Breast
Other benign tumors
Intraductal papilloma
Deputy Editor-in-Chief: Gary Tozbikian, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 23 August 2021
Last staff update: 11 June 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Papilloma of the breast [title]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Bidot S, Li X. Intraductal papilloma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastpapilloma.html. Accessed October 3rd, 2025.
Definition / general
- Benign intraductal proliferation of epithelial cells with fibrovascular cores and underlying myoepithelial cells
Essential features
- Common benign breast lesion
- Distinction with malignant papillary lesions may be difficult on biopsy and immunohistochemistry may be necessary
- No consensus regarding management of papilloma without atypia
- Surgical excision of intraductal papilloma with atypical epithelial proliferation is recommended
Terminology
- Duct papilloma of the breast
- Intracystic papilloma of the breast (old terminology)
ICD coding
- ICD-10: D24 - benign neoplasm of the breast
Epidemiology
- 5% of benign breast lesions (Am J Surg Pathol 2006;30:665)
- Involves women of all ages (Arch Pathol Lab Med 2016;140:628)
- Uncommon in men
Sites
- Central intraductal papilloma: arises from large lactiferous ducts, usually solitary (Arch Pathol Lab Med 2016;140:628)
- Peripheral intraductal papilloma: involves terminal duct lobular unit, usually multiple (papillomatosis) (Arch Pathol Lab Med 2016;140:628)
Pathophysiology
- Poorly understood
- Intraductal papilloma might originate from bipotent progenitor cells that differentiate as luminal and myoepithelial cells (Am J Pathol 2018;188:1106)
Clinical features
- Solitary central intraductal papilloma may present as a retroareolar mass with serous or serosanguineous nipple discharge
- Peripheral intraductal papilloma is often discovered incidentally
Diagnosis
- Screening mammography
- Core needle biopsy, vacuum assisted biopsy, excisional biopsy (Surg Pathol Clin 2018;11:1)
Radiology description
- Nonspecific findings
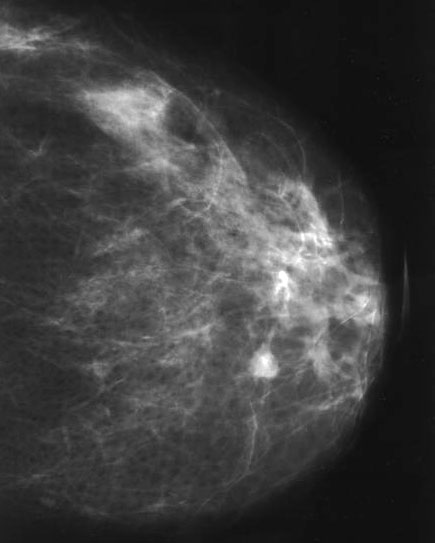
- Mammography (Diagn Interv Radiol 2013;19:471, AJR Am J Roentgenol 2012;198:264)
- Can be large (usually central papilloma), rounded or ovoid well circumscribed mass
- Calcifications may be seen
- Small lesions (usually peripheral papilloma) may not be visible
- Ultrasonography (Diagn Interv Radiol 2013;19:471, AJR Am J Roentgenol 2012;198:264)
- Classic pattern is solid mural nodule within a dilated duct
- Vascular pedicle may be seen on color Doppler
- MRI (Diagn Interv Radiol 2013;19:471, AJR Am J Roentgenol 2012;198:264)
- Well circumscribed round or ovoid intraductal mass with variable enhancement
- May be associated with ductal dilation
Radiology images
Contributed by Mark R. Wick, M.D.
Mammogram
Images hosted on other servers:

Round or ovoid mass on mammogram and ultrasound

Well circumscribed
mass with
calcifications

Ductal dilatation on mammogram
Prognostic factors
- Long term risk of developing breast carcinoma (Mod Pathol 2021;34:78)
- Papilloma without atypia: ~X2 if single; ~X3 if multiple
- Papilloma with atypia: ~X5 if single; ~X7 if multiple
- Risk of upgrade to malignancy (DCIS or invasive breast carcinoma)
- Upgrade rate of papilloma without atypia and with pathology / radiology concordance is low (Mod Pathol 2021;34:78, Am J Surg 2020;220:677, Cancer 2016;122:2819, Clin Imaging 2020;60:67, Breast Cancer Res Treat 2020;183:577, Ann Surg Oncol 2021;28:2573)
- Upgrade rate of intraductal papilloma with atypia is high (Hum Pathol 2021;110:43, Breast Cancer Res Treat 2020;183:577, Ann Surg Oncol 2021;28:2573)
Case reports
- 52 year old man with intraductal papilloma that progressed to ductal carcinoma in situ (Radiol Case Rep 2018;13:602)
- 53 year old woman with a large intraductal papilloma (Int J Surg Case Rep 2019;55:1)
- 55 year old man with unilateral bloody discharge and intraductal papilloma (J Surg Case Rep 2019;2019:rjz023)
Treatment
- No consensus for intraductal papilloma without atypia
- Complete surgical excision often performed (Am J Surg 2020;220:677)
- Different management among institutions (Clin Imaging 2020;60:67)
- Complete surgical excision should be performed for intraductal papilloma with atypia
Clinical images
Images hosted on other servers:

Male with nipple discharge
Gross description
- Central intraductal papilloma: well circumscribed polypoid nodule in a cystically dilated duct (Arch Pathol Lab Med 2016;140:628)
- Peripheral intraductal papilloma: not grossly visible (Arch Pathol Lab Med 2016;140:628)
Gross images
Contributed by Mark R. Wick, M.D.
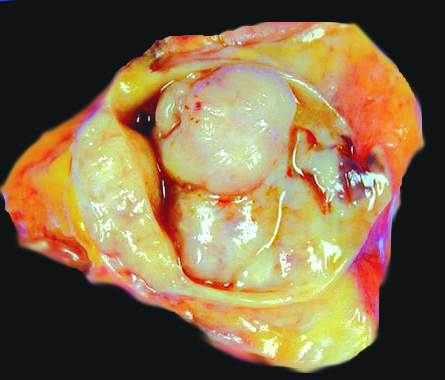
Intracystic mass
Images hosted on other servers:

Intraductal polypoid mass
Frozen section description
- Frozen section not performed on lesions suspected to be intraductal papilloma
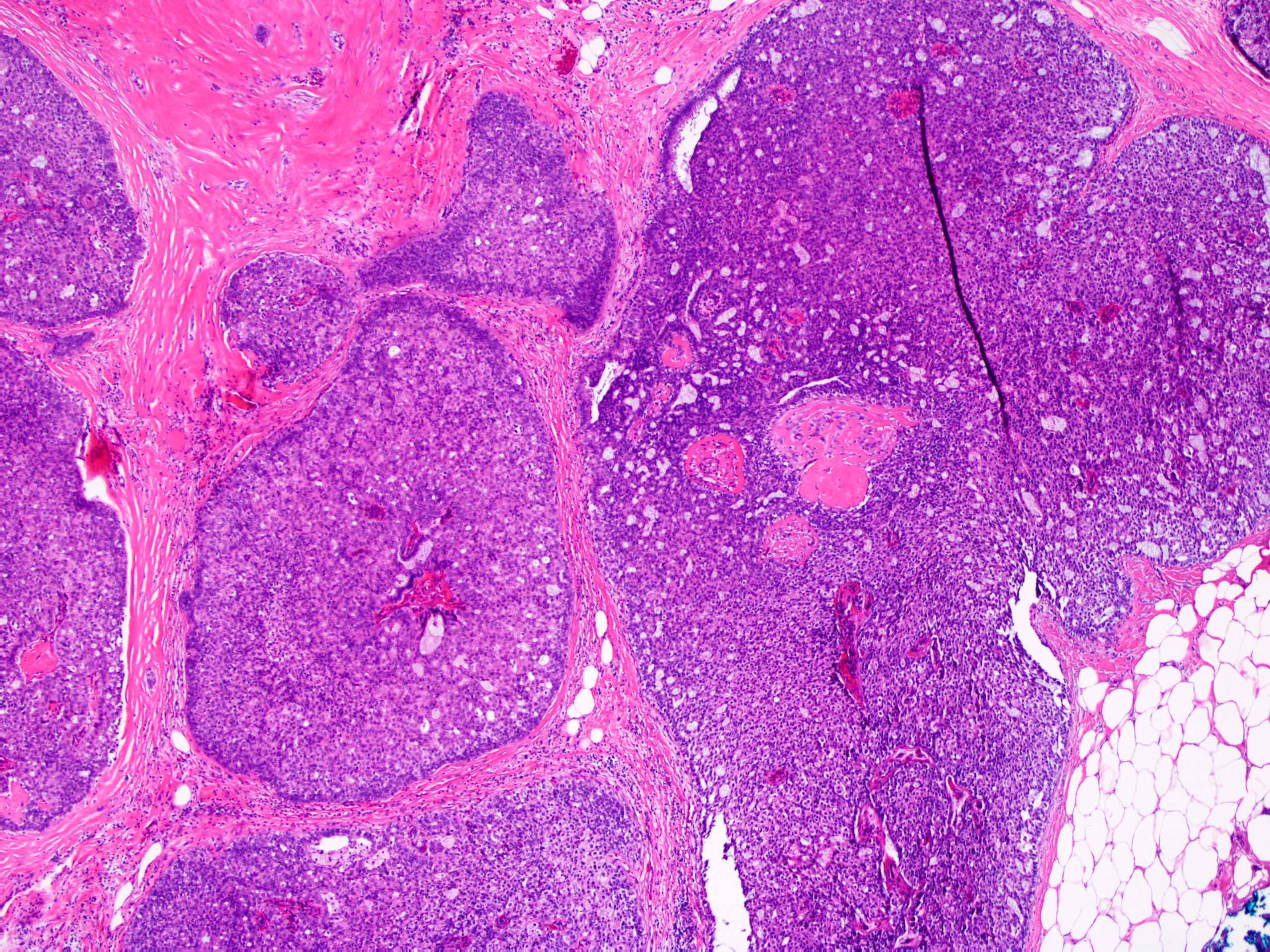
Microscopic (histologic) description
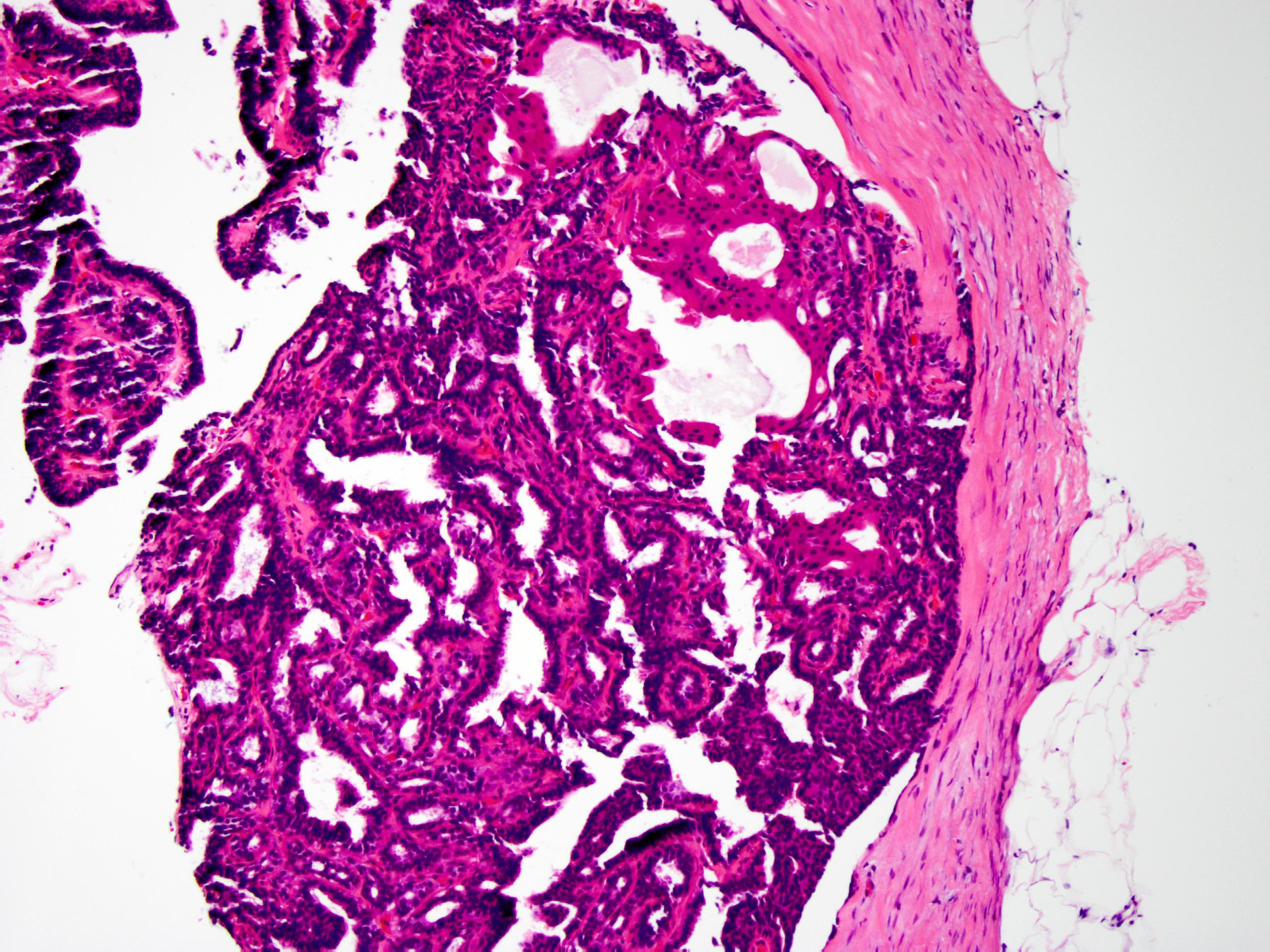
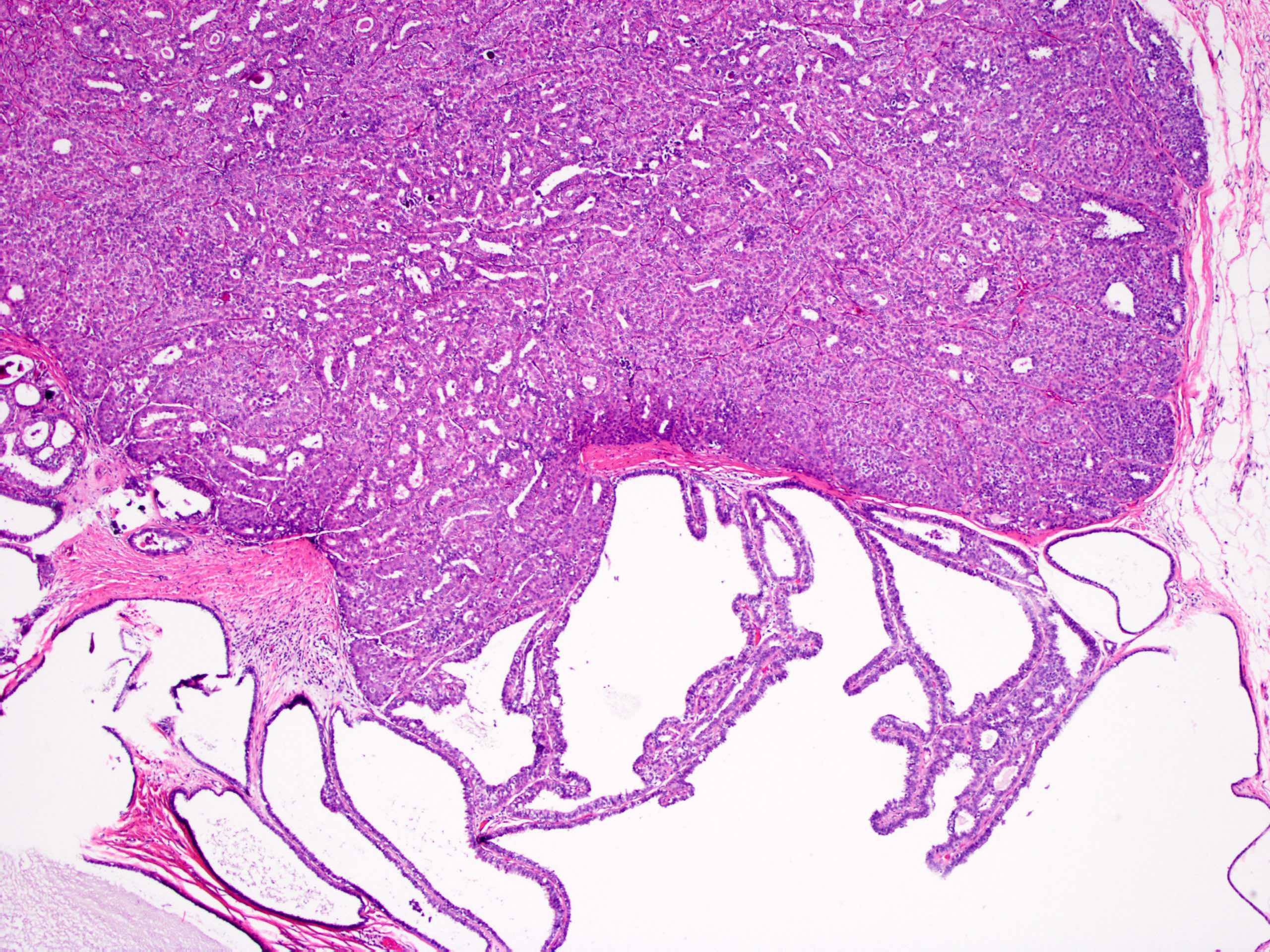
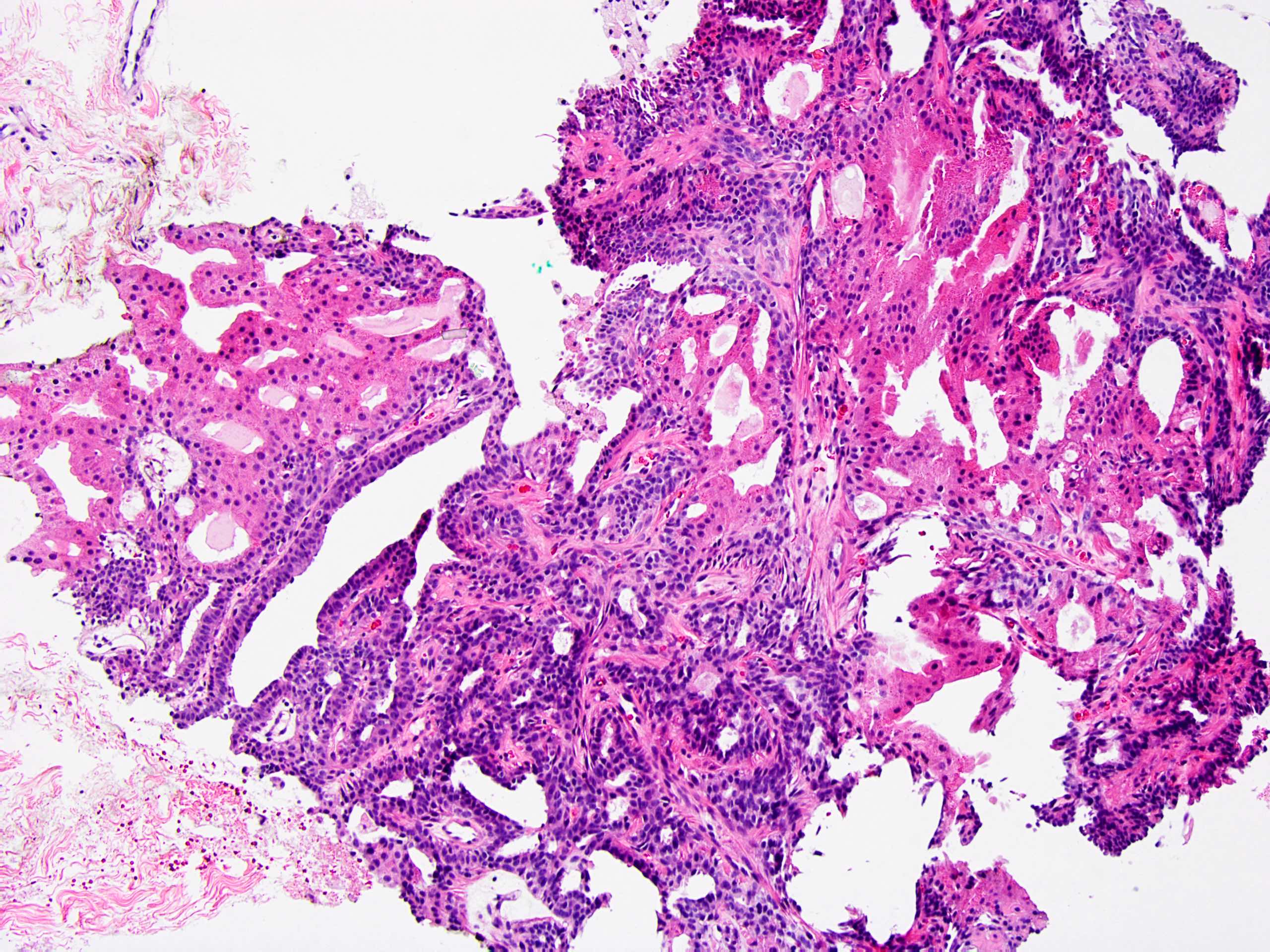
- Circumscribed intraductal proliferation comprised of arborizing fibrovascular cores lined by outer layer of luminal cells and an inner layer of myoepithelial cells (Histopathology 2016;68:22)
- Myoepithelial cells might be inconspicuous in sclerotic areas
- Myoepithelial cells also present at the periphery of the involved duct
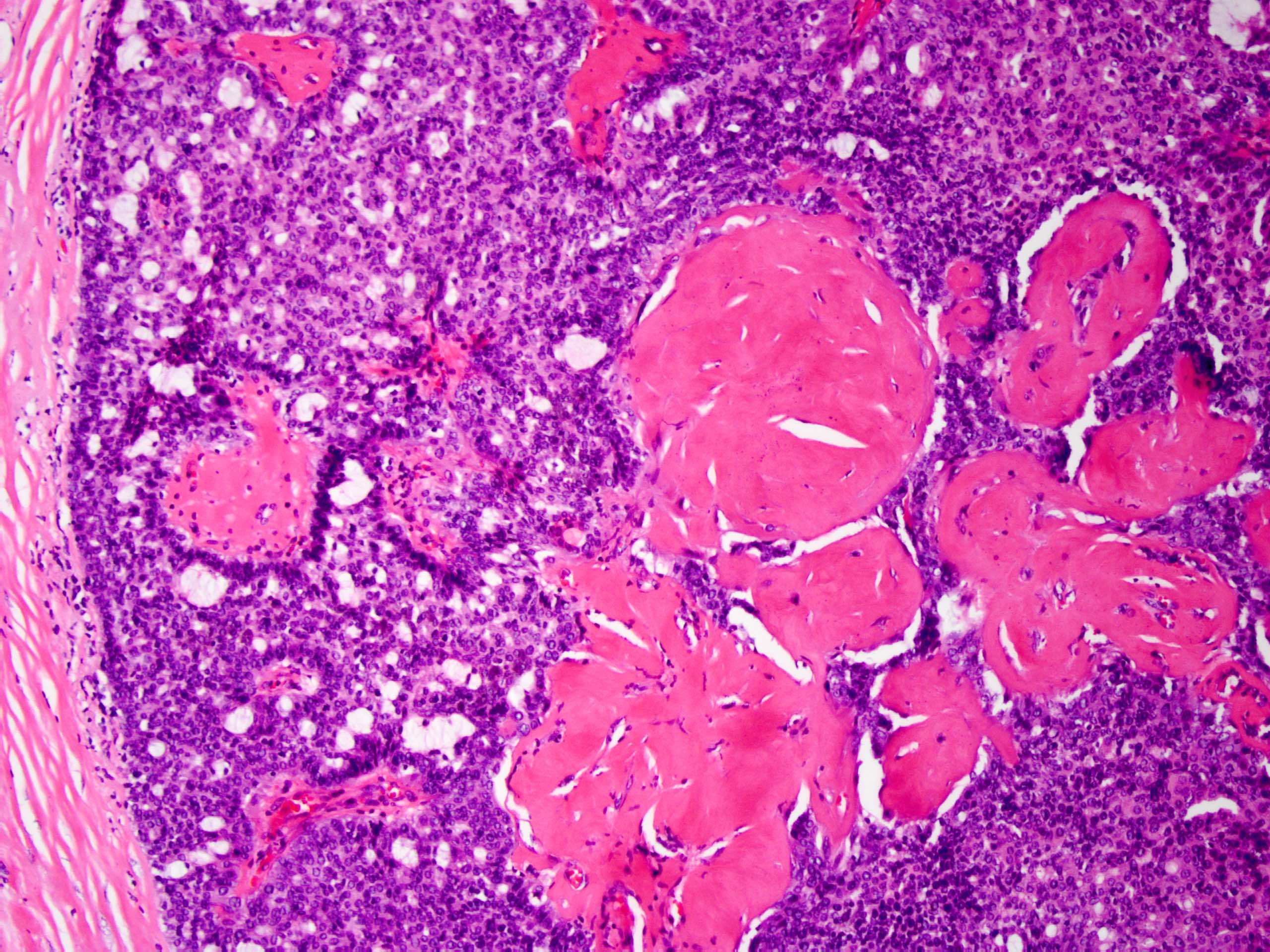
- Frequently associated with usual type ductal hyperplasia and apocrine metaplasia, less frequently squamous, osseous or chondroid metaplasia may be seen
- May undergo ischemic or hemorrhagic changes, either spontaneously or secondary to biopsy / trauma
- May show prominent fibrosis / sclerosis which may contained entrapped glands (sclerosing papilloma)
- May be involved by:
Microscopic (histologic) images
Contributed by Xiaoxian (Bill) Li, M.D., Ph.D.
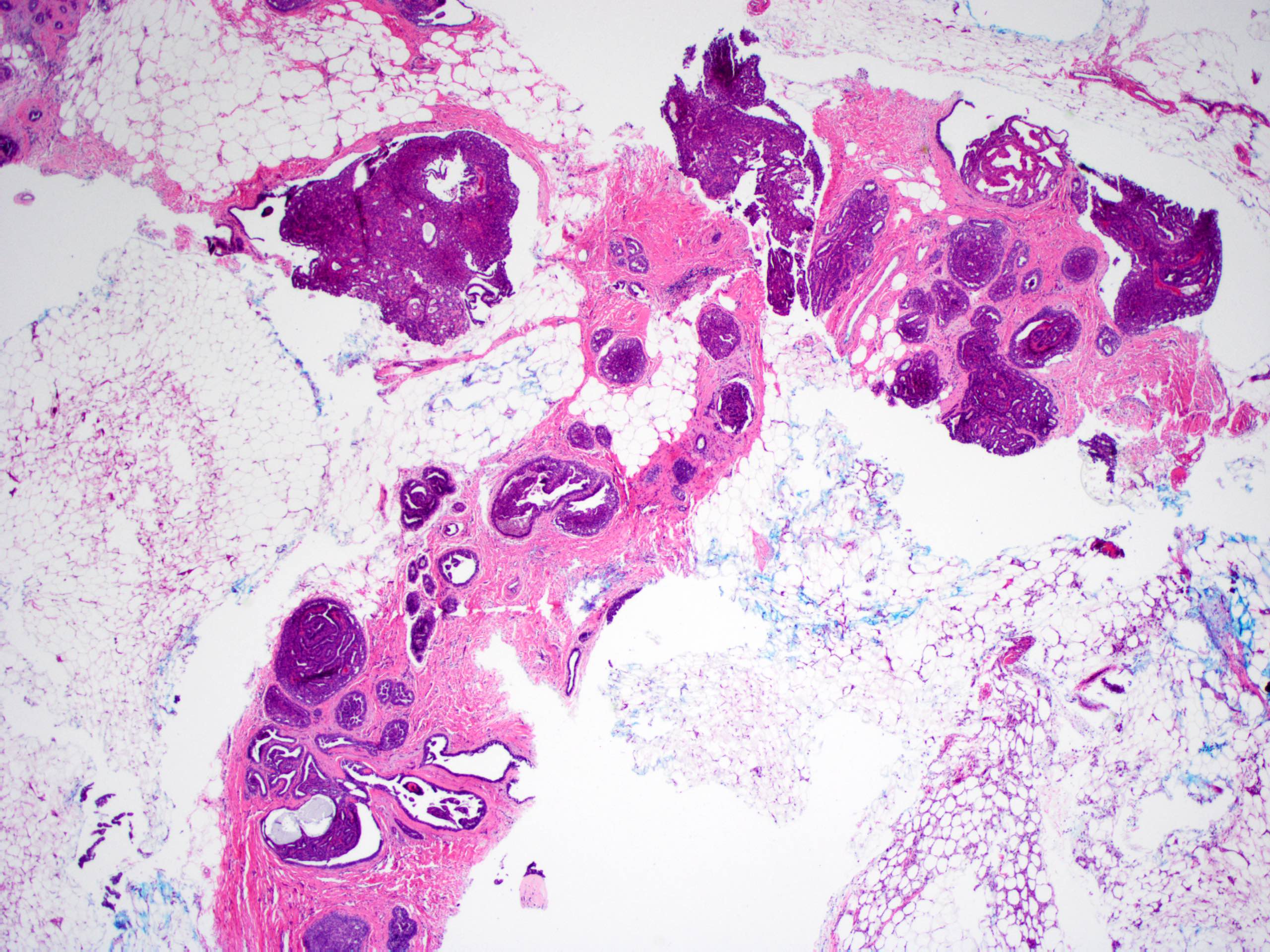
Minute intraductal papillomas
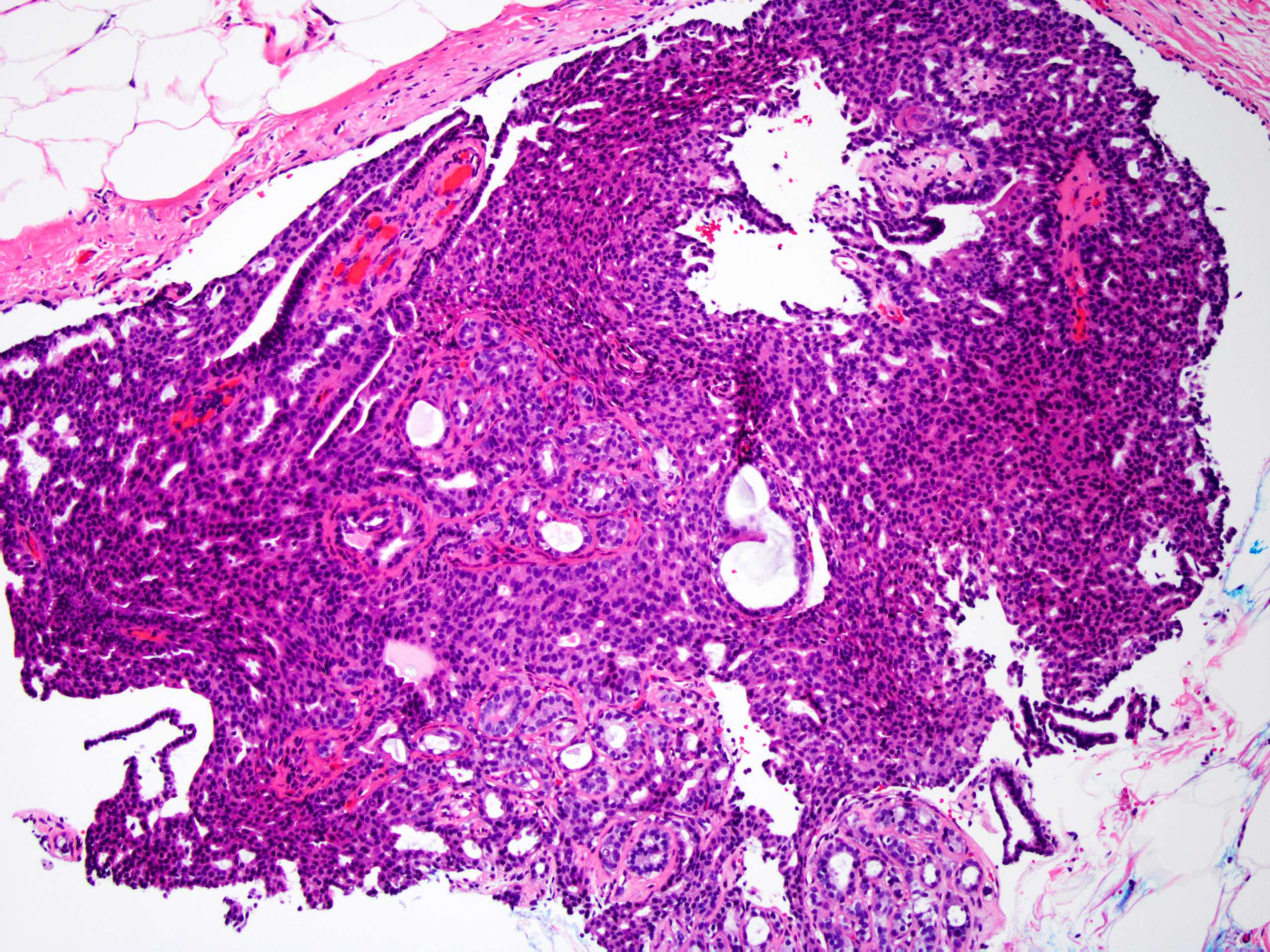
Papillary cores
Involved by usual ductal hyperplasia
Involved by apocrine metaplasia
Involved by ductal carcinoma in situ
Contributed by Jijgee Munkhdelger, M.D., Ph.D. and Andrey Bychkov, M.D., Ph.D.
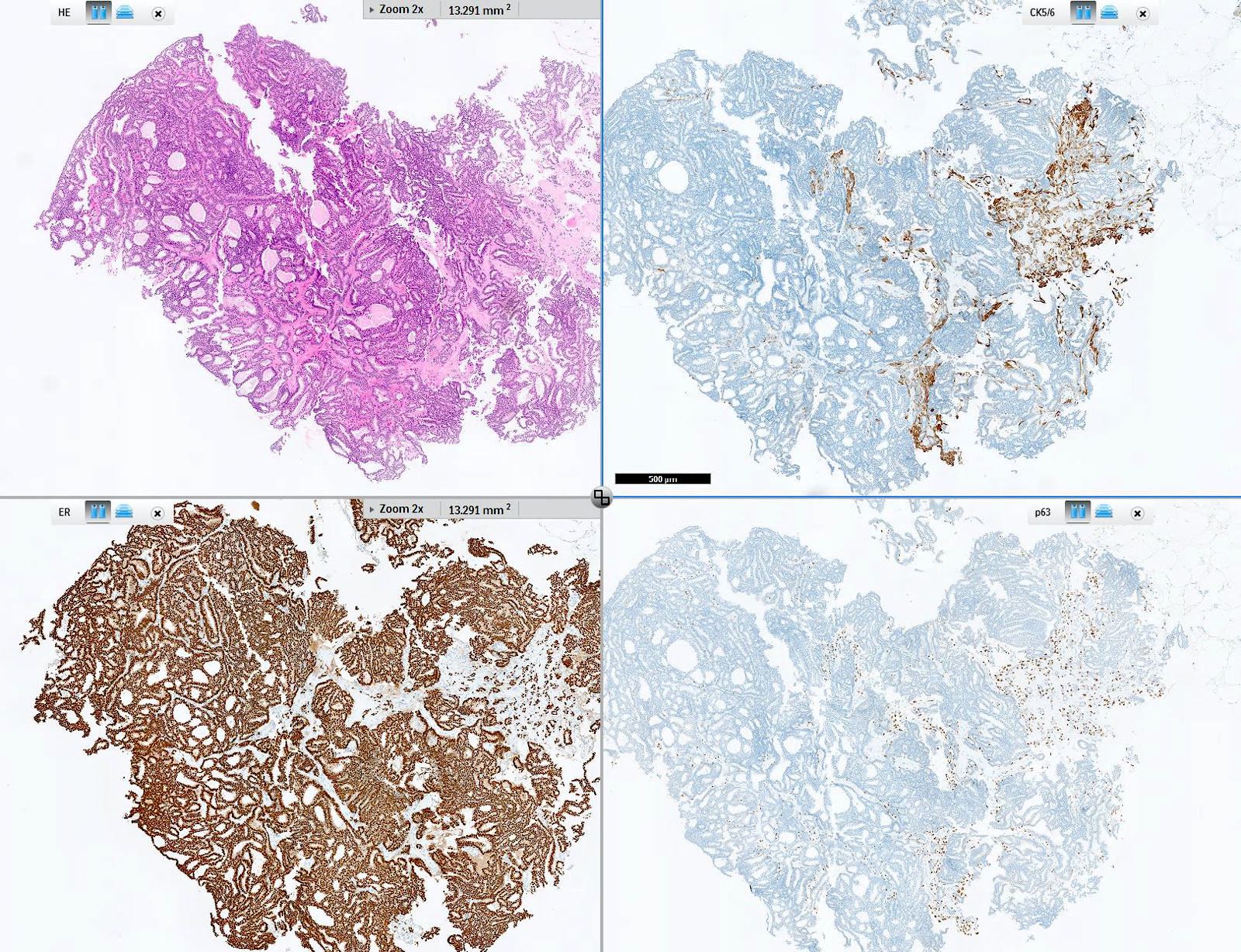
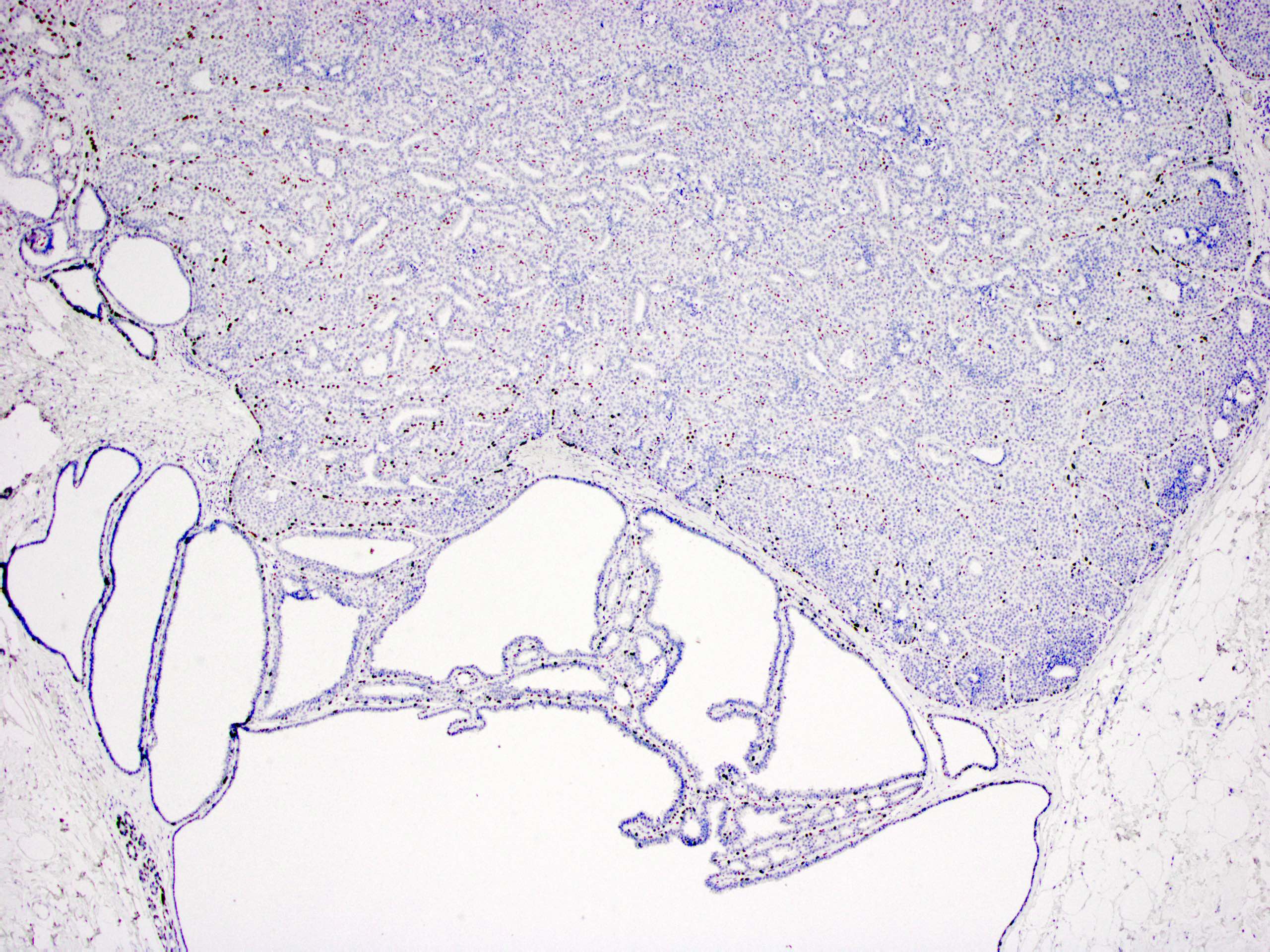
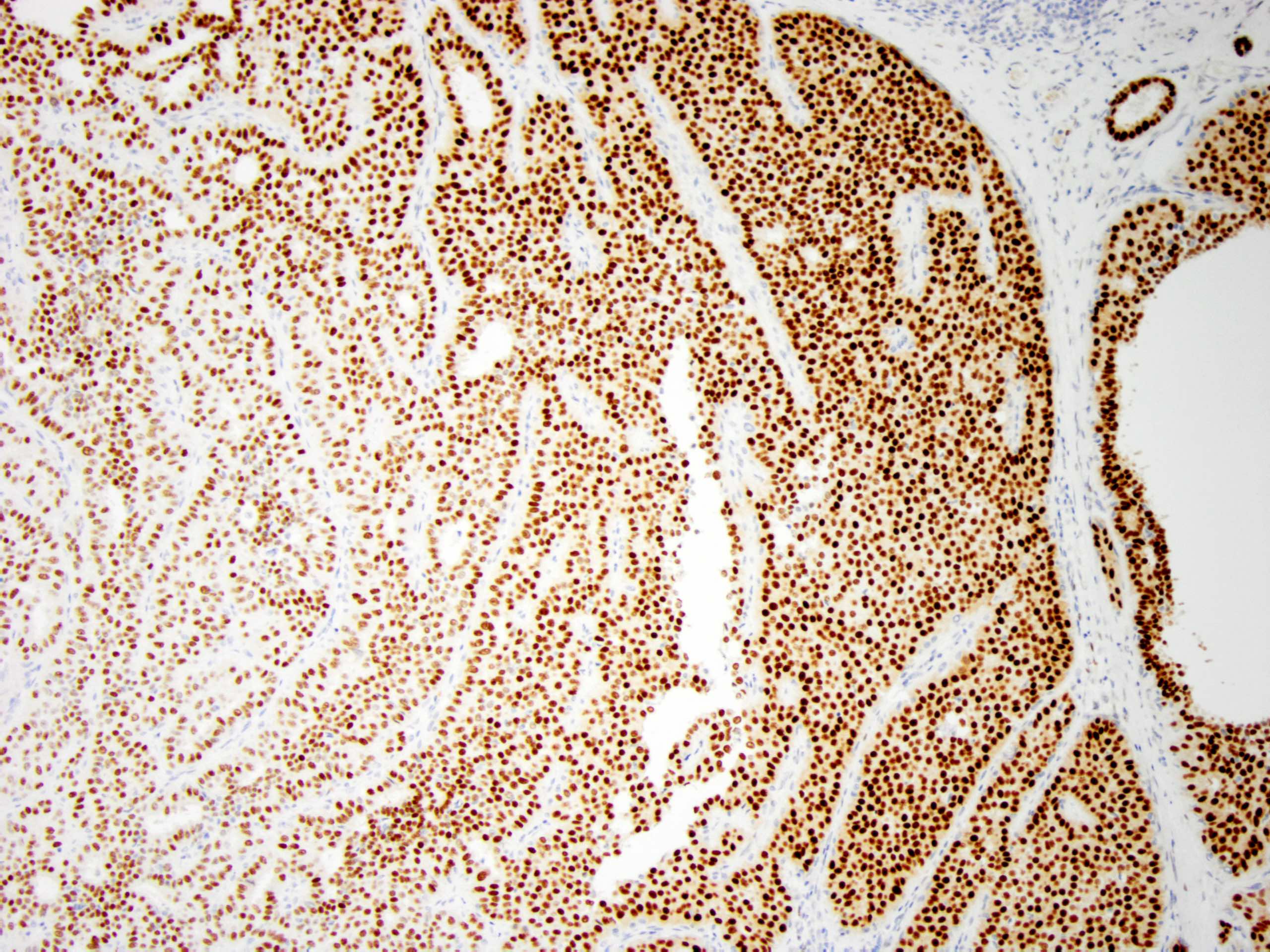
Intraductal papilloma with DCIS immunoprofile
Intraductal papilloma with DCIS, CK5/6
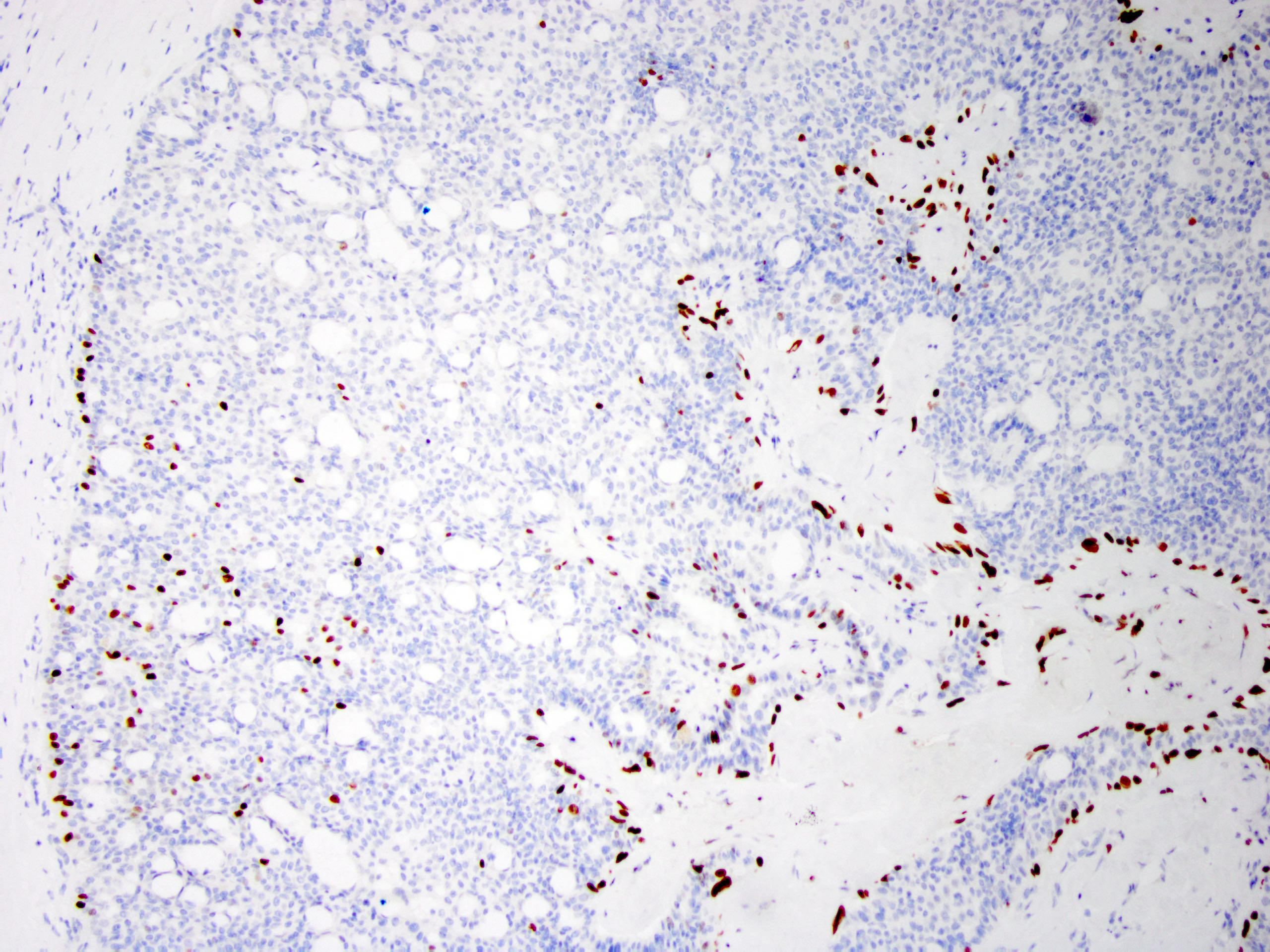
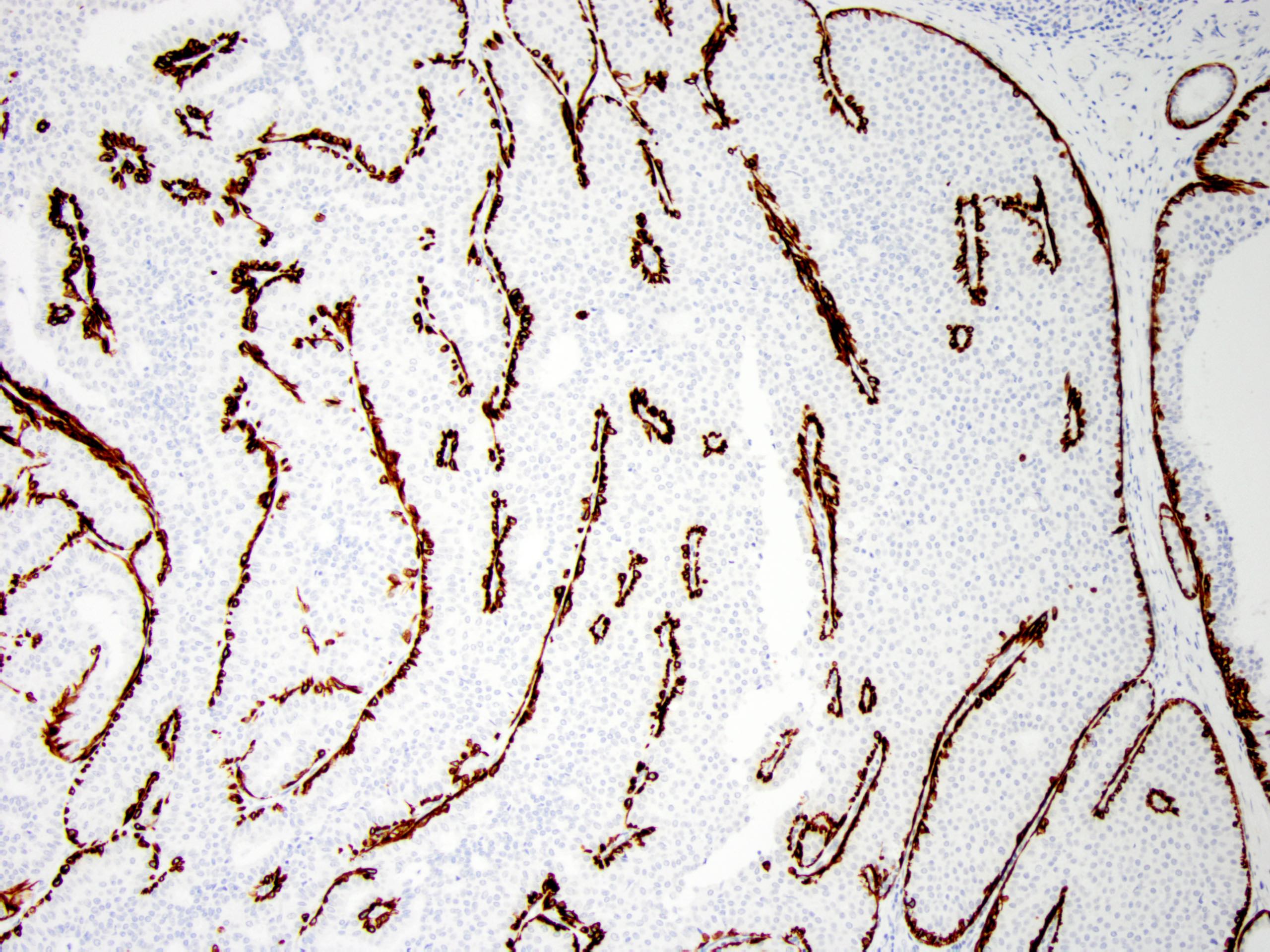
Intraductal papilloma with DCIS, p63
Virtual slides
Images hosted on other servers:

Sclerosing intraductal papilloma
Cytology description
- Large stellate tissue fragments of benign ductal cells in a proteinaceous background (Diagn Cytopathol 2007;35:386)
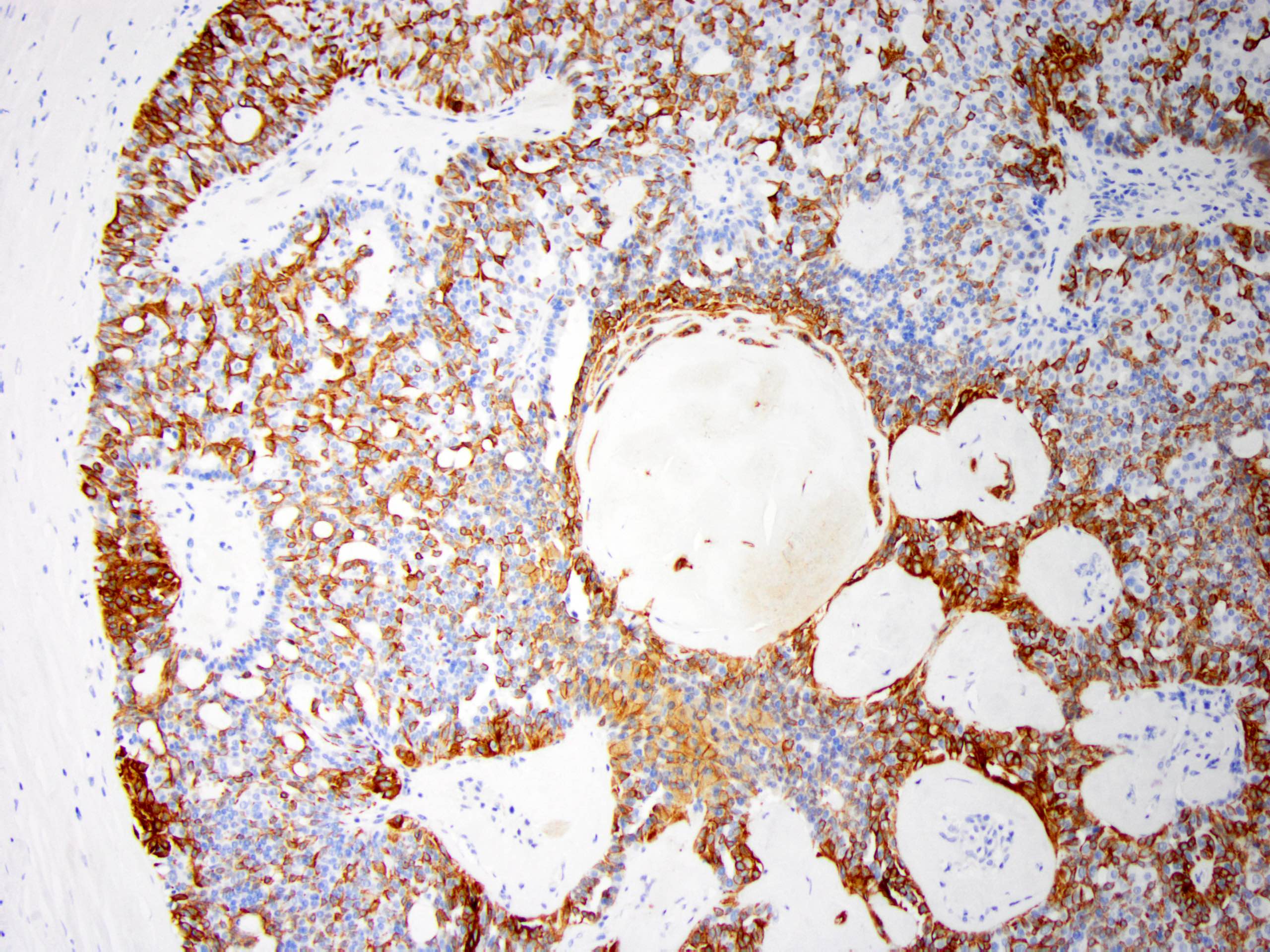
Positive stains
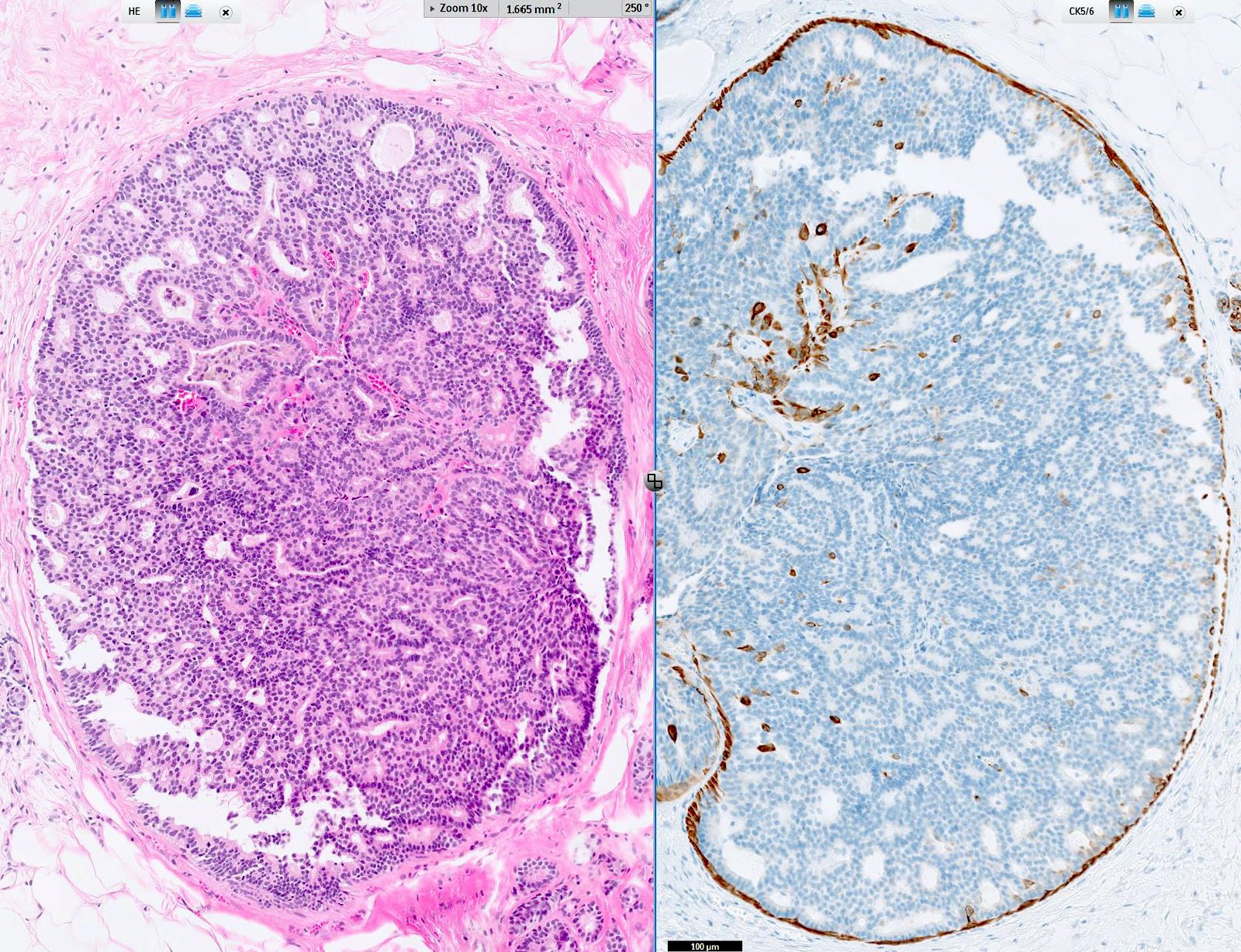
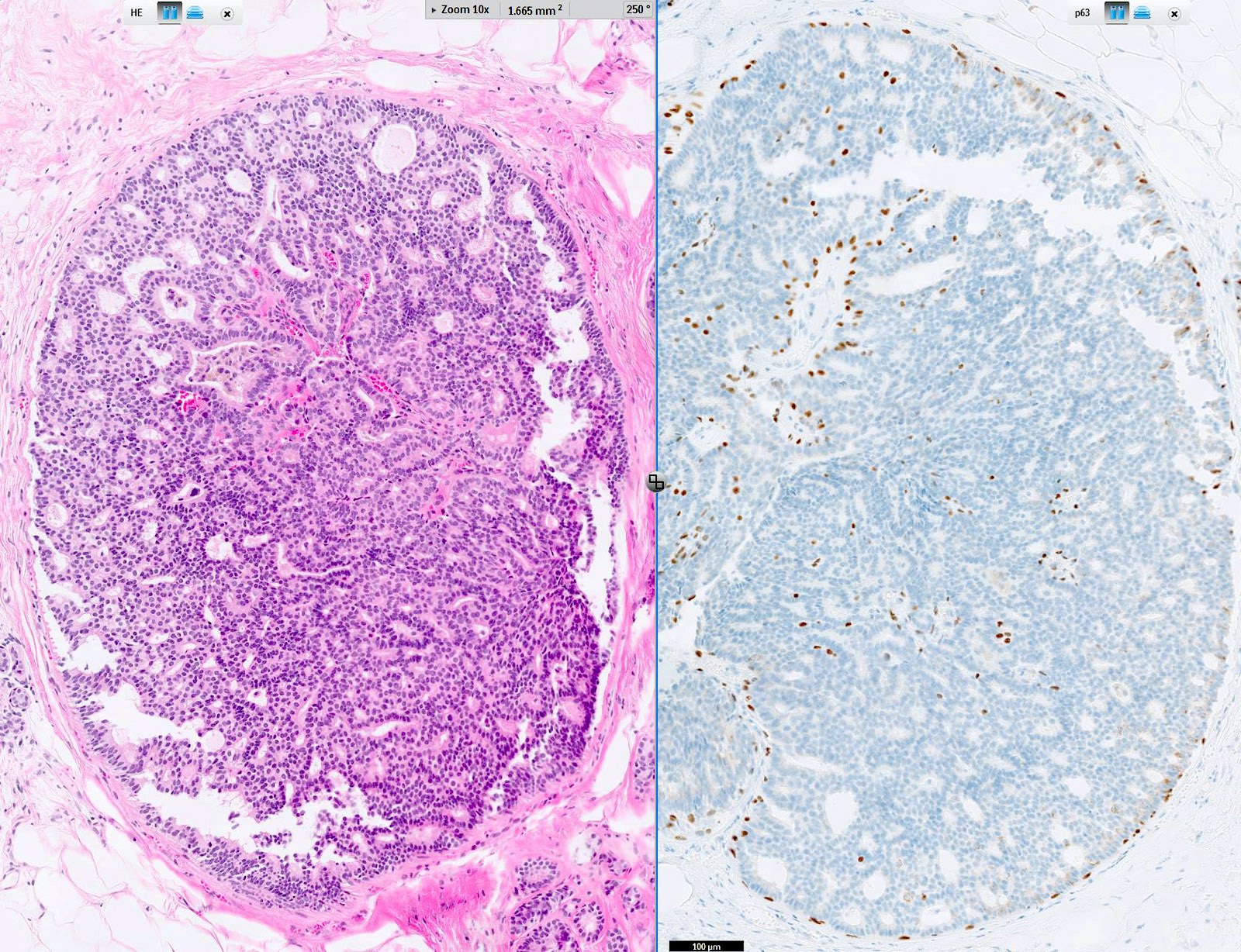
- Myoepithelial cell markers (CK5, p63, p40, calponin, alpha smooth muscle actin, smooth muscle myosin heavy chain / SMMHC) show myoepithelial cells in fibrovascular cores and at the periphery of the involved duct (Arch Pathol Lab Med 2016;140:628)
- In intraductal papilloma involved by usual ductal hyperplasia
- ER is patchy positive (Pathol Int 2012;62:381)
- CK5 is patchy positive in a mosaic pattern (Pathol Int 2012;62:381)
Molecular / cytogenetics description
- PIK3CA / AKT1 pathway mutations commonly involved (Mod Pathol 2010;23:27, Mod Pathol 2021;34:1044):
- AKT1 mutations are commonly seen in papilloma without (54%) or with mild hyperplasia (15%)
- PIK3CA mutations can be seen in 21 - 42% in papilloma with or without atypia
Videos
Intraductal papilloma
Sample pathology report
- Right breast, 9 o'clock, 1 cm from the nipple, ultrasound guided core biopsy:
- Intraductal papilloma with apocrine metaplasia
- Comment: Patchy positivity for CK5 and ER supports the above diagnosis.
Differential diagnosis
- Atypical ductal hyperplasia involving an intraductal papilloma (atypical papilloma) (Histopathology 2016;68:22):
- Monotonous low grade cellular proliferation
- Atypical proliferation is small (≤ 3 mm) (Cancer 1996;78:258, Am J Surg Pathol 2006;30:665)
- Decreased myoepithelial cells
- CK5/6 negative, ER diffusely positive
- Monotonous low grade cellular proliferation
- Intraductal papillary carcinoma (papillary DCIS) (Histopathology 2016;68:22):
- Encapsulated papillary carcinoma (Histopathology 2016;68:22):
- Adenomyoepithelioma (Mod Pathol 2021;34:1044, Mod Pathol 2020;33:1764, Am J Surg Pathol 1991;15:554):
- Rare, usually benign, well circumscribed nonencapsulated biphasic tumor with myoepithelial and epithelial components
- Multiple patterns (spindle cell, tubular, lobulated, papillary)
- Papillary pattern might be difficult to differentiate from intraductal papilloma
- In adenomyoepithelioma, myoepithelial cells are more conspicuous
- Invasive papillary carcinoma (Mod Pathol 2021;34:1044):
- Uncommon subtype of breast carcinoma
- Invasive carcinoma with > 90% papillary architecture
- Negative for myoepithelial cells
- Tall cell carcinoma with reverse polarity (Mod Pathol 2021;34:1044):
- Rare papillary lesion with uncertain malignant potential
- Distinctive morphology:
- Columnar epithelial cells with apically located nucleus with papillary, solid and follicular architecture
- Nuclei with clearing, groove and pseudoinclusion (reminiscent of tall cell variant of papillary thyroid carcinoma)
- Recurrent IDH2 R172 hotspot mutation
- Solid papillary carcinoma (Mod Pathol 2021;34:1044):
- Uncommon subtype of breast carcinoma
- Expansile solid nodules with interspersed fibrovascular cores composed of monotonous atypical cells (low or intermediate grade)
- Considered as an in situ disease
- Myoepithelial cells may be attenuated at the periphery
Practice question #1
Regarding this breast specimen, what is the correct diagnosis?
- Intraductal papillary carcinoma
- Intraductal papilloma with apocrine metaplasia
- Intraductal papilloma with DCIS
- Intraductal papilloma with LCIS
- Invasive papillary carcinoma
Practice answer #1
B. This intraductal papilloma shows typical features of apocrine metaplasia.
Comment Here
Reference: Intraductal papilloma
Comment Here
Reference: Intraductal papilloma
Practice question #2
What is the staining pattern of p63 for intraductal papilloma of the breast without atypia?
- At the periphery of involved duct only
- In the fibrovascular cores only
- Intraductal papillomas do not stain for p63
- At the periphery and in the fibrovascular cores
Practice answer #2
D. p63 stain for myoepithelial cells is positive throughout the lesion, including in the fibrovascular cores and at the periphery of the involved duct.
Comment Here
Reference: Intraductal papilloma
Comment Here
Reference: Intraductal papilloma
Practice question #3
What is the typical staining pattern of atypical epithelial proliferation involving an intraductal papilloma of the breast?
- Diffusely positive for ER and patchy positive for CK5/6, negative for p63
- Diffusely positive for ER, negative for p63 and CK5/6
- Diffusely positive for ER, p63 and CK5/6
- Negative for ER, p63 and CK5/6
- Patchy positive for ER, negative for p63 and CK5/6
Practice answer #3
B. The atypical low grade epithelial proliferation is diffusely positive for ER, negative for CK5/6 and negative for p63.
Comment Here
Reference: Intraductal papilloma
Comment Here
Reference: Intraductal papilloma
