppression (Lancet 1998;351:623, J Am Acad Dermatol 2003;49:397, Arch Dermatol 2001;137:459)
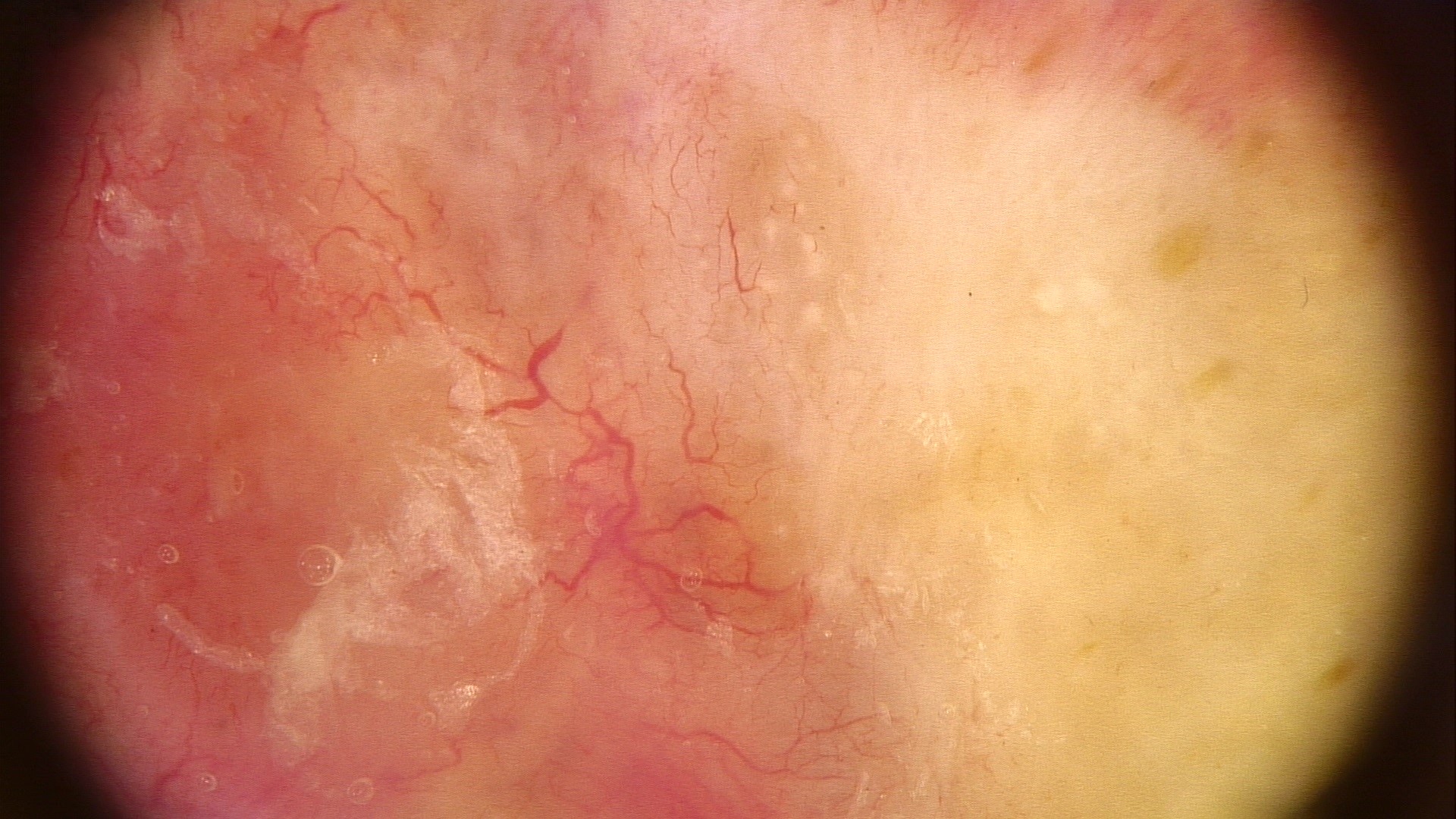
- Nodular variant usually presents as a pearly pink or flesh colored papule or nodule with arborizing and branching vessels (Br J Dermatol 2002;147:41)
- In the past, ulceration of a nodular BCC gave rise to the term rodent ulcer
- Tumor with ulceration has characteristic rolled borders
- Superficial variant presents with scaly macules, patches or plaques with an erythematous surface
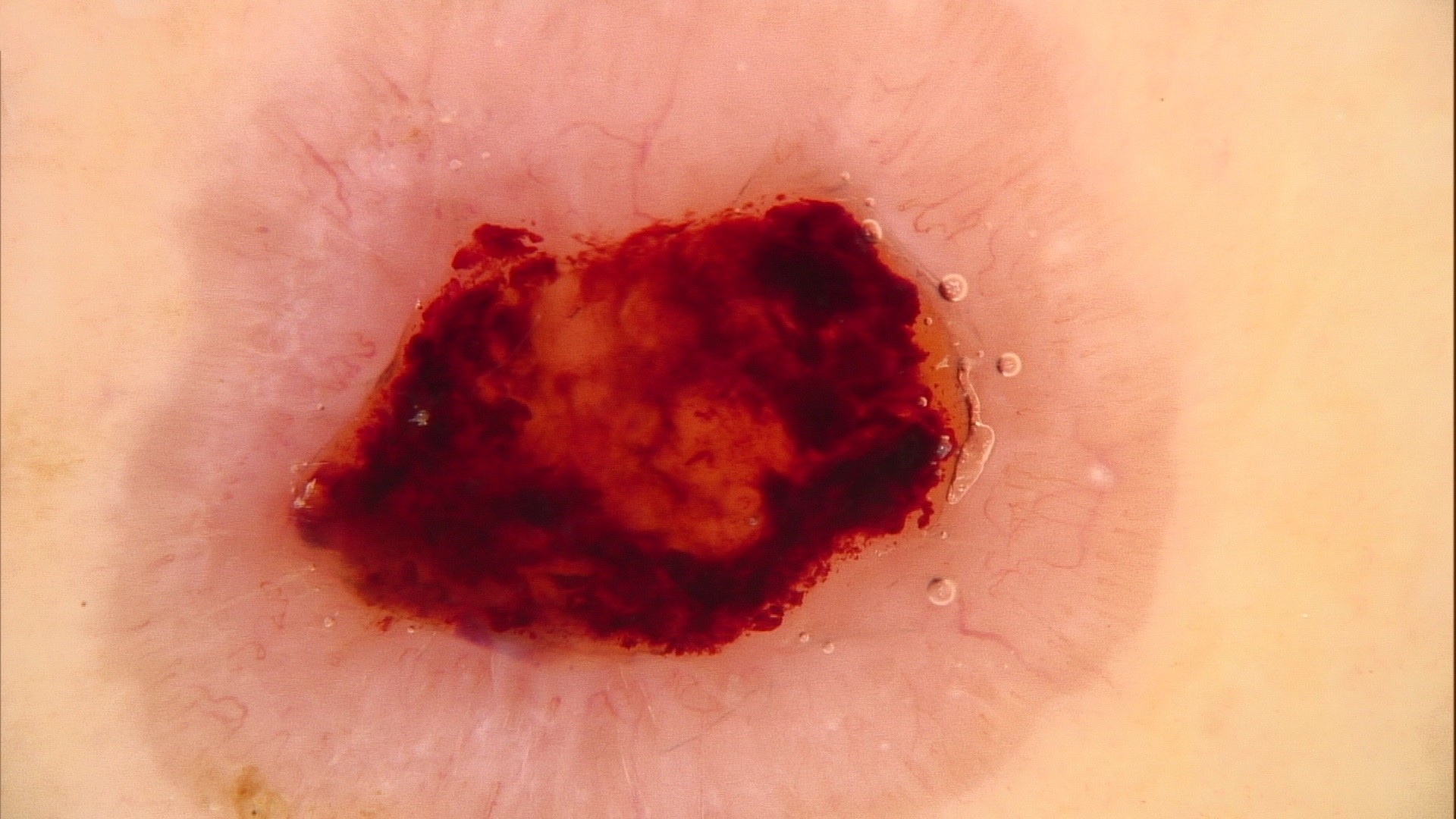
- Pigmented variant resembles a nodular or superficial BCC but has a pigmented surface and can be clinically mistaken for a melanoma
- Neglected tumors may result in massive skin, soft tissue and bone destruction with severe disfiguration
- Clinical features
- Dermatoscopy
- Histological features
- Histological type associated with risk of local recurrence
- Lower risk: nodular, superficial, pigmented, infundibulocystic, fibroepithelial
- Higher risk: basosquamous, sclerosing / morpheaform, keloidal, infiltrating, BCC with sarcomatoid differentiation and micronodular variants
- Circumscription of tumor margins
- Presence of perineural and lymphovascular invasion
- Status of surgical margins
- Tumor size
- Localization (part of skin affected, e.g. head and neck, trunk, etc.)
- History of nonmelanoma skin cancer
- Radiation therapy
- PUVA therapy
- Immunosuppression
- Reference: NCCN: Basal Cell Skin Cancer Evidence Blocks [Accessed 15 December 2020]
- 55 year old Caucasian man with BCC on the left forearm presenting with ulcerative axillary lymph node and pulmonary metastases (Case Rep Oncol Med 2018;2018:3485326)
- 65 year old man with clear cell BCC on upper chest (Patholog Res Int 2011;2011:386921)
- 65 year old man with neglected BCC on posterior neck presenting with diffuse skeletal metastases (JAAD Case Rep 2018;4:678)
- 76 year old Caucasian man with basosquamous carcinoma with lymphovascular invasion on left lateral shoulder (Cureus 2018;10:e3401)
- 79 year old woman with massive basosquamous carcinoma of back (Oxf Med Case Reports 2017;2017:omw095)
- 90 year old woman with infiltrative BCC on left shin that was clinically diagnosed as tinea corporis (Dermatol Online J 2018;24:13030)
- Surgery
- Mohs micrographic surgery
- Curettage and electrodesiccation for tumors with lower risk of local recurrence
- Radiation therapy
- Topical treatment (5-fluorouracil, imiquimod)
- Photodynamic therapy with aminolevulinic acid or porfimer sodium
- Nicotinamide (can be used for prophylactic treatment)
- Systemic therapy (sonidegib and vismodegib are hedgehog pathway inhibitors [HhIs])
- Reference: NCCN: Basal Cell Skin Cancer Evidence Blocks [Accessed 15 December 2020]
Contributed by Sergiy Vasylenko, M.D., Bohdan Lytvynenko, M.D. and Arghya Banerjee, M.D.

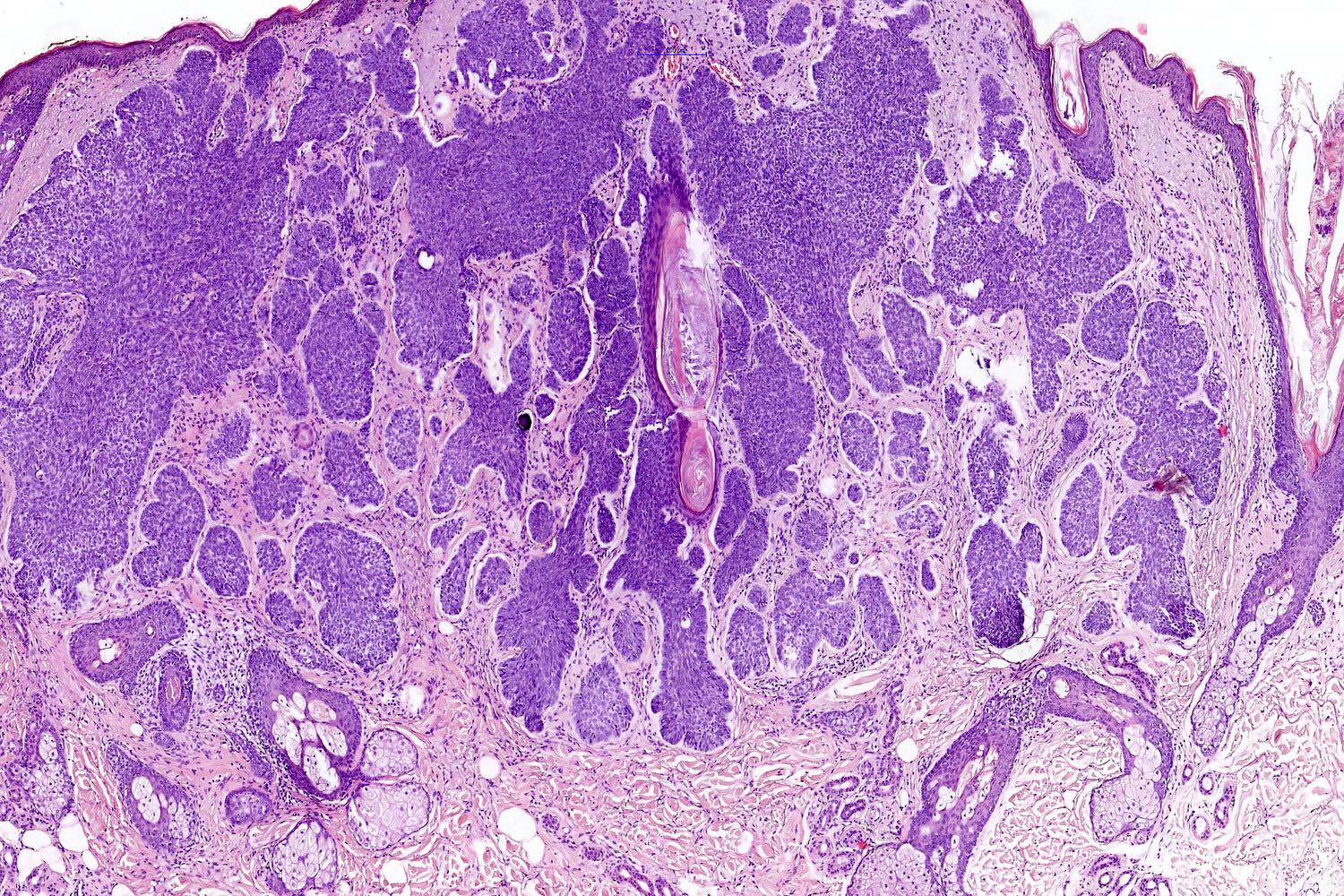
Nodular BCC

Ulcerative BCC

Pigmented, ulcerated BCC


Superficial BCC


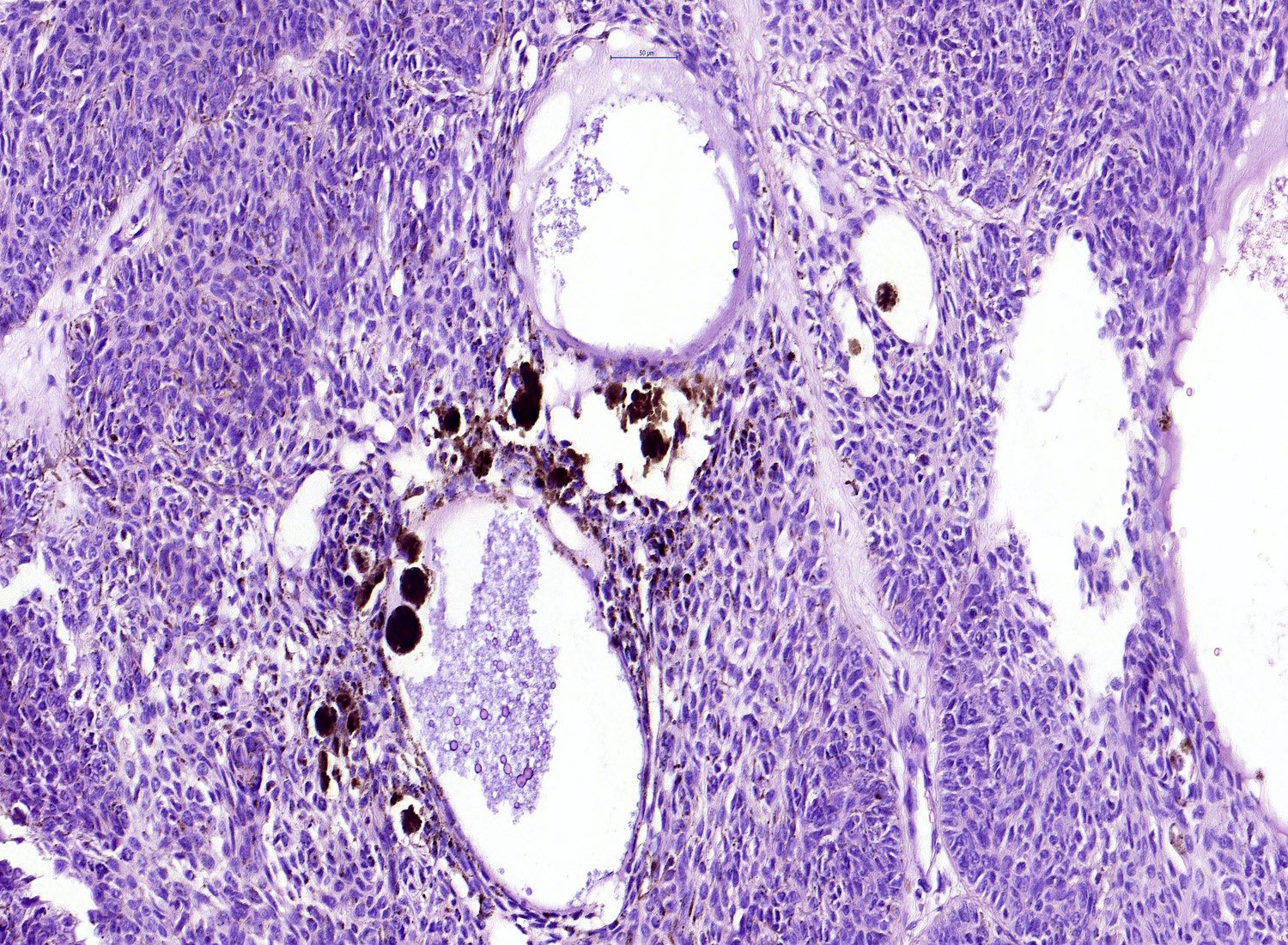
Pigmented BCC

Infiltrative BCC
- Variable, mirroring the clinical variants described above
- Mohs micrographic surgery technique is one of the most often used options for assessment of margins of surgery specimens (Dermatol Surg 2019;45:S57)
- Mohs surgery shows excellent 5 year cure rates: primary 99%, recurrent 94.4% (J Dermatol Surg Oncol 1989;15:315)
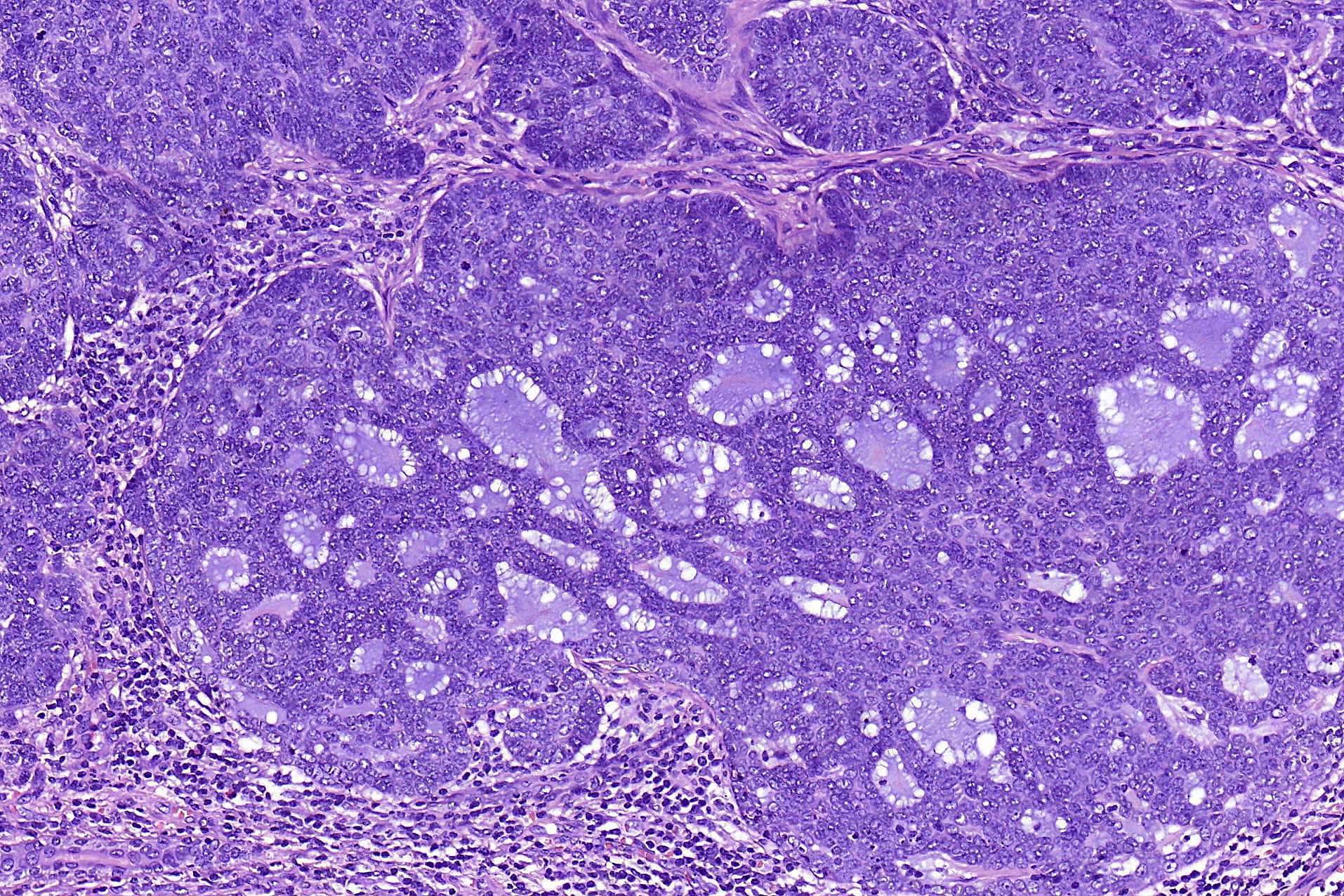
- Nodular and nodulocystic BCC
- Relatively circumscribed mass
- Epidermal or follicular attachment variably present
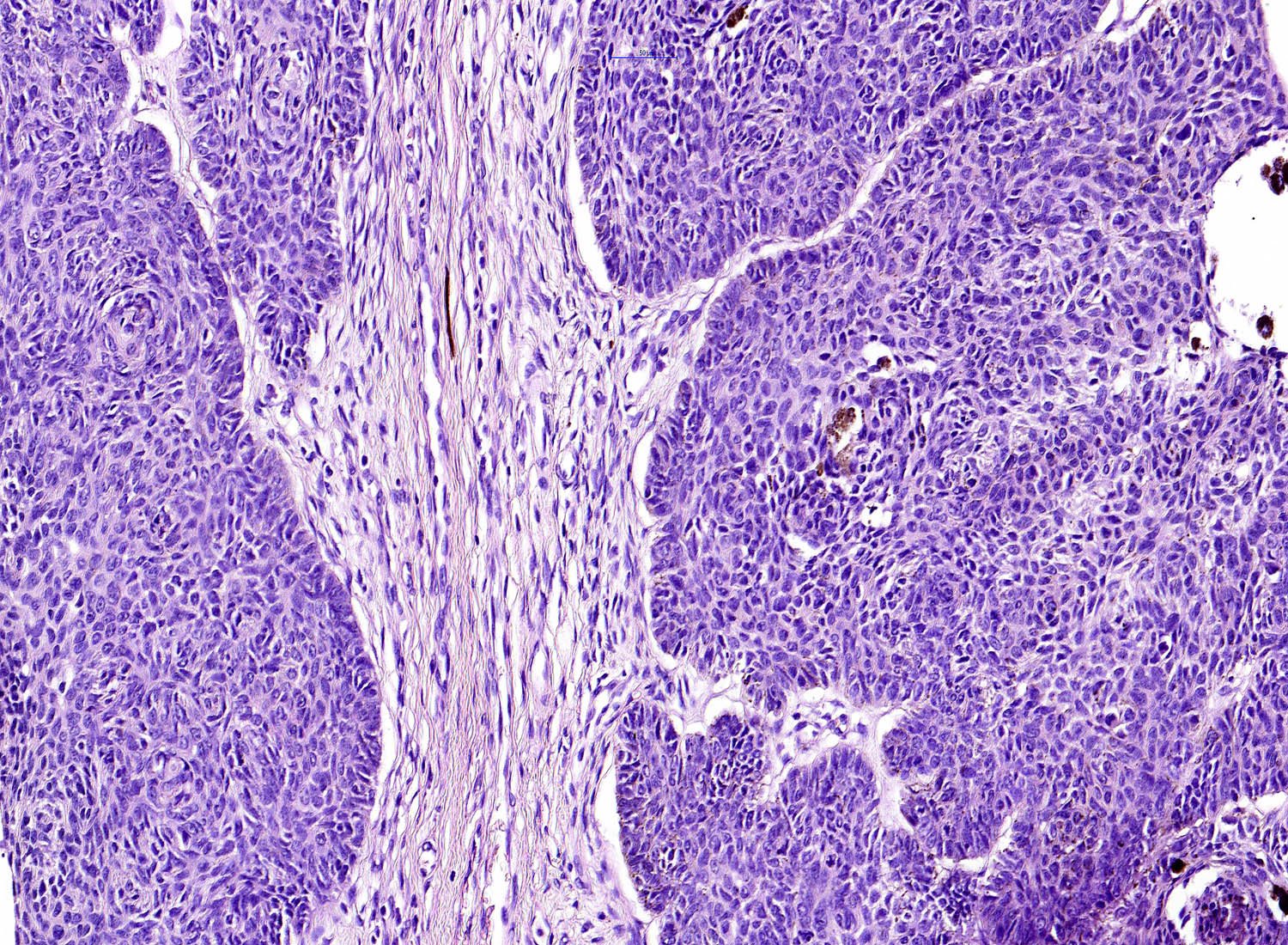
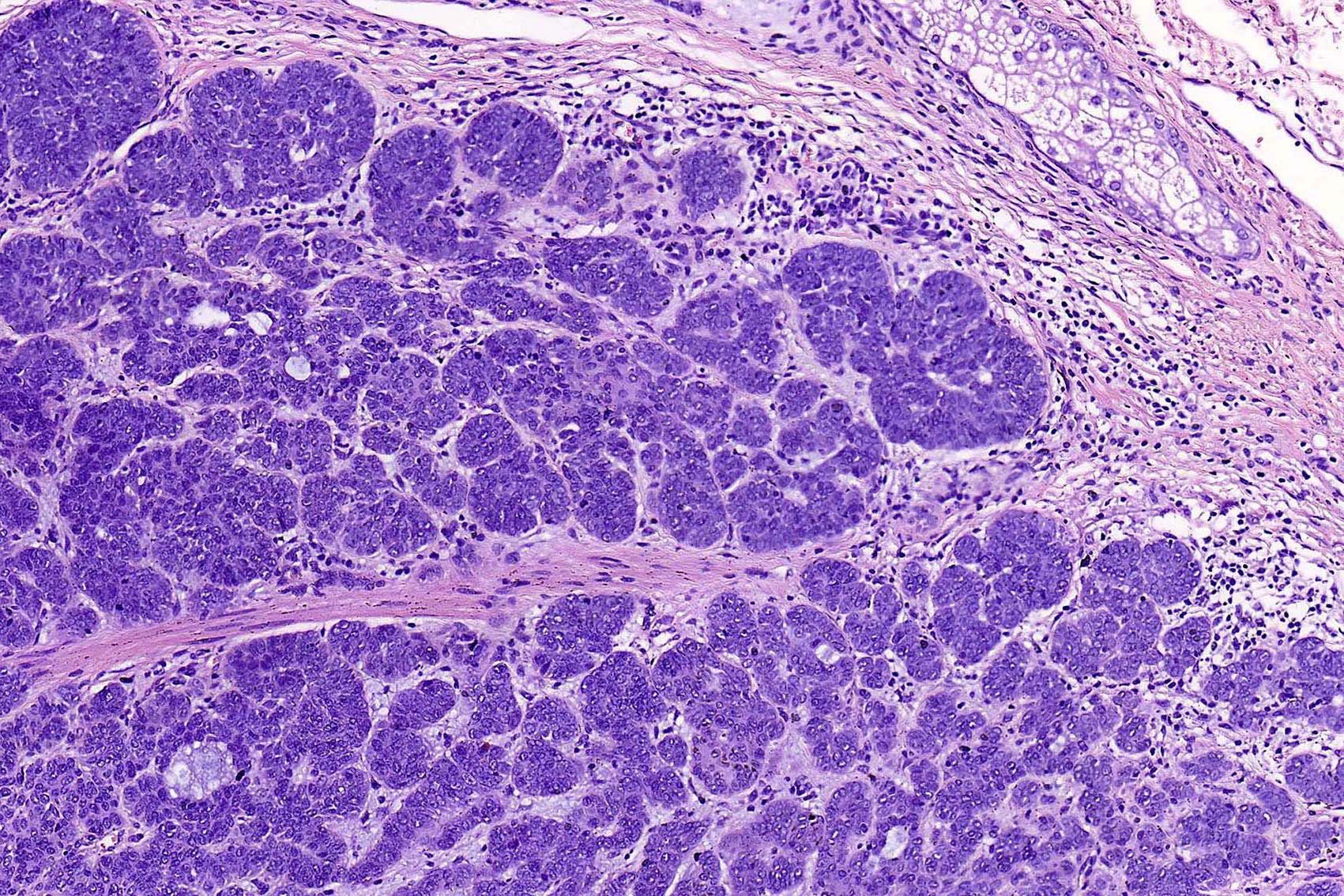
- Large basaloid lobules with peripheral nuclear palisade
- Lobules may be solid or show central cyst formation due to excessive mucin production
- Fibromyxoid stroma
- Cleft formation between tumor lobules and stroma
- Pleomorphism is generally mild
- Variable mitotic activity and apoptosis
- Sometimes necrosis en masse
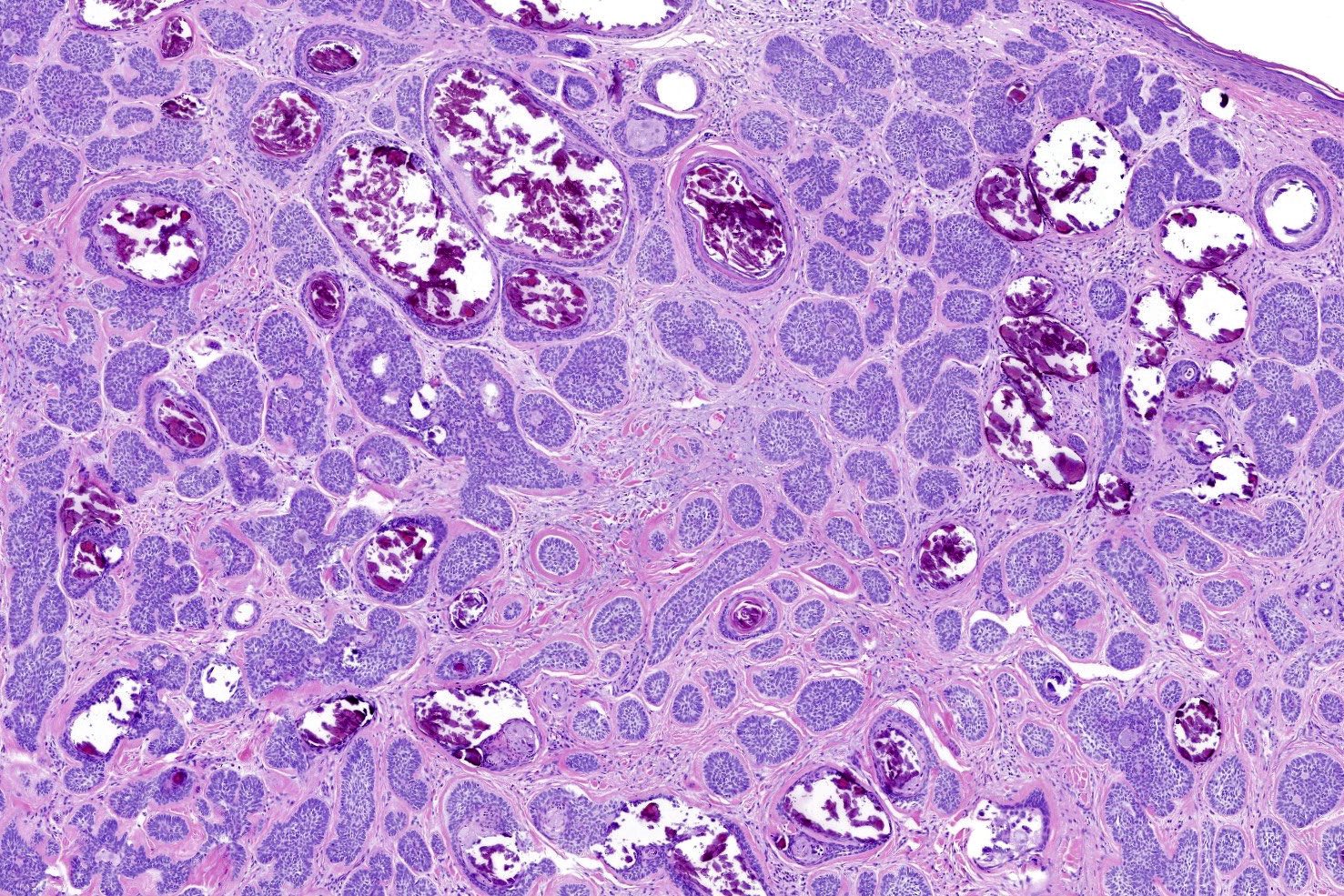
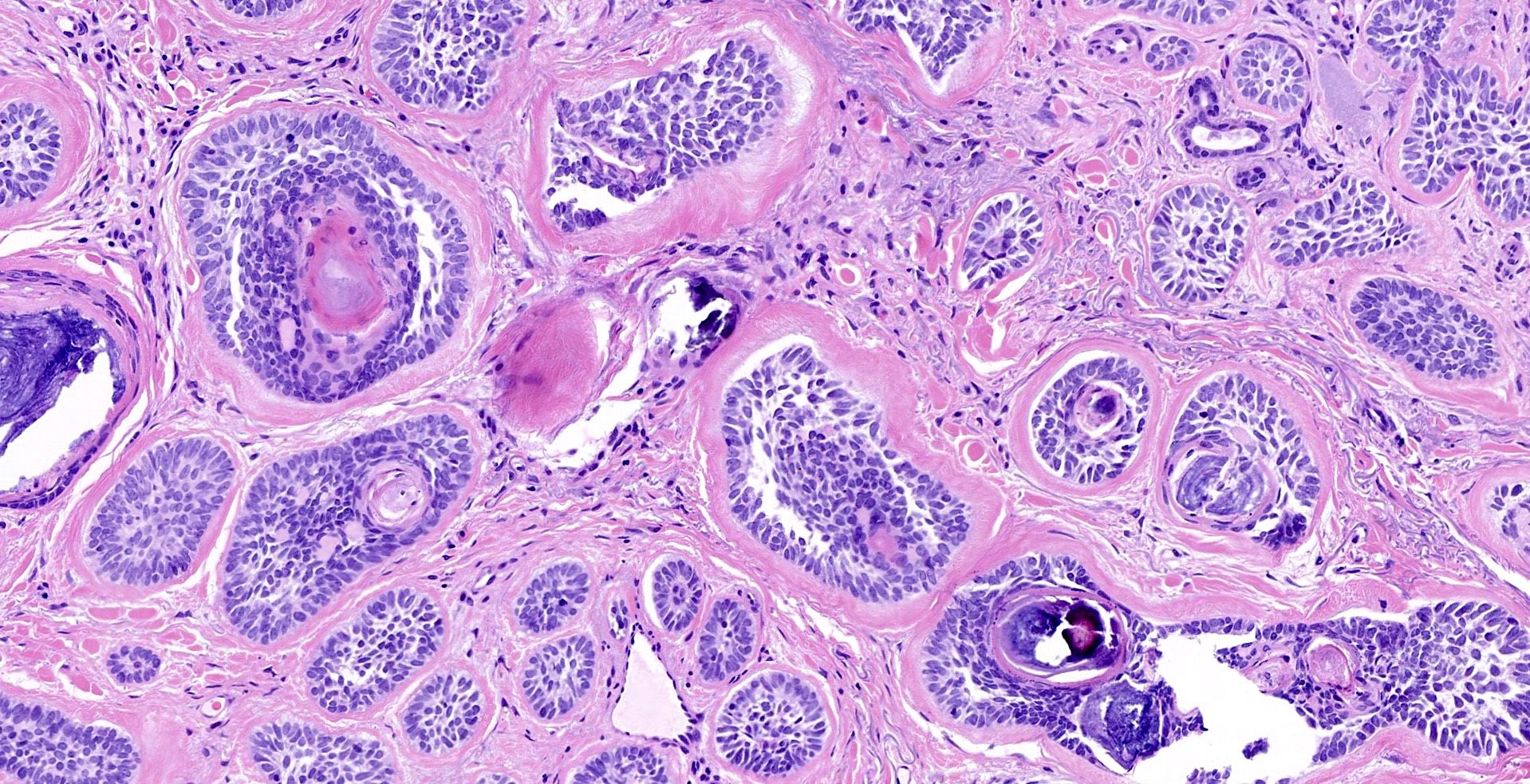
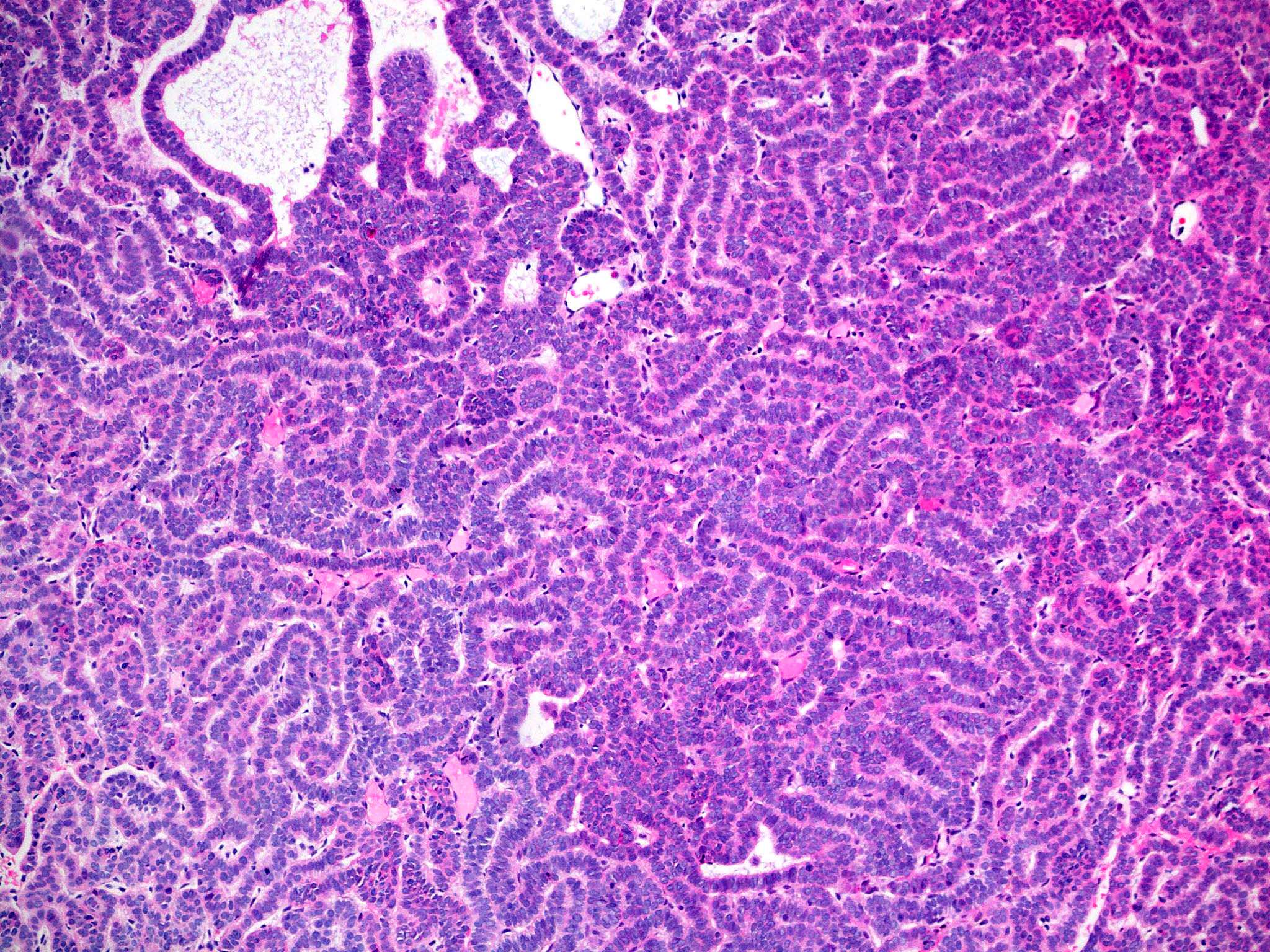
- Adenoid BCC
- Reticulate pseudoglandular pattern of basaloid cells
- Mucinous stroma
- Can mimic true gland formation, resulting in diagnostic confusion with a sweat gland adenocarcinoma, e.g. adenoid cystic carcinoma
- Micronodular BCC
- Small basaloid nests
- Peripheral palisading less prominent
- Retraction artifact usually absent
- Can diffusely infiltrate the dermis and extend into the subcutis
- Infiltrative BCC
- Small irregular clumps of basaloid cells
- Limited peripheral palisading
- Stroma loose and mucin may be prominent
- Extensive spread
- Perineural invasion can be seen
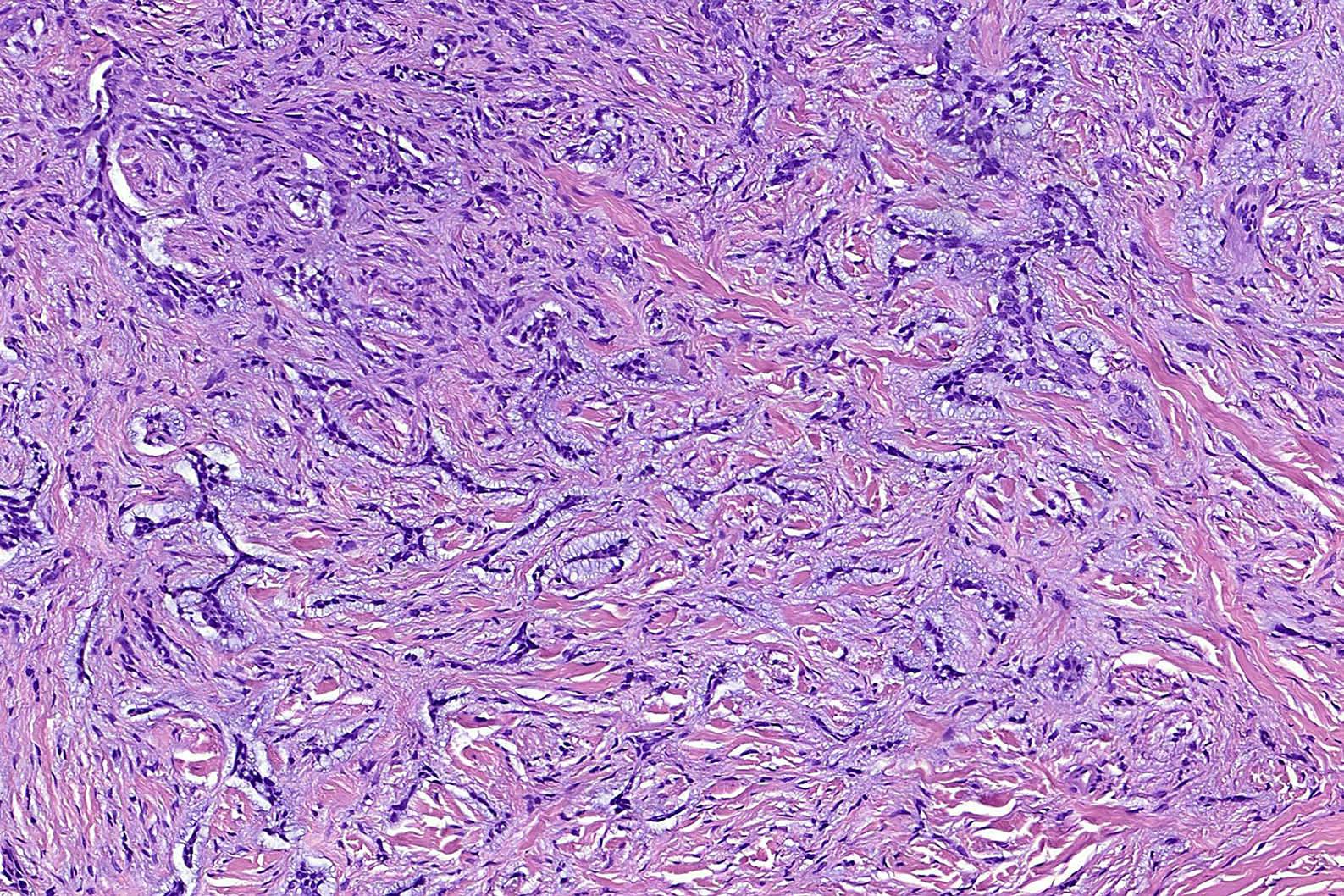
- Morpheaform (sclerosing, morphoeic) BCC
- Thin strands and nests of basaloid cells
- Limited peripheral palisading
- Stroma is dense and sclerotic
- Extensive spread
- Perineural invasion can be seen
- Keratotic BCC
- Horn cyst formation
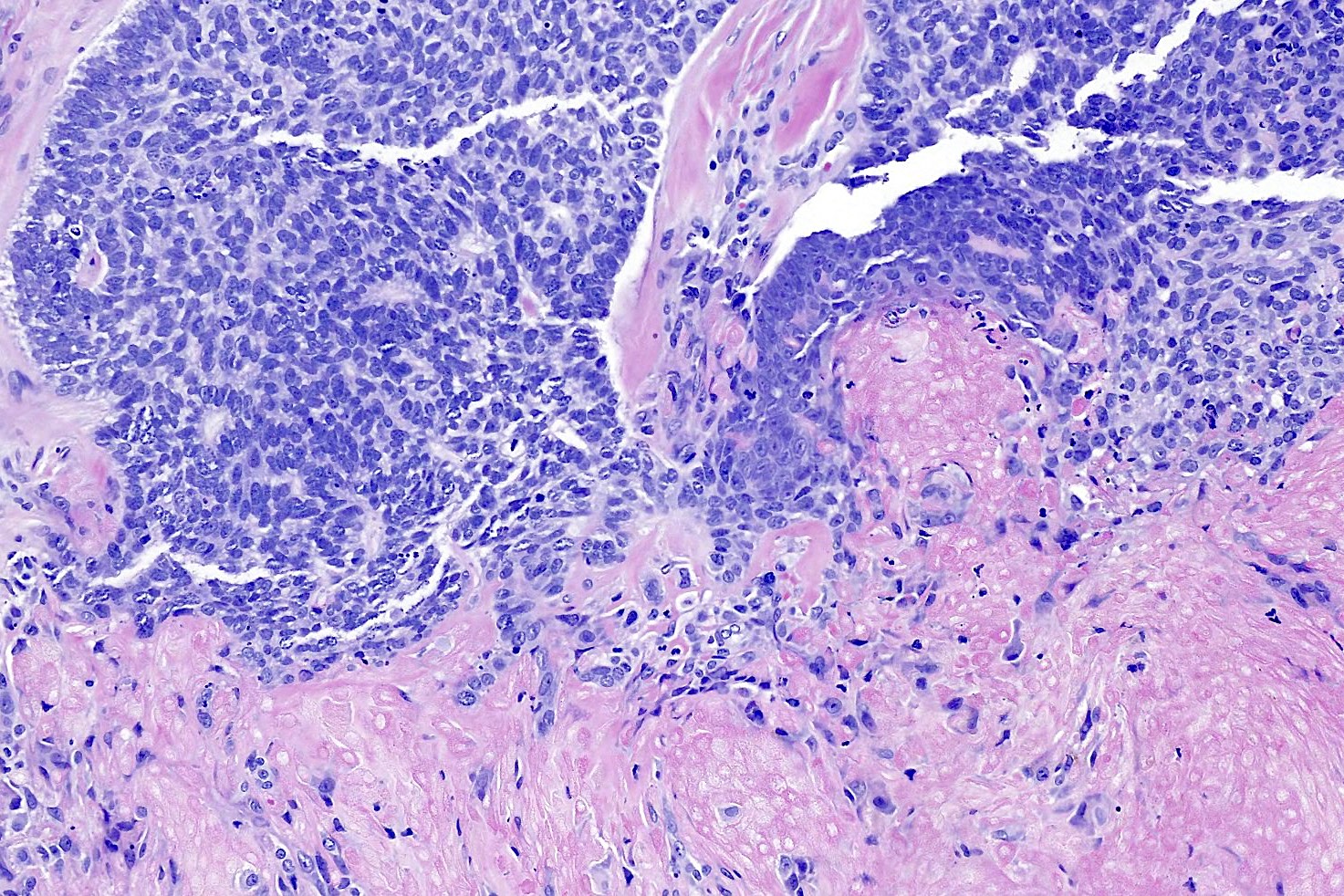
- Basosquamous (metatypical) BCC
- Biphasic tumor
- Foci of neoplastic squamous differentiation
- Pigmented BCC
- Nodular and superficial variants can be pigmented
- Colonization of tumor's complexes with melanocytes
- Stromal melanophages
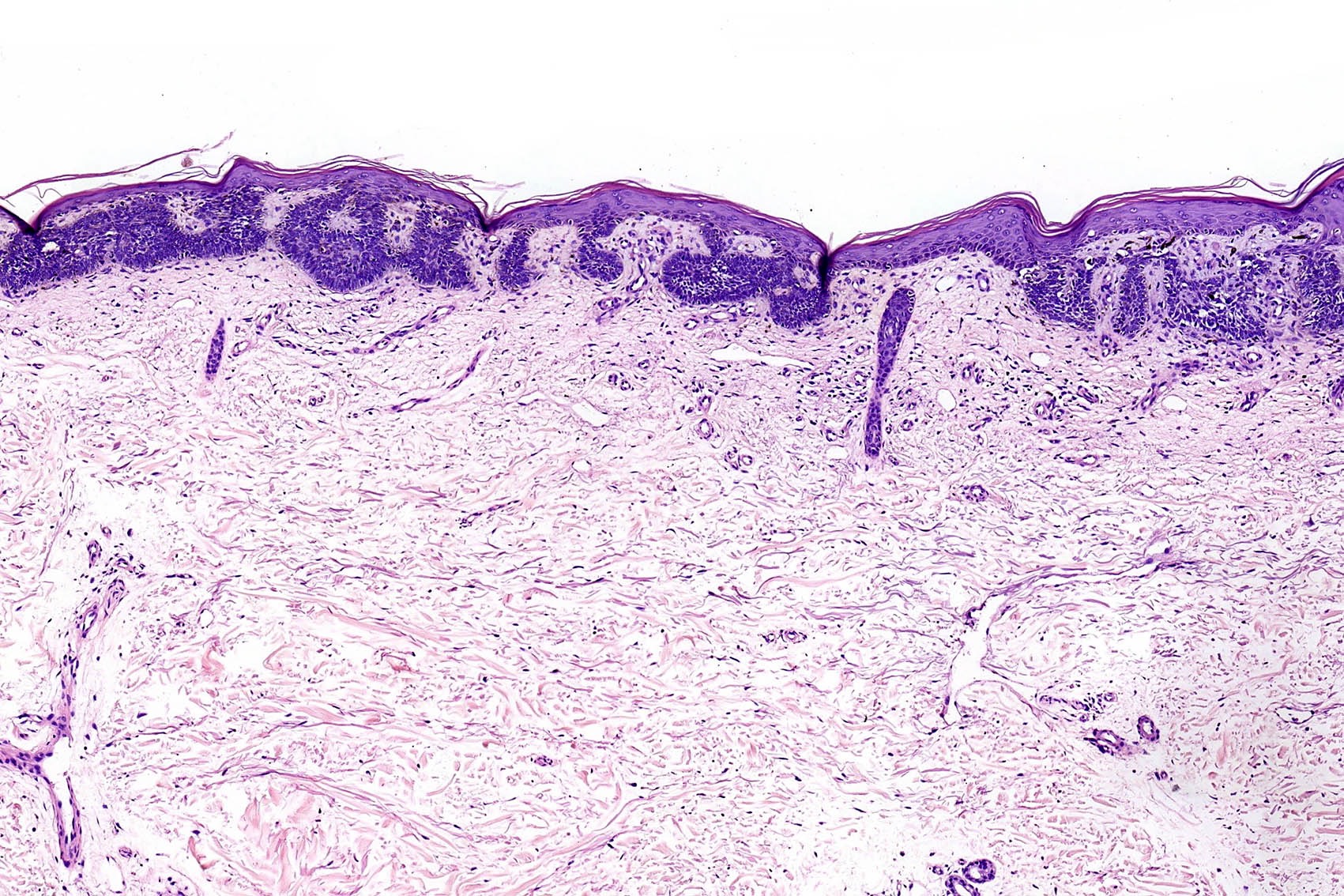
- Superficial BCC
- Isolated basaloid lobules projecting from the lower margin of the epidermis
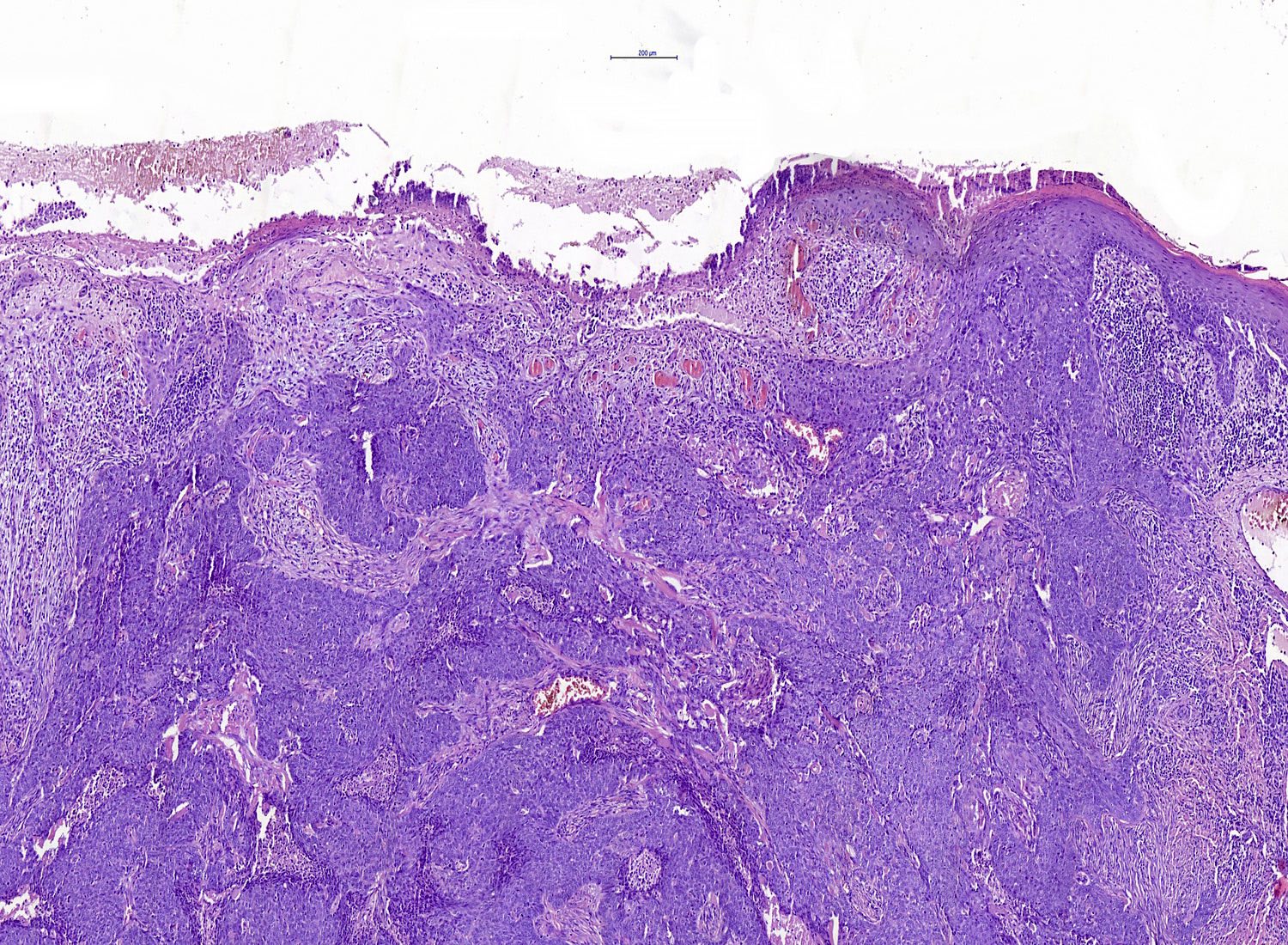
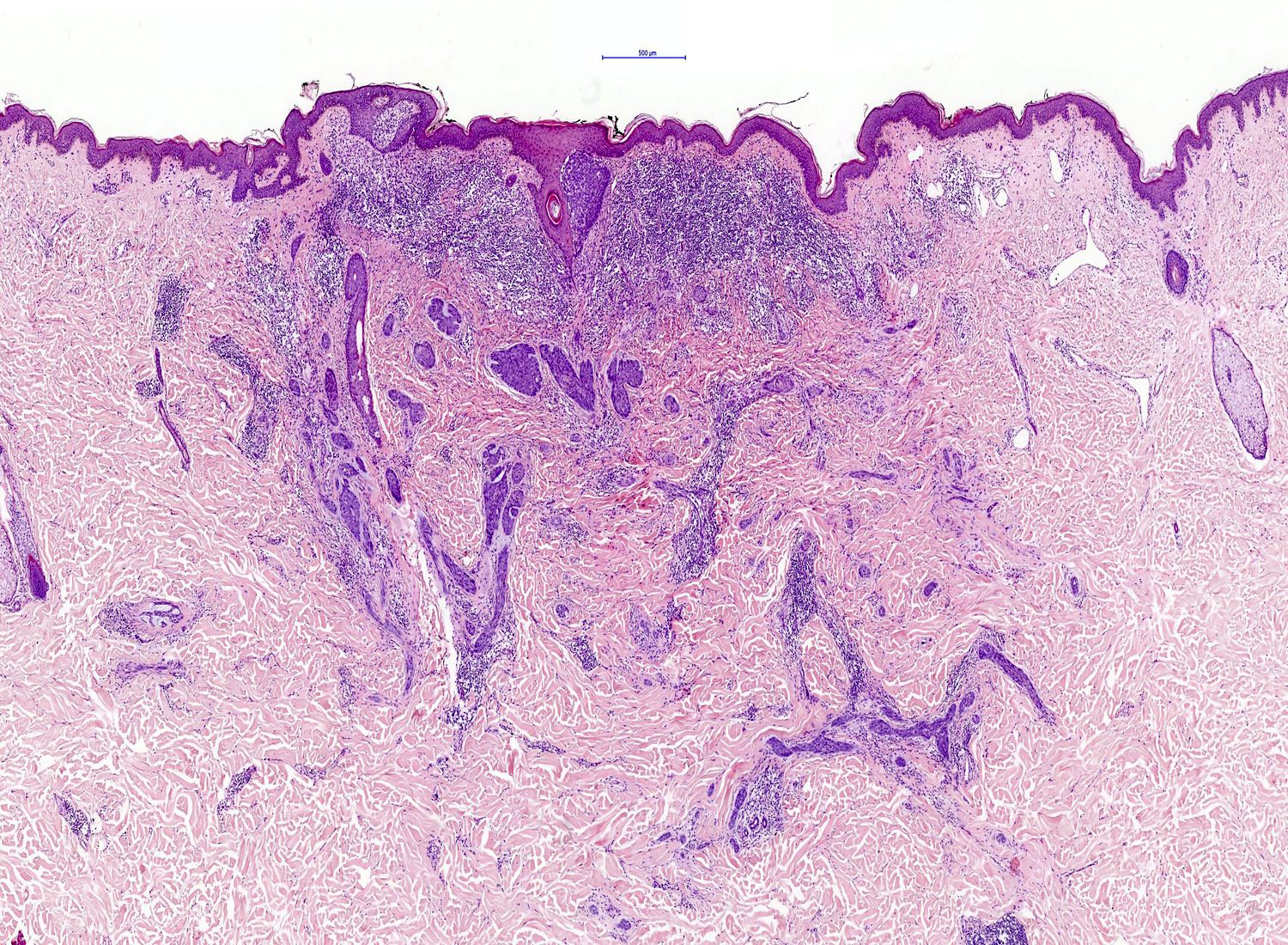
- Ulcerative BCC
- Ulceration
- Highly infiltrative growth pattern
- Less commonly nodulocystic variant with ulceration
- BCC, fibroepitheliomatous type (fibroepithelioma of Pinkus)
- Anastomosing strands and cords of basaloid cells connected to the epidermis
- Peripheral nuclear palisading with a formation of follicular germ-like structures
- Rarely, isthmic differentiation is present
- Fibrotic stroma that can differentiate towards follicular papillae in the areas of germ-like structure formation
Rare variants
- Pleomorphic (giant cell, BCC with monster cells) BCC
- Mitotic activity
- Apoptosis
- Сellular pleomorphism and giant cell formation
- Atypia has no prognostic significance
- Clear cell BCC
- Focal or total clear cell change with clear to finely granular eosinophilic cytoplasm due to lysosomal degeneration
- Peripheral palisading is usually preserved
- Signet ring cell BCC
- Tumor cells with laterally displaced nuclei
- May show positivity for S100 protein, glial fibrillary acidic protein and smooth muscle actin, suggesting myoepithelial differentiation
- Referred to as BCC with myoepithelial differentiation
- Granular BCC
- Tumor cells with abundant granular eosinophilic cytoplasm
- BCC with differentiation towards adnexal structures
- Tumor complexes can show differentiation towards sebaceous, follicular, eccrine or apocrine structures
- Infundibulocystic BCC
- Synonym: BCC with follicular differentiation
- Superficial dermal proliferation of basaloid cells arranged in anastomosing cords and strands
- Peripheral palisading is present
- Stroma is typically scanty
- Infundibular cysts are present
- Metaplastic BCC
- Stromal malignant metaplastic features (carcinosarcoma)
- Chondroid, osteoid and smooth muscle differentiation may be seen
- BCC with matricial differentiation (shadow cell BCC)
- Tumor cells show differentiation towards matricial cells of the hair follicle displaying shadow cells and trichohyaline granules
- Keloidal BCC
- Stroma shows thick, sclerotic collagen bundles
- BCC with thickened basement membrane
- Tumor complexes surround by thickened basement membrane
- Basomelanocytic tumor
- Combined and intermixed basal cell and melanomatous elements
- BCC with neuroid type nuclear palisading
- Central nuclear palisading reminiscent of that seen in schwannoma
Contributed by Antonina Kalmykova, M.D., Phillip H. McKee, M.D., Sate Hamza, M.D., Eduardo Calonje, M.D.,
Wayne Grayson, M.B.Ch.B., Ph.D., James Sampson, M.B.B.S., M.Sc. and Assia Bassarova, M.D., Ph.D.
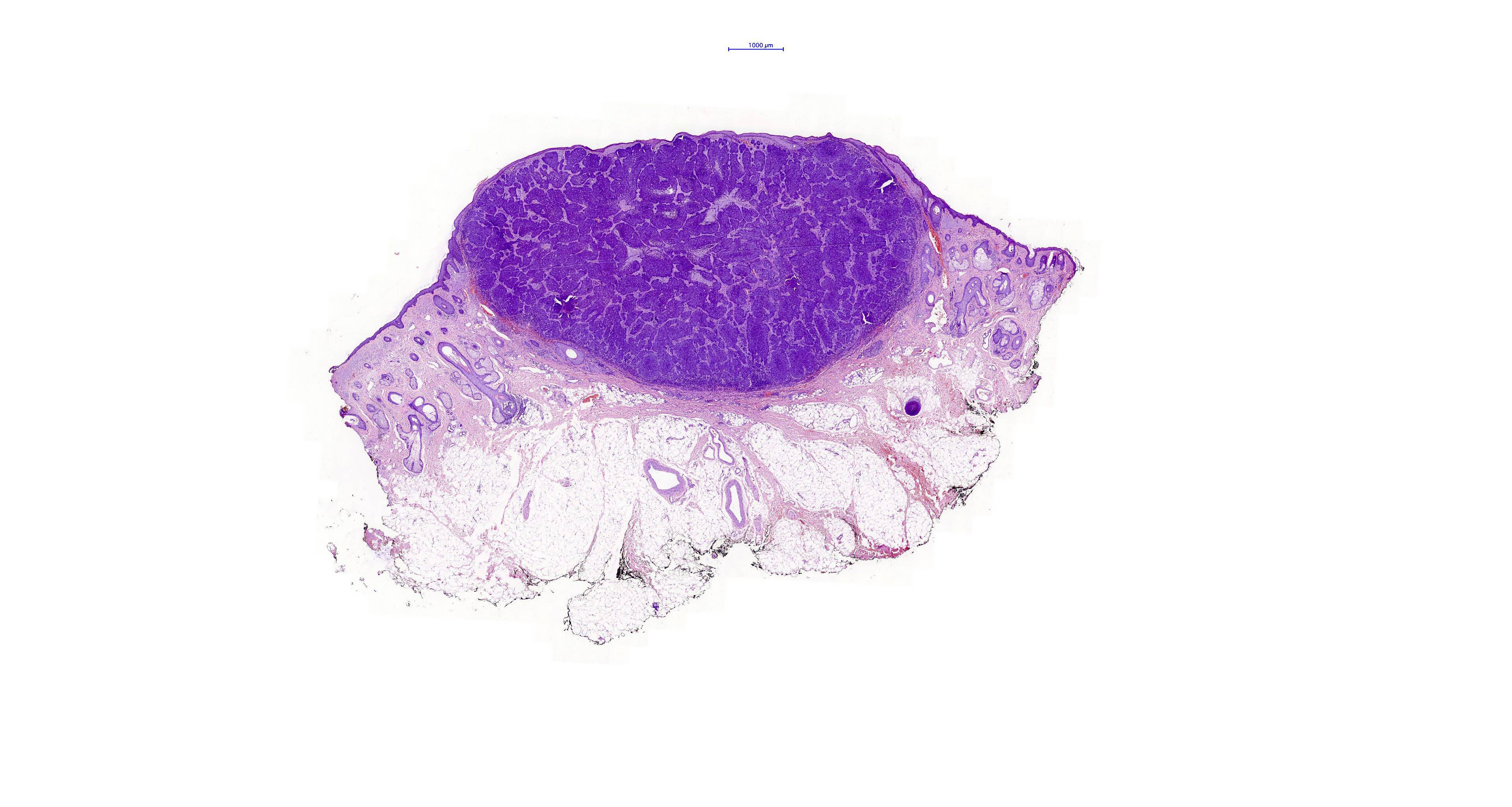
Nodular BCC
Nodular BCC

Nodulocystic BCC
Pigmented BCC
Ulcerative BCC
Superficial BCC
Adenoid BCC
Infiltrative BCC
Morpheaform BCC
Keloidal BCC
Micronodular BCC
Keratotic BCC
Granular cell BCC
BCC with matricial differentiation
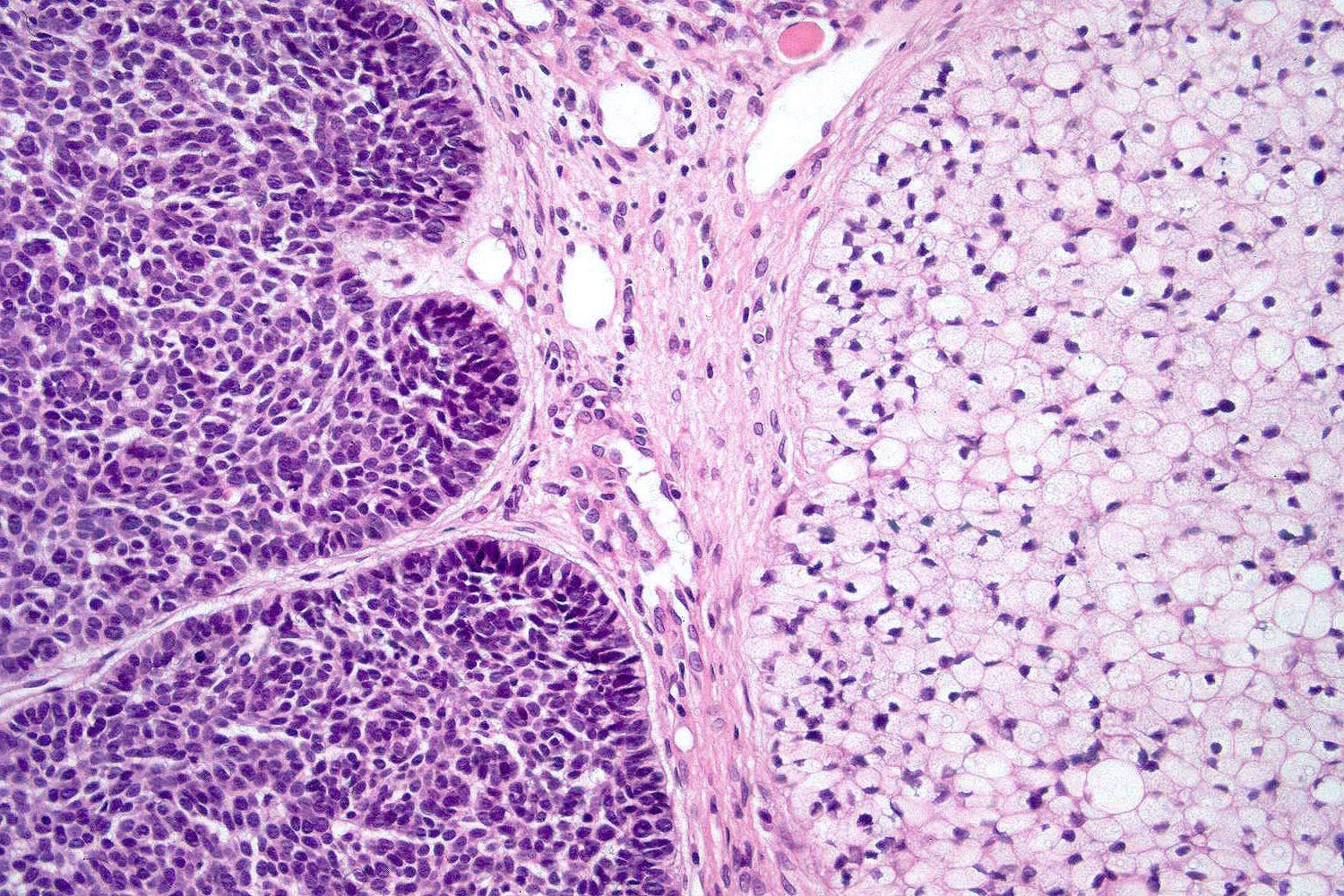
Clear cell BCC
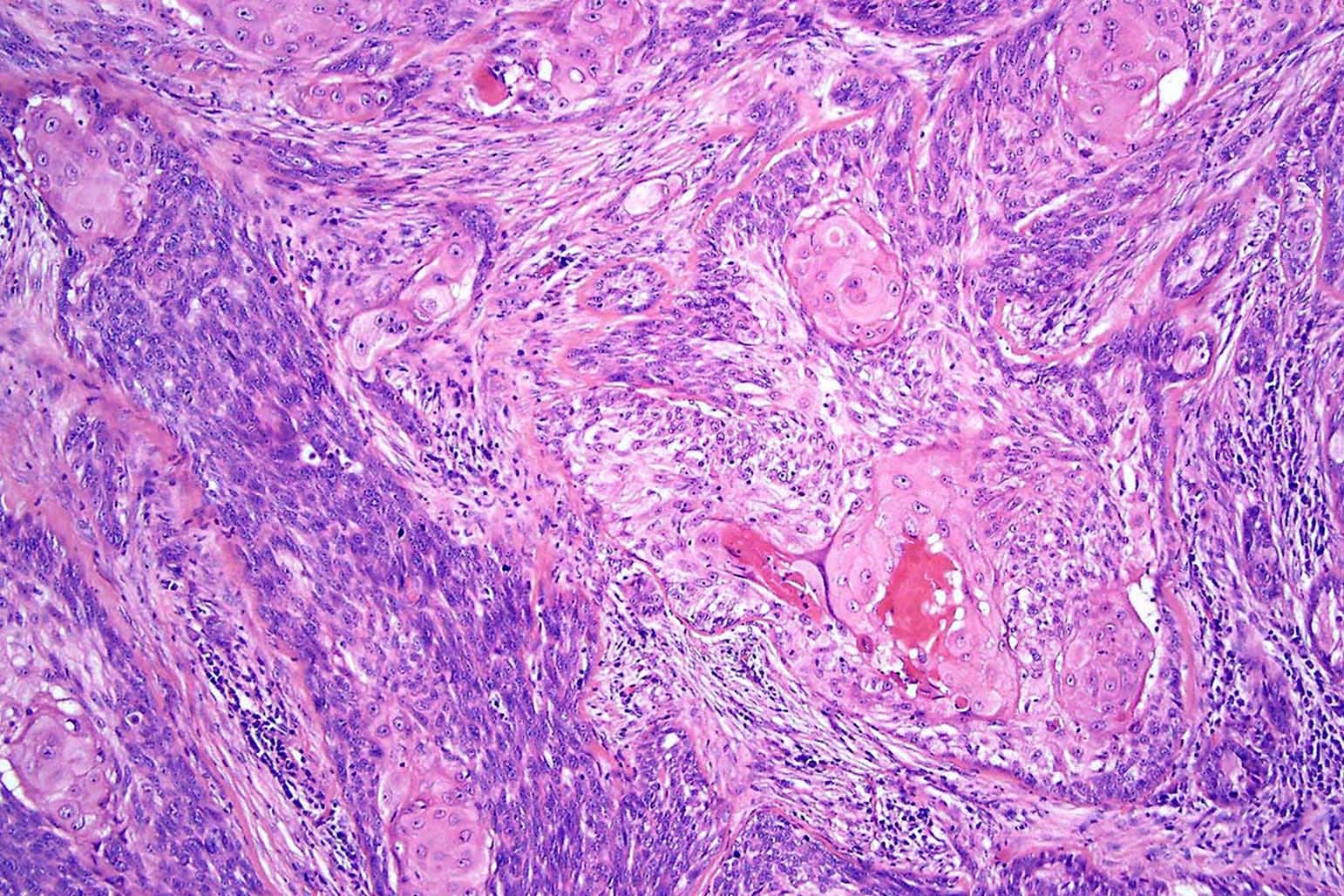
Basosquamous carcinoma
BCC with thickened basement membrane
Basomelanocytic tumor
Basomelanocytic tumor: AE1 / AE3
Basomelanocytic tumor: melanA
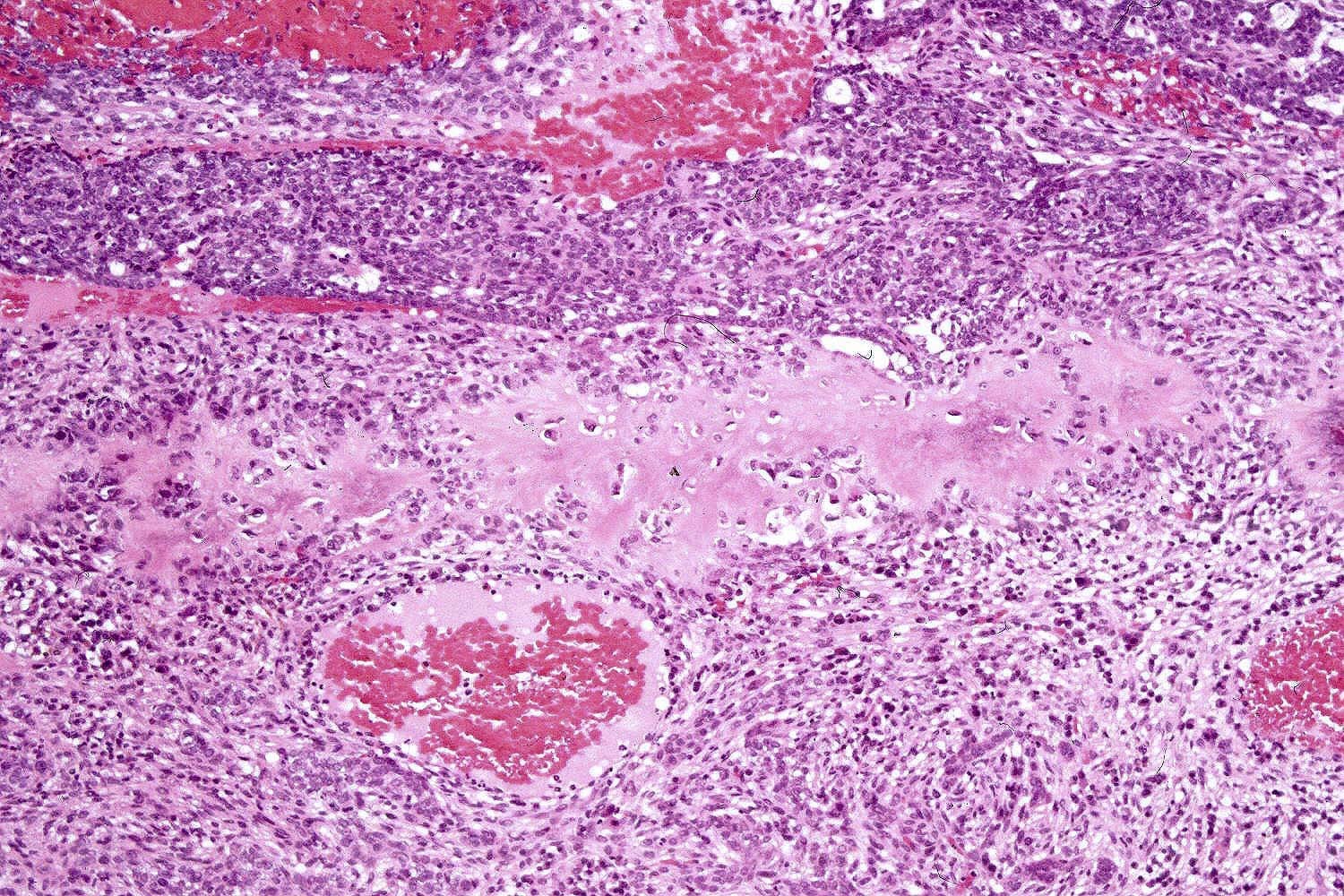
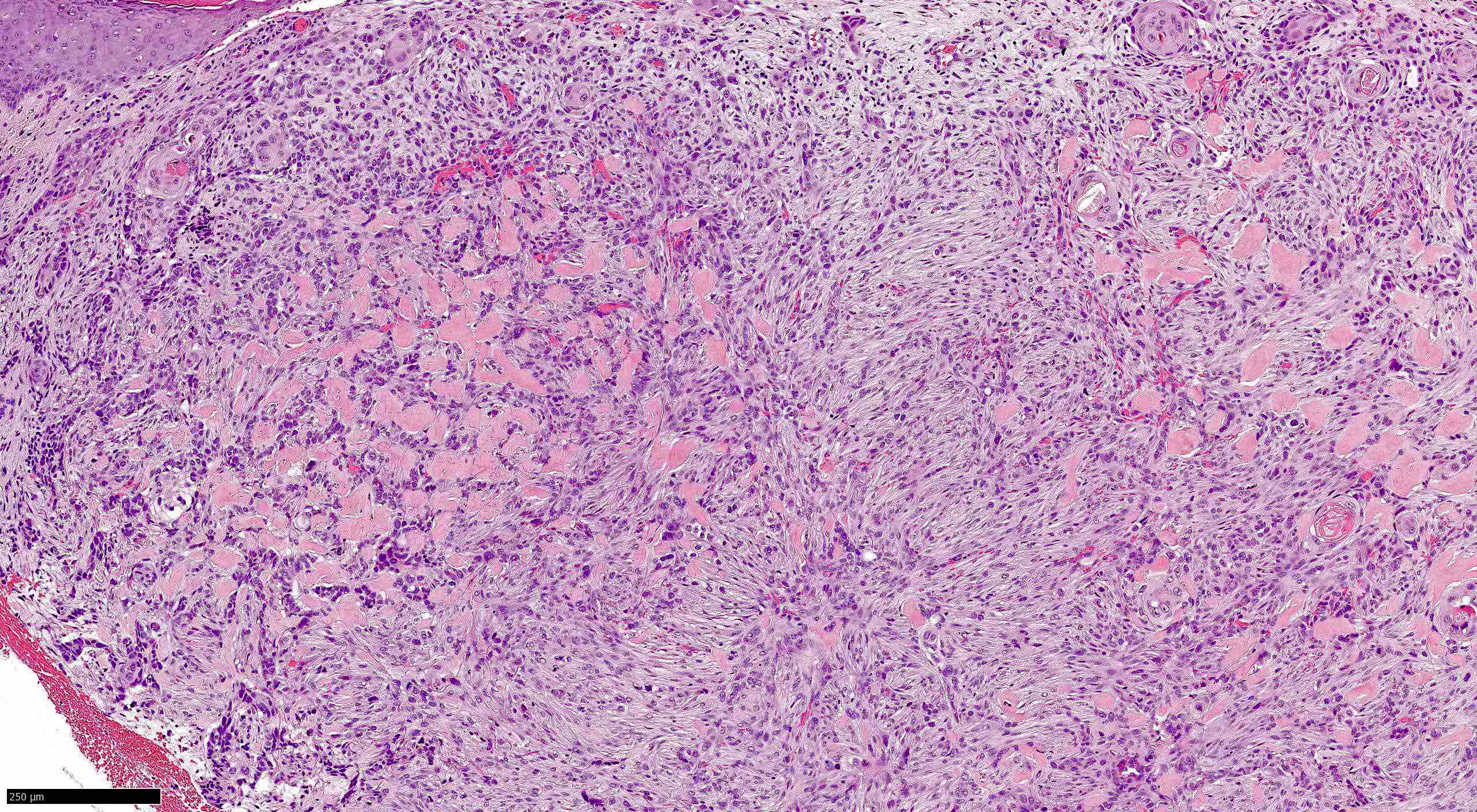
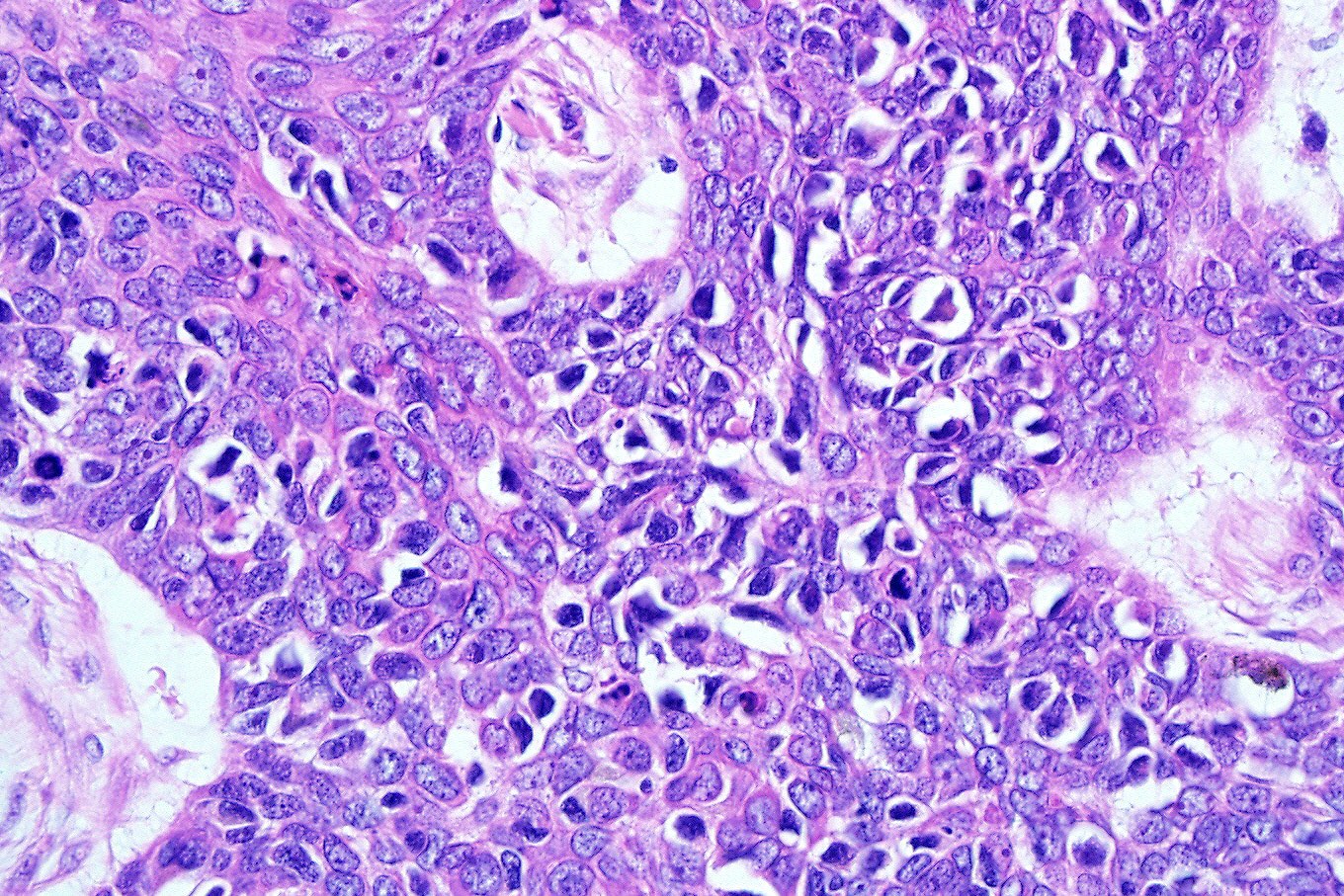
Metaplastic BCC
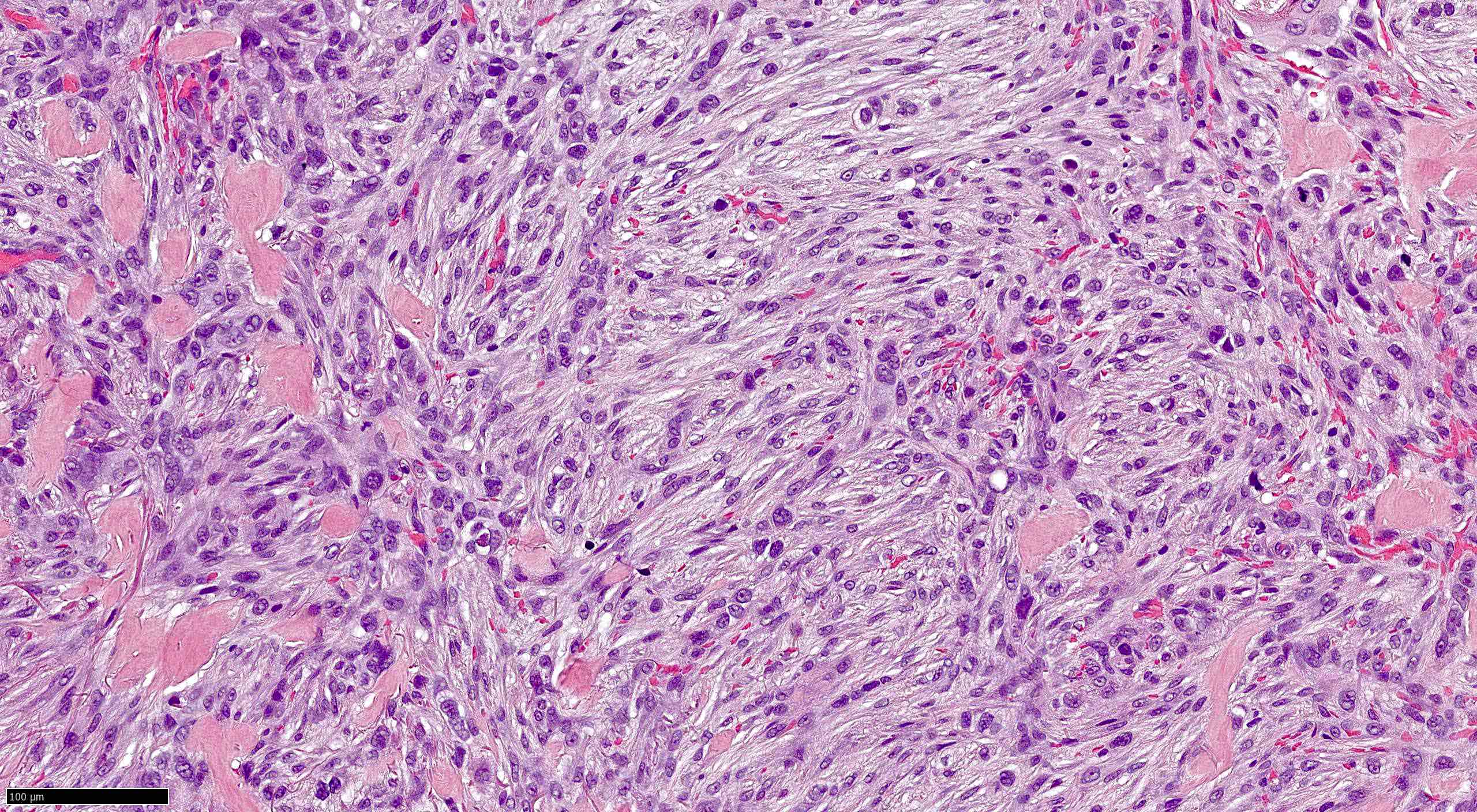
Metaplastic BCC
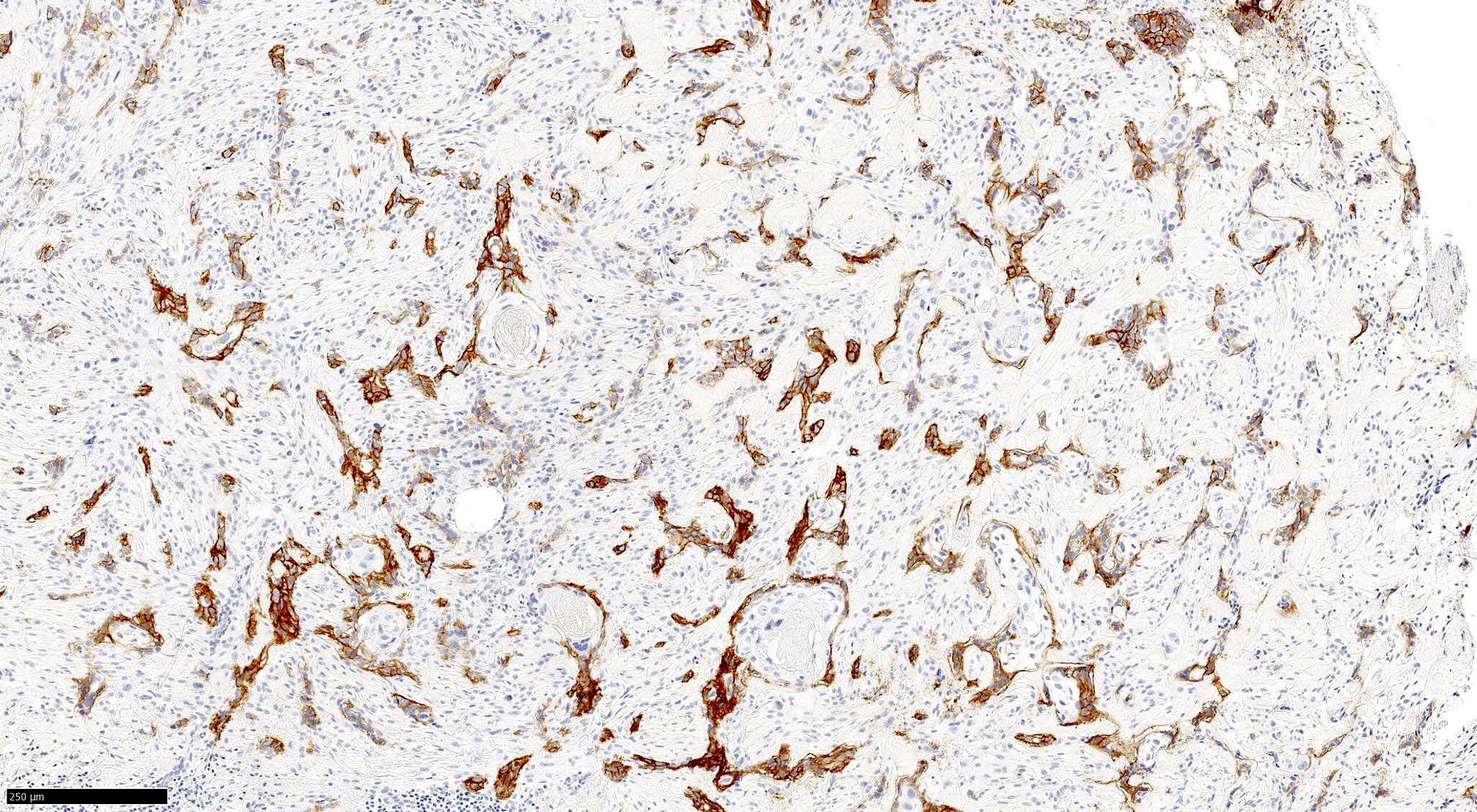
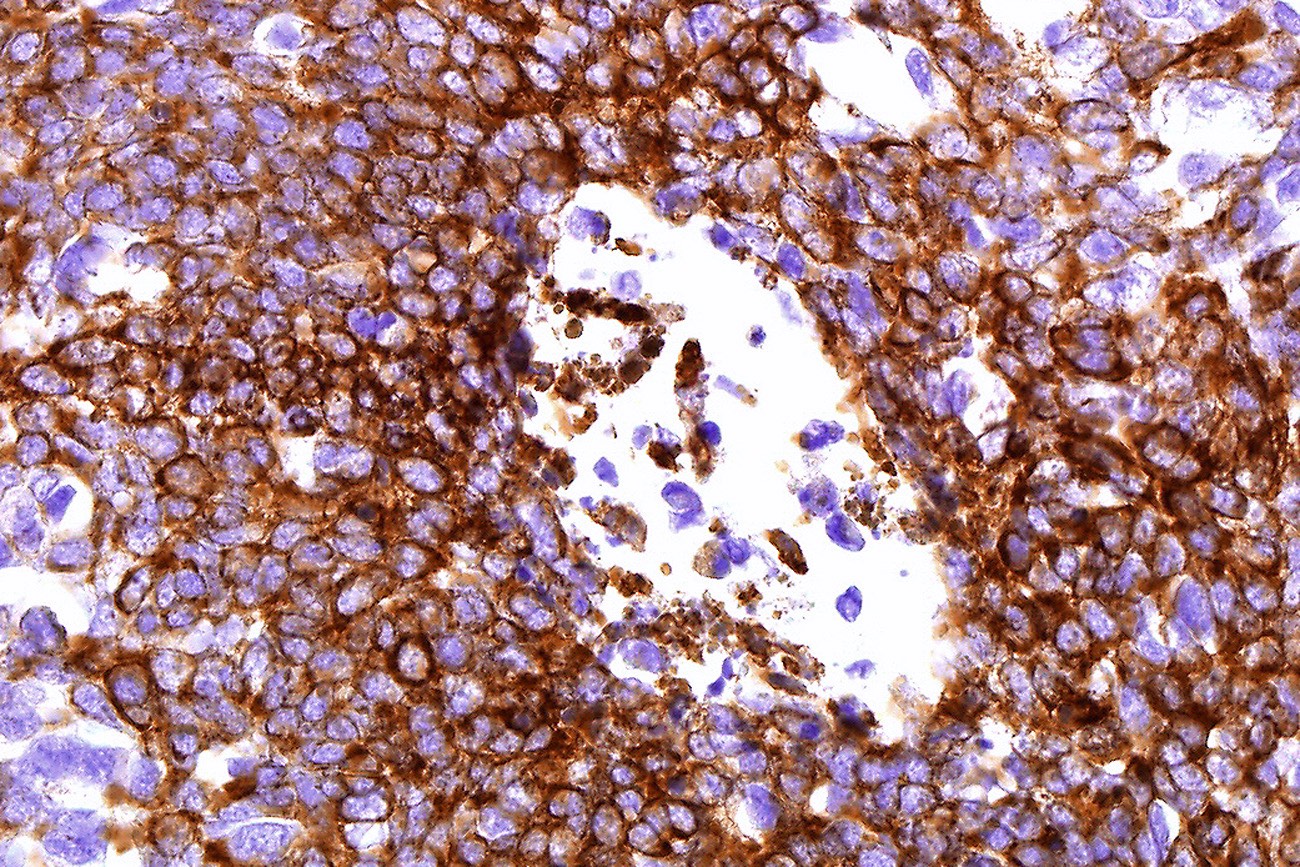
Metaplastic BCC: BerEP4
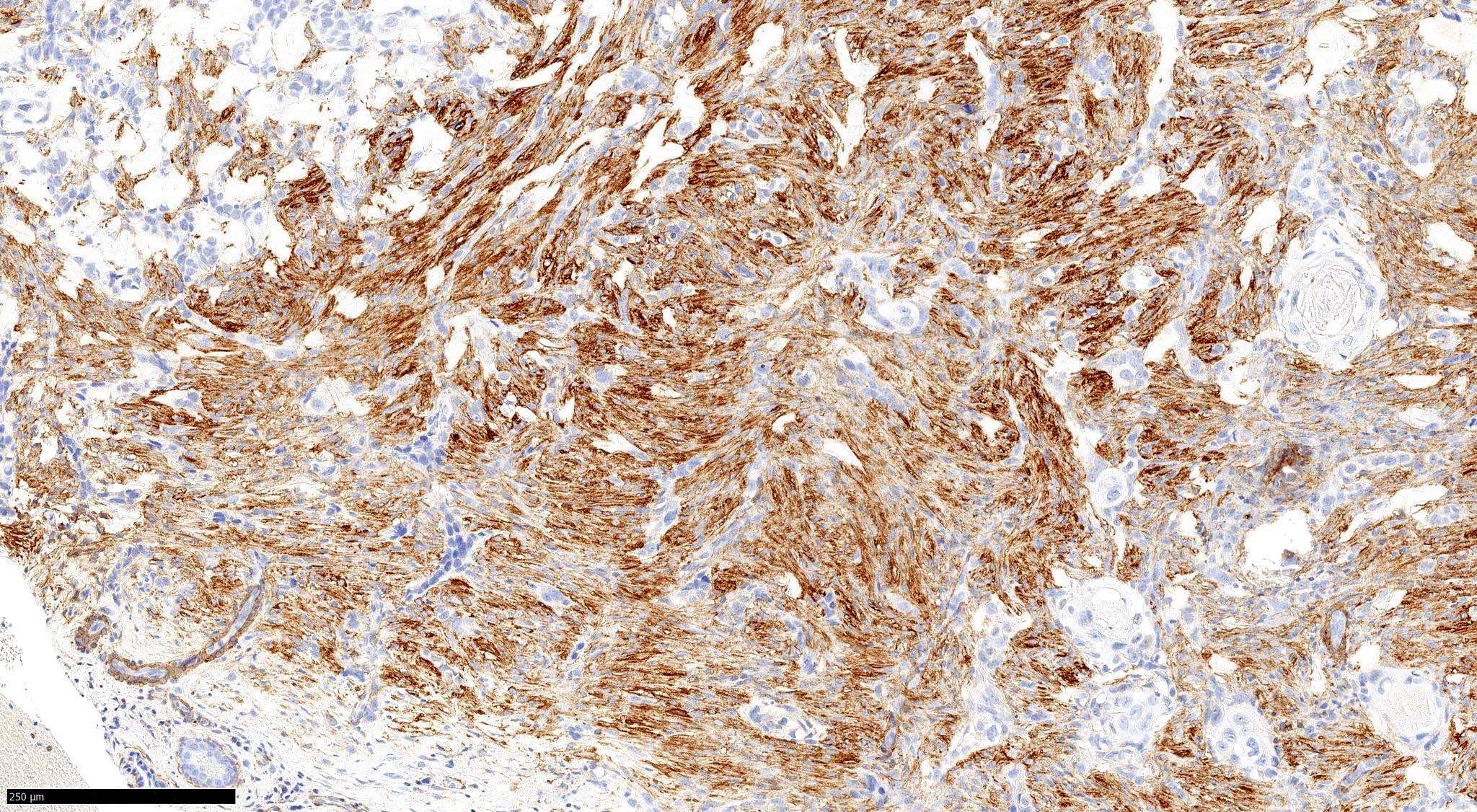
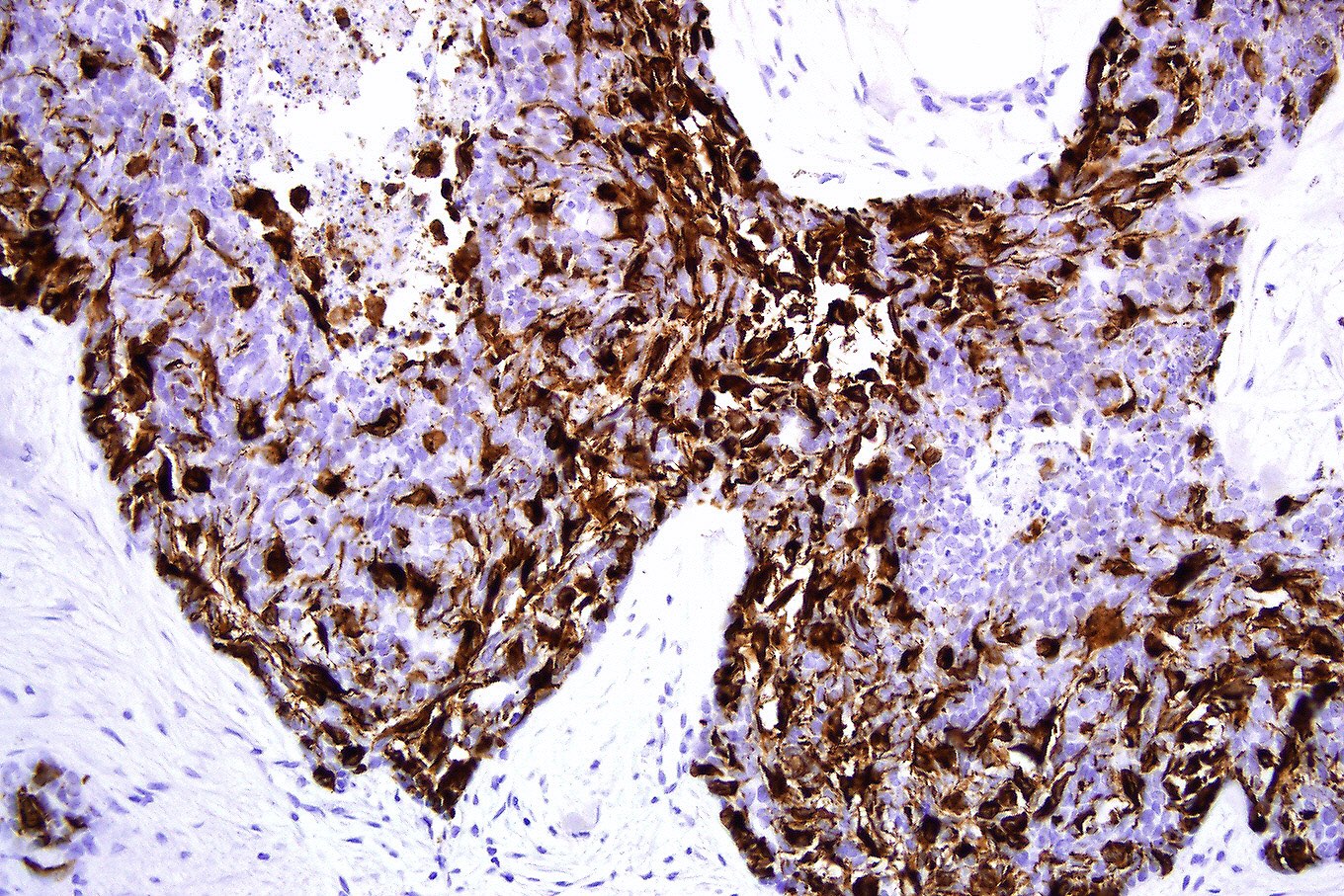
Metaplastic BCC: SMA


Fibroepithelial BCC (Pinkus tumor)
Rippled pattern BCC
Rippled pattern BCC: p63
Rippled pattern BCC: CK8/18
Rippled pattern BCC: BerEP4
- Sensitivity and specificity of exfoliative cytology estimate 97.5% (95% CI 94.5% to 98.9%) and 90.1% (95% CI 81.1% to 95.1%) respectively and can result in wrong or false positive result (Cochrane Database Syst Rev 2018;12:CD013187)
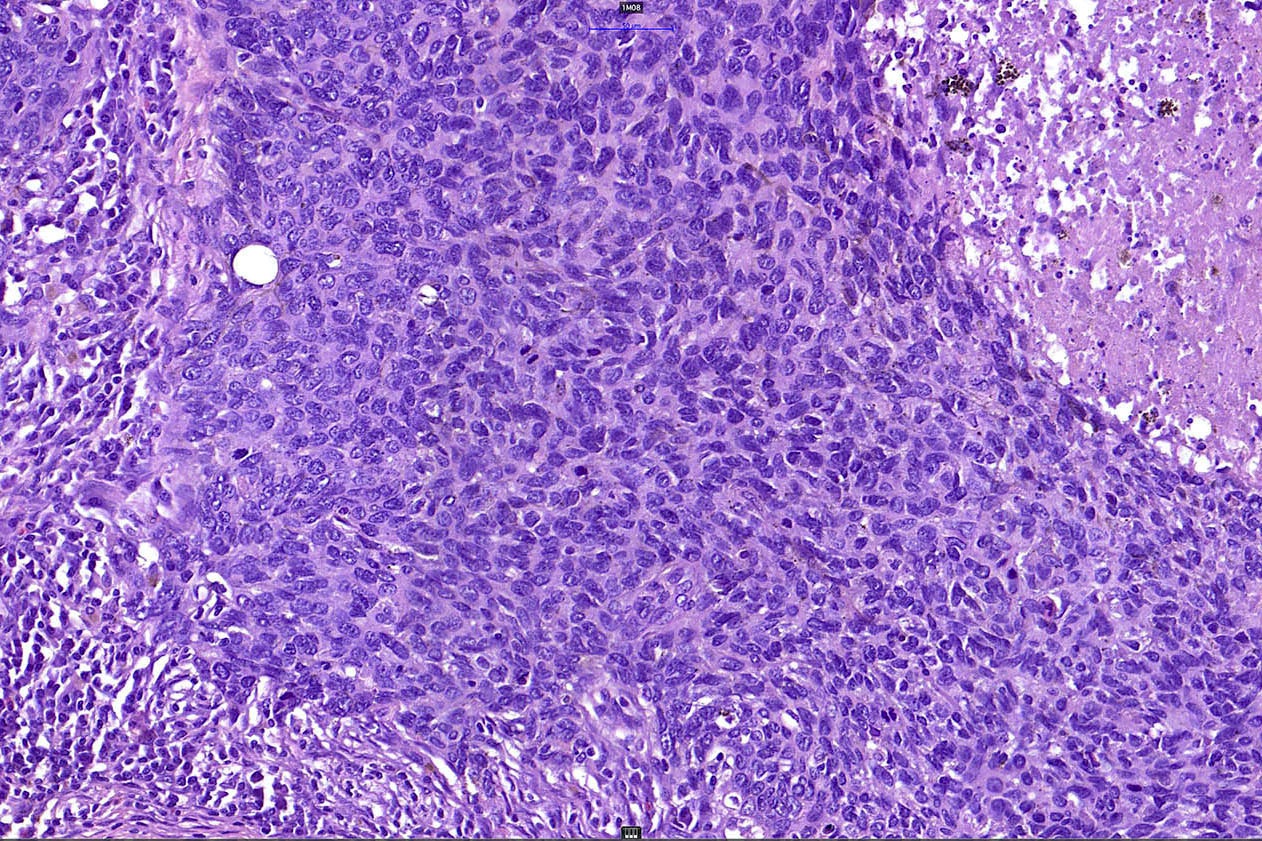
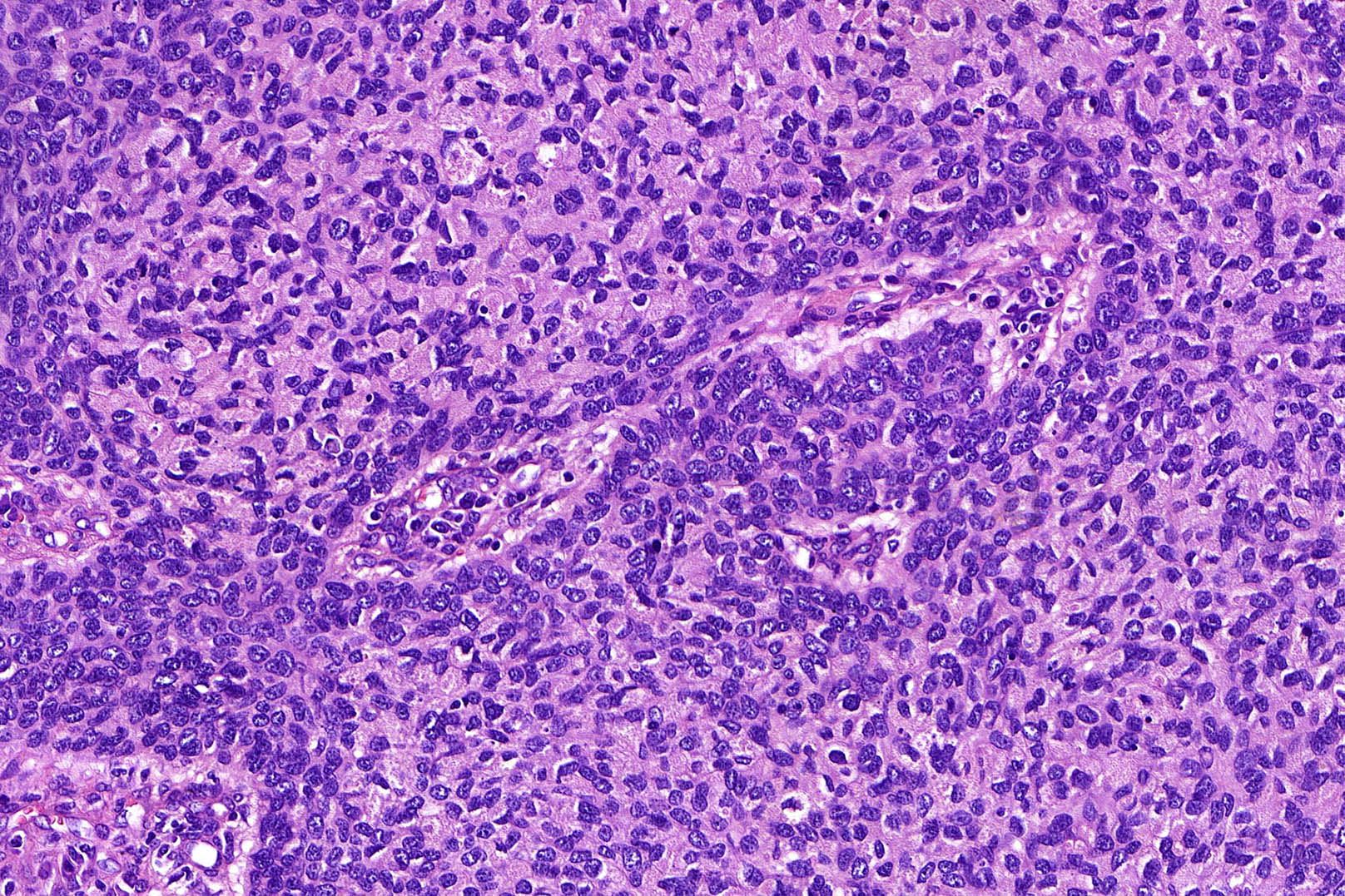
- Complexes of tightly packed basaloid cells with palisading in the periphery
- High nuclear/cytoplasmic ratio, minimal atypia and mitotic activity
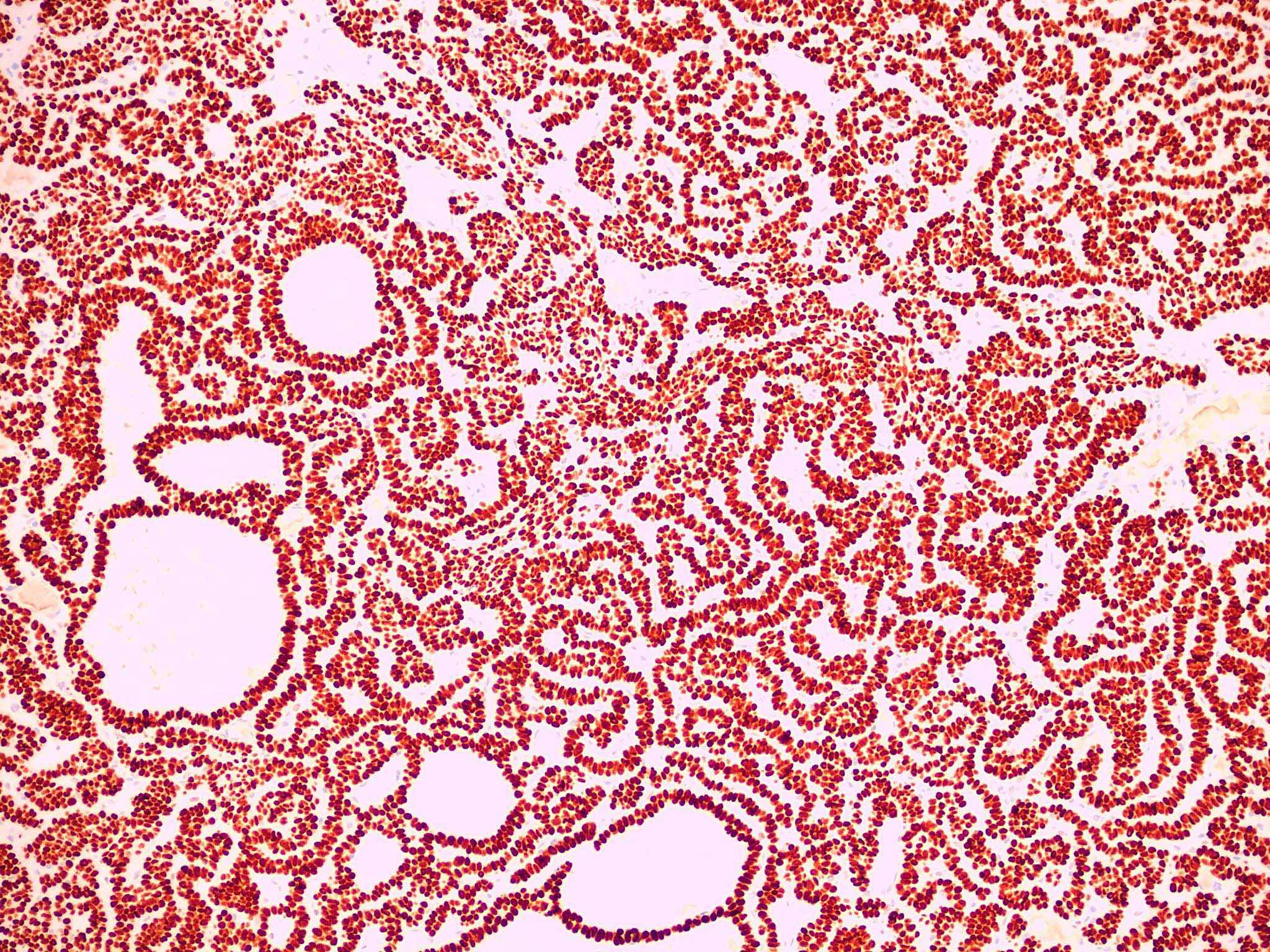
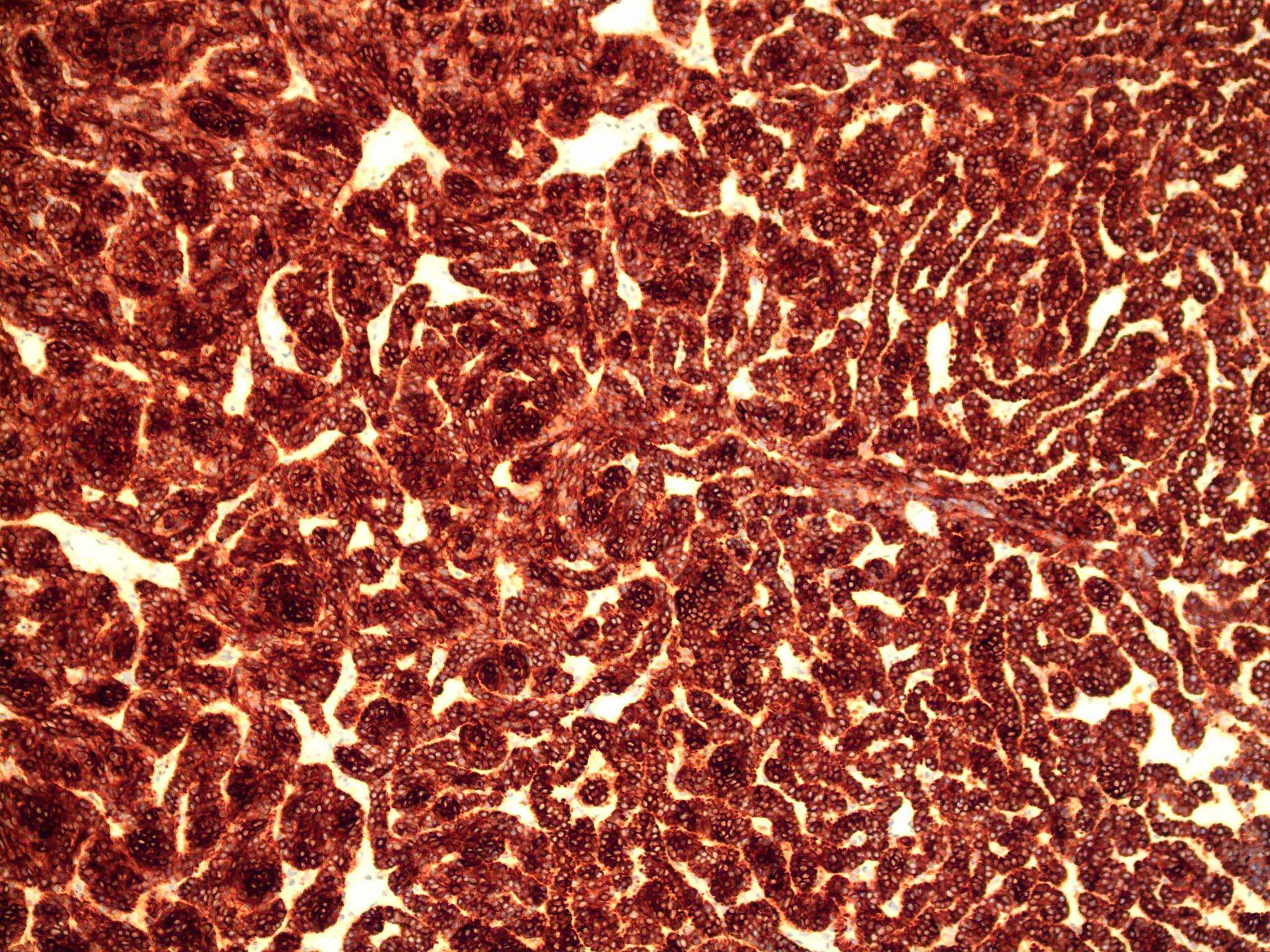
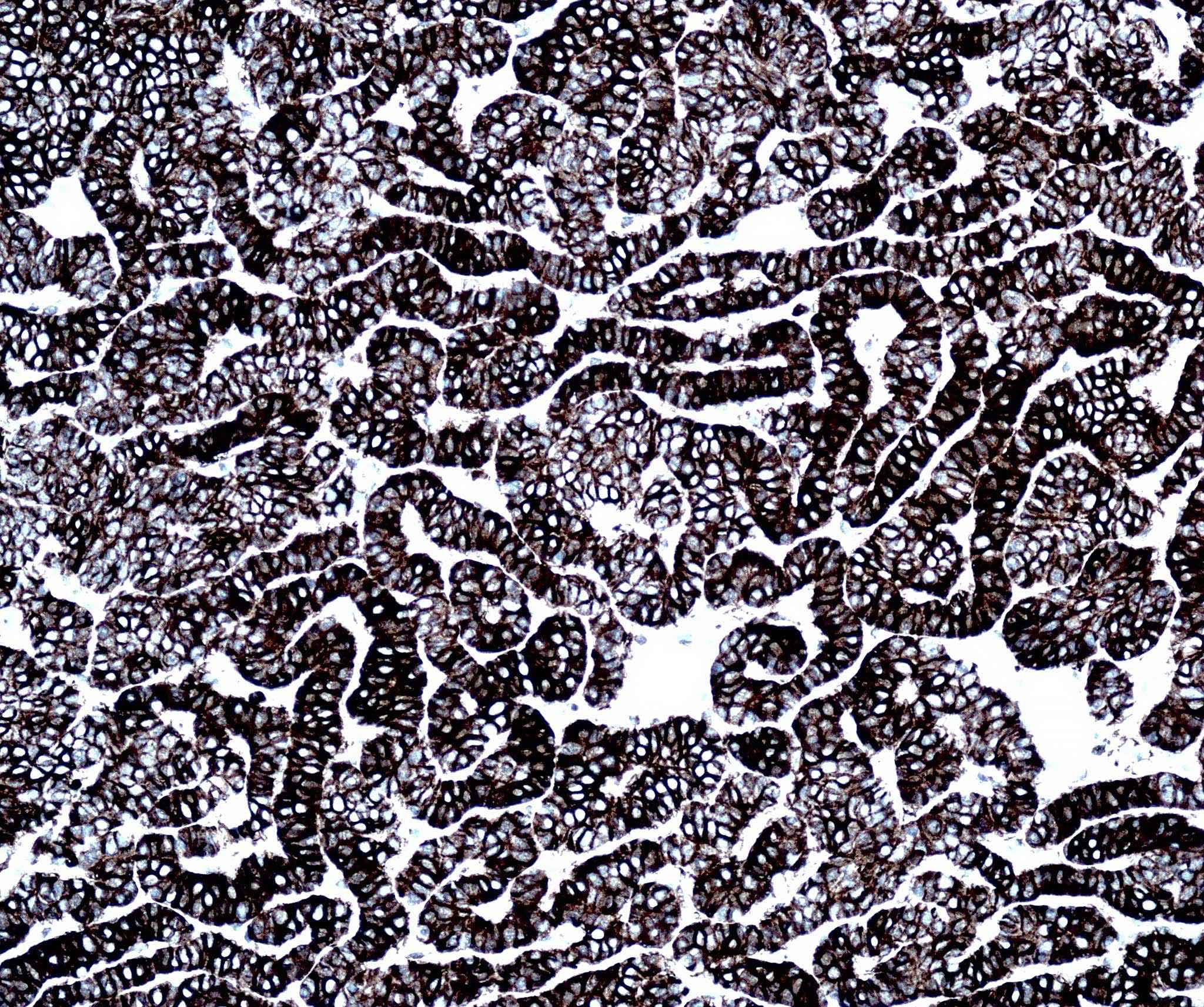
- CK AE1 / AE3 (100%), BerEP4 (80 - 100%), p63 (100%), CAM 5.2 (20 - 95%), androgen receptor (33 - 66%), p53 (74.5 - 83%), 34 beta E12 (high molecular weight CK), BCL2 (diffuse pattern), CD10 (positive in tumor cells, negative in stroma) (Dermatopathology (Basel) 2015;2:15, Arch Pathol Lab Med 2017;141:1490, Rom J Morphol Embryol 2018;59:1115, Am J Pathol 1992;141:25)
- CK20, adipophilin, SOX10, S100, MelanA / MART1, HMB45, CD34, CD44 (Dermatopathology (Basel) 2015;2:15)
- Usually negative: CK7 (0 - 70%), CEA (0 - 20%), EMA (0 - 6%) (Dermatopathology (Basel) 2015;2:15, Arch Pathol Lab Med 2017;141:1490, Rom J Morphol Embryol 2018;59:1115, Am J Pathol 1992;141:25)
- Chromosomal gains at 6p (47%), 6q (20%), 9p (20%), 7 (13%) and X (13%)
- Regional loss on 9q in 33% of tested tumors encompassing 9q22.3 to which the Patched gene has been mapped (J Invest Dermatol 2001;117:683)
BCC discussed by Dr. Jerad Gardner
Malignant keratinocytic neoplasms discussed by Dr. Clay J. Cockerell
- Face, excision:
- Nodular basal cell carcinoma (LVI0 Pn0 R0) (ICD-O code 8097/3) (see synoptic report)
- Synoptic report:
- Tumor site: face
- Procedure: excision
- Histological type: nodular basal cell carcinoma
- Depth of invasion: 2.5 mm
- Tumor size (greatest dimension): 7 mm
- Anatomic level (Clark level): IV
- Lymphovascular invasion (LVI): 0
- Perineural invasion (Pn): 0
- Peripheral margins: uninvolved
- Deep margin: uninvolved
- Reference: NCCN: Basal Cell Skin Cancer Evidence Blocks [Accessed 15 December 2020]
- Follicular induction (also known as follicular basal cell hyperplasia, epidermal basaloid cell hyperplasia and basaloid epidermal proliferation) versus superficial BCC:
- Usually seen above dermatofibroma, less common above nevi
- Follicular differentiation (germinative buds and papillary mesenchymal bodies) shows clear cell hyperplasia, epidermal hyperplasia between sites of follicular induction
- No atypical nuclei, increased mitotic figures or apoptotic bodies
- CK20+ colonizing Merkel cells
- Trichoepithelioma / trichoblastoma versus nodular BCC:
- Delicate perifollicular-like stroma with small spindled cells
- Papillary mesenchymal bodies
- No prominent cleft retraction, myxoinflammatory stroma, significant mitotic activity (is sometimes marked in trichoblastoma and should not be misconstrued as implying malignant trichoblastoma), cytologic atypia or tumor necrosis
- Desmoplastic trichoepithelioma versus morpheaform BCC:
- Does not extend into the deep dermis
- Architectural symmetry, horn cysts with calcification, granulomatous inflammation and follicular / sebaceous / infundibular differentiation
- No mitotic figures, ductal differentiation, cytologic atypia, tumor to stroma clefting or perineural infiltration
- CK20+ colonizing Merkel cells, androgen receptor-
- PHLDA1+ (highly specific for trichoepithelioma / trichoblastoma, although expression in micronodular BCC has been reported)
- Note: no single IHC marker can differentiate trichoepithelioma and BCC
- Basaloid follicular hamartoma versus infundibulocystic BCC:
- Tumor of follicular infundibulum versus superficial BCC:
- Syringoma versus morpheaform BCC:
- Squamous cell carcinoma (basaloid, clear cell, sarcomatoid):
- Shows an intraepidermal component, pagetoid spread
- No peripheral palisading, clefting or myxoinflammatory stroma
- Areas with conventional features like keratinization, keratin pearls
- BerEP4- (also absent in squamous areas of basosquamous carcinoma)
- EMA+ (may be expressed in squamous areas of BCC), CD44+
- Microcystic adnexal carcinoma versus morpheaform BCC:
- Superficial keratocysts (infundibular or isthmic), ductal differentiation with eosinophilic luminal secretions
- Frequently invades nerves (can't discriminate)
- No peripheral palisading, mitotic activity, tumor to stroma retraction or myxoinflammatory stroma
- CEA+, EMA+ in ductal structures
- CK15+, BerEP4 variable (mixed reports)
- p63 highlights ductal myoepithelial cells
- Sebaceous carcinoma versus BCC (nodular, clear cell):
- Intraepidermal pagetoid spread
- No peripheral clefting
- May have evidence of sebaceous, lobular architecture
- Often relatively greater cytologic atypia and less basaloid morphology
- Diffuse androgen receptor+ (versus focally positive in BCC)
- Low molecular weight CK+, EMA+
- BerEP4-, adipophilin+, perilipin+
- Merkel cell carcinoma:
- Rarely may show intraepidermal with pagetoid spread
- No / focal peripheral palisading
- Homogenous salt and pepper chromatin
- Nuclear molding
- Abundant mitotic activity and necrosis
- MCPyV 70 - 80% (highly specific marker)
- CK20+ (paranuclear, dot-like pattern)
- Neuroendocrine markers expressed but rarely also positive in BCC
- Adenoid cystic carcinoma versus adenoid BCC:
- Well defined cribriform patterns
- No peripheral palisading, continuity with the epidermis or adjacent hair follicle or retraction artifacts between the tumor islands and stroma
- Typically shows hyaline material lining the lumina of the ducts and sometimes also present in the stroma
- CD117+ (20% of BCC CD117+), CD43+ (40%), CK7+, CEA+, EMA+ (in ductal structures)
- p63+, SMA+, calponin+ (myoepithelial cell population at periphery of tumor islands)
- Clear cell melanoma (balloon cell melanoma) versus clear cell BCC:
- Clear cell eccrine porocarcinoma versus clear cell BCC:
- Clear cell hidradenocarcinoma versus clear cell BCC:
- Trichilemmal carcinoma versus clear cell BCC:
- Pilomatrix carcinoma versus BCC with matricial differentiation:
- No conventional areas of BCC
- Pigmented reticulated seborrheic keratosis versus BCC with follicular differentiation:
- No peripheral palisading, myxoinflammatory stroma, peripheral clefting, atypical nuclei, increased mitotic figures or apoptotic bodies
- CK20+ colonizing Merkel cells may be present
- Cylindroma versus BCC with thick basement membrane:

This image comes from a tumor on the face of an elderly patient. What is the most likely diagnosis?
- Sclerosing sweat ductal carcinoma
- Microcystic adnexal carcinoma
- Basal cell carcinoma with ductal differentiation
- Secretory carcinoma
- Metastatic adenocarcinoma
This image comes from the head of an elderly patient. What is the most likely diagnosis?
- Sebaceoma
- Sebaceous carcinoma
- Sebaceous adenoma
- Basal cell carcinoma with sebaceous differentiation
- Porocarcinoma
