Adrenal gland & paraganglia
Neuroblastic tumors
Ganglioneuroblastoma, intermixed and nodular
Authors: Carmen M. Perrino, M.D., Debra L. Zynger, M.D.


Last author update: 1 August 2014
Last staff update: 16 January 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Ganglioneuroblastoma
Table of Contents
Definition / general | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Molecular / cytogenetics images | Differential diagnosisCite this page: Perrino C, Zynger DL. Ganglioneuroblastoma, intermixed and nodular. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/adrenalganglioneuroblastoma.html. Accessed September 9th, 2025.
Definition / general
- Neoplasm of neuroectodermal origin comprised of mixture of neuroblasts and ganglion cells in varying proportions
- Divided into stroma rich (well differentiated, intermixed, nodular) and stroma poor categories depending on amount of Schwannian, spindle cell stroma
- Intermixed: composite tumor in the stroma rich category
- Ganglioneuromatous tissue with interspersed, sharply defined, unencapsulated nests of variably differentiated neuroblastic cells
- Nodular: composite tumor in the stroma rich category
- Predominance of differentiated Schwannian type stroma associated with ≥ 1 macroscopically visible nodule(s) of neuroblasts showing neuropil formation but lacking Schwannian stroma (stroma poor nodule) (Mod Pathol 2015;28:166)
- Grossly identifiable mature and immature components may either both be in primary tumor or one may be in primary and one in metastasis (Lack: Tumors of the Adrenal Glands and Extraadrenal Paraganglia, AFIP, 2007))
Epidemiology
- 4th most common tumor in childhood
- 75 - 85% occur within first 4 years of life
- M = F
Sites
- Occur anywhere in anatomic distribution of sympathoadrenal neuroendocrine system
- ~80% arise within abdomen or adrenal gland
- ~20% within thoracic cavity
Etiology
- Clonal proliferation of immature cells of neural crest origin
Clinical features
- Asymptomatic
- Abdominal / back mass
- Watery diarrhea due to production of vasoactive intestinal polypeptide (Lack: Tumors of the Adrenal Glands and Extraadrenal Paraganglia, Volume 8, AFIP, Series 4)
- Patients with favorable histology lesions usually present with localized disease (stage I, II, III) (Pediatr Blood Cancer 2009;53:563)
- Patients with unfavorable histology lesions present with distant metastases in > 50% of cases (stage IV) (Pediatr Blood Cancer 2009;53:563)
Diagnosis
- 60 - 70% are advanced stage (III, IV) or have metastases at diagnosis (J Clin Oncol 1993;11:1466)
Laboratory
- Increased urine catecholamine metabolites (homovanillic acid, vanillylmandelic acid)
- Increased urine / serum dopamine as adjunct laboratory test
Radiology description
- MRI: hypointensity on T1 weighted image with rapid enhancement and hyperintensity on T2 weighted image (Intern Med 1995;34:1168)
Radiology images
Image hosted on other servers:
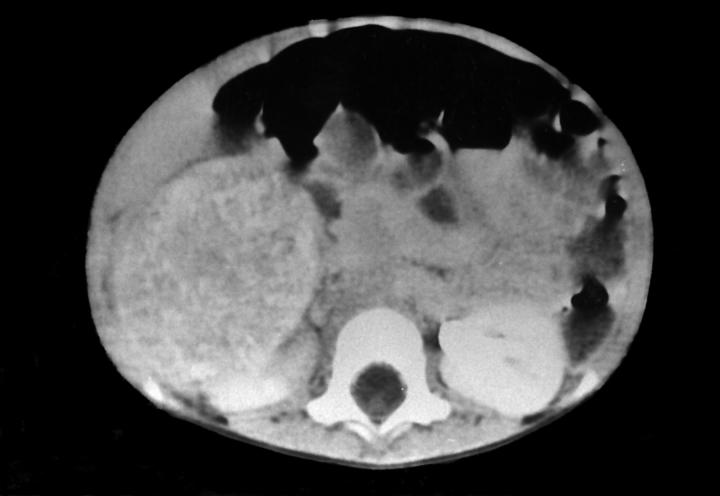
Spiral CT: hyperechoic mass
Prognostic factors
- Multiple classification systems have been developed with the goal of stratifying patients into prognostic groups (see staging - neuroblastic tumors)
- In Shimada Classification, intermixed type is favorable histology
- Nodular subtype was initially categorized as unfavorable histology and in 2003, the INPC created 2 prognostically different subsets within this subtype (Cancer 2003;98:2274, Cancer 2000;89:1150)
- Favorable subset: composed of Schwannian rich, stroma dominant component favorable nodule(s)
- Poorly differentiated or differentiating neuroblastoma: mitosis karyorrhexis index ([MKI] count of cells undergoing mitosis or karryhorexis, based on 5,000 cell count from random fields) ≤ 200, age < 1.5 years
- Differentiating neuroblastoma: MKI < 100, age 1.5 - 5 years
- Unfavorable subset: composed of unfavorable nodule(s)
- Any neuroblastoma, MKI > 200, any age
- Any neuroblastoma, MKI 100 - 200, > 1.5 years
- Undifferentiated neuroblastoma, any age
- Poorly differentiated neuroblastoma, age > 1.5 years
- Any neuroblastoma, age > 5 years
Treatment
- Depends on prognostic stage (Pediatr Blood Cancer 2009;53:563, UpToDate: Treatment and prognosis of neuroblastoma)
- Low risk
- Surgical resection alone is mainstay
- Chemotherapy only if tumor is unresectable or symptoms of spinal cord / respiratory / bowel compromise
- Expectant observation in some infants with small adrenal masses, localized neuroblastoma or asymptomatic stage 4S disease
- Intermediate risk
- Surgical resection
- Moderate chemotherapy
- Radiation only if disease progresses despite surgery / chemotherapy
- High risk
- Induction: intensive chemotherapy
- Local control: surgical resection, radiation
- Consolidation: chemotherapy, myeloablative therapy, autologous stem cell transplant
- Maintenance: cis-retinoic acid or immunotherapy
- Low risk
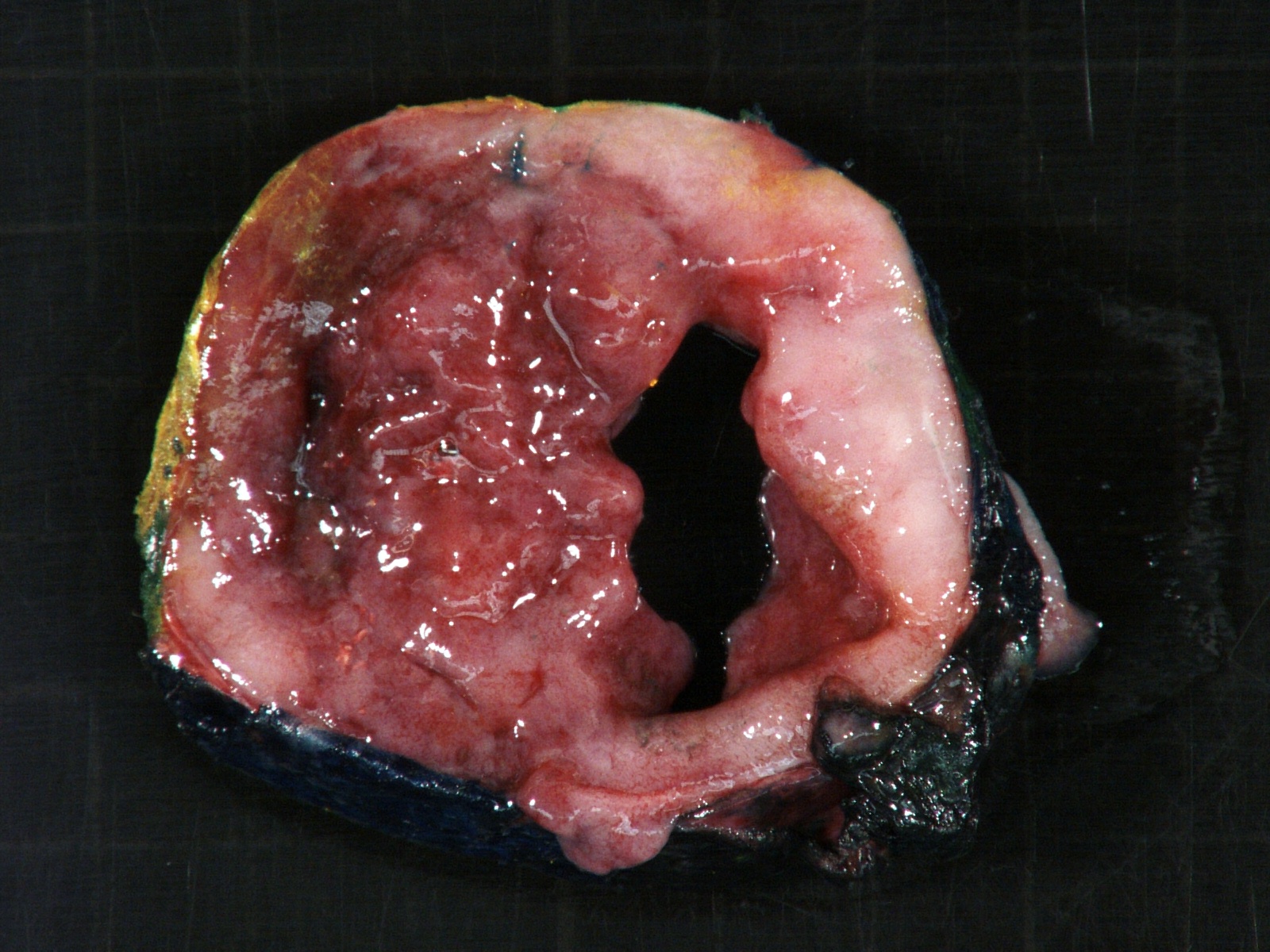
Gross description
- More homogeneous and mature appearance than neuroblastoma
- Varies by subtype, from circumscribed ovoid mass to large multilobulated tumor
- Stroma rich, nodular subtype: area(s) of stroma poor, immature tumor are usually hemorrhagic with well defined borders (J Natl Cancer Inst 1984;73:405)
- Calcification (chalky white, yellow areas) and cystic degeneration may occur
- If large, adrenal gland may be difficult to identify
Gross images
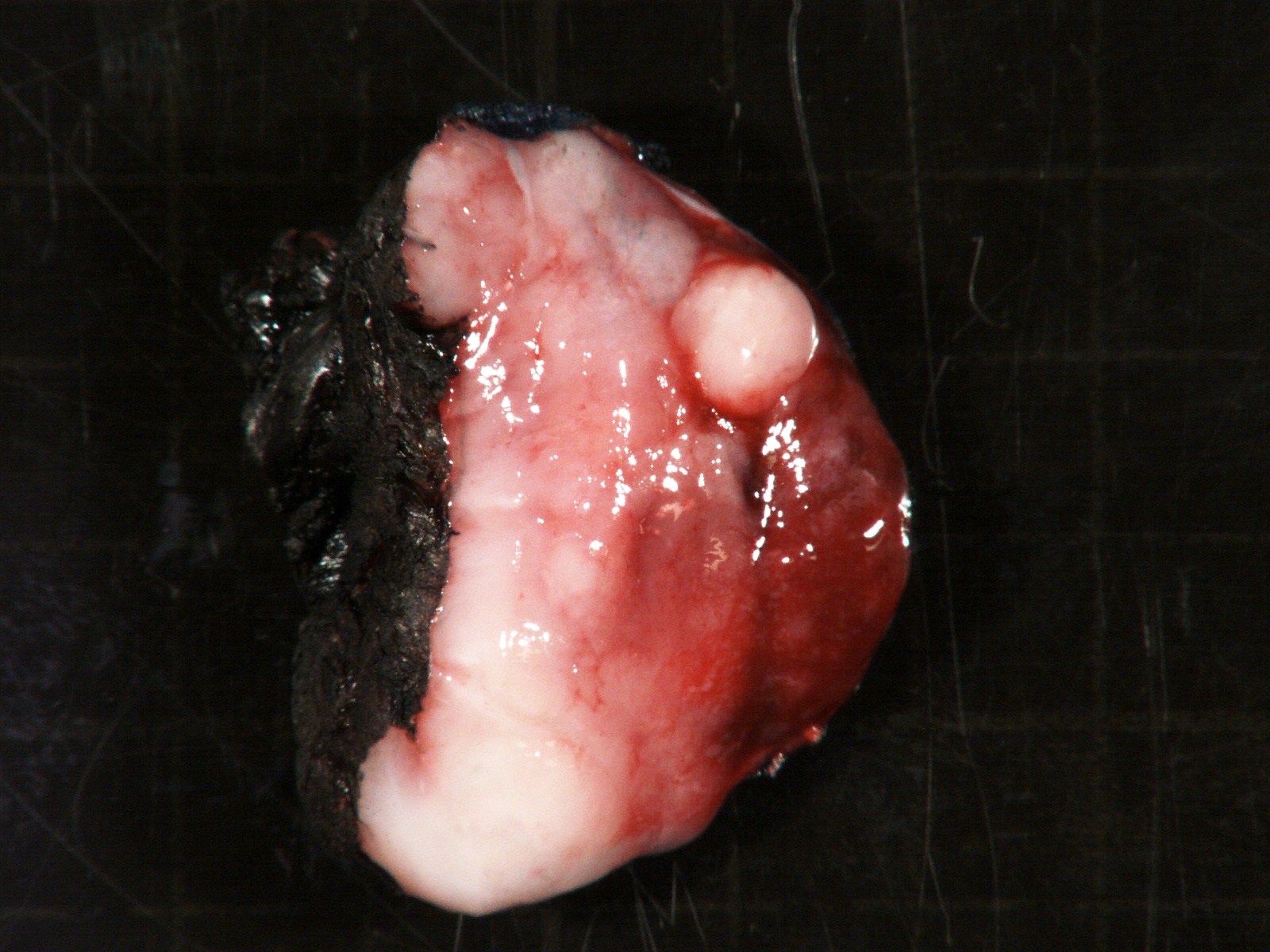
Contributed by Carmen Perrino, M.D. and Debra L. Zynger, M.D.
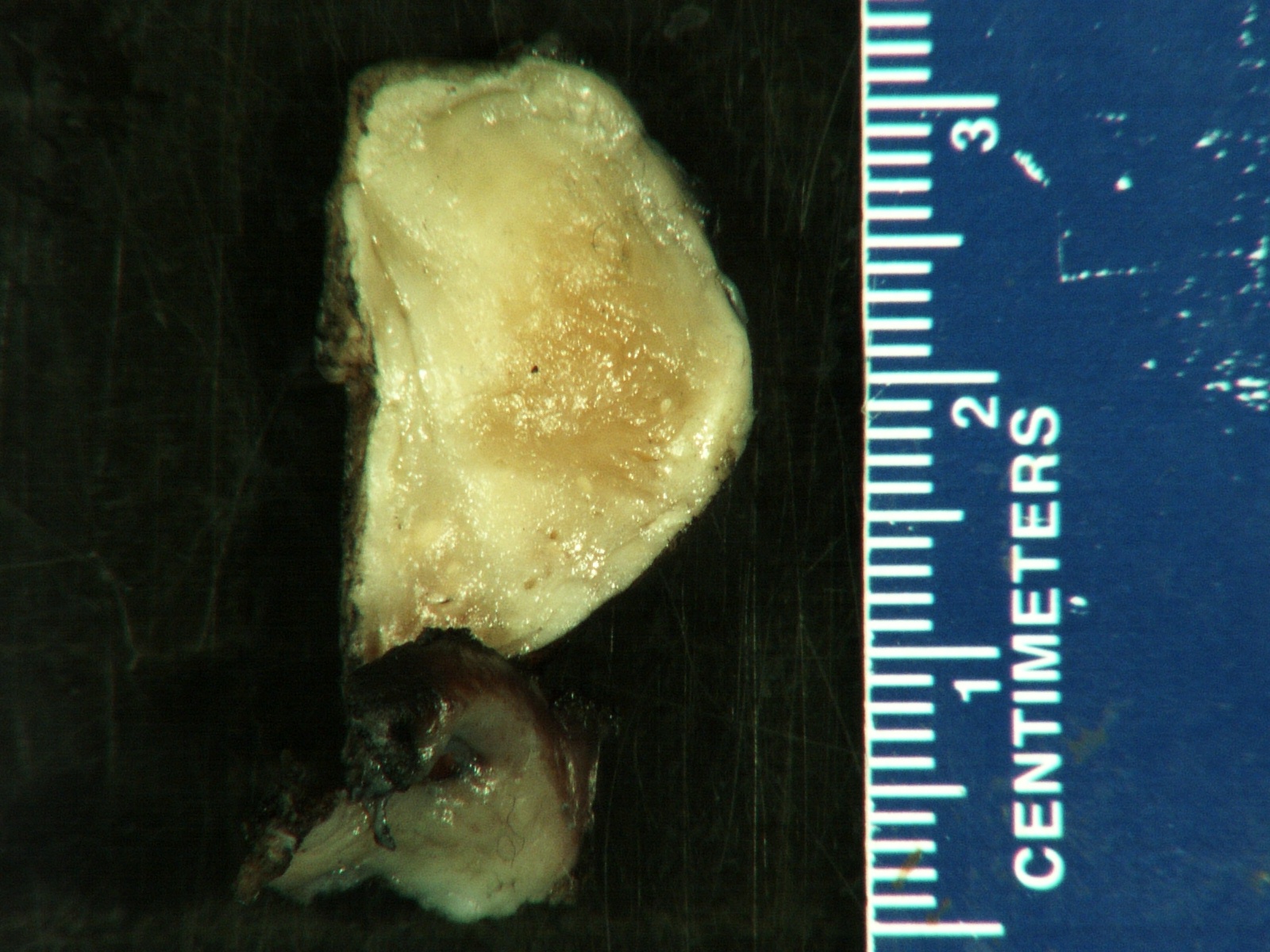
Stroma rich, intermixed type
Focal undifferentiated component
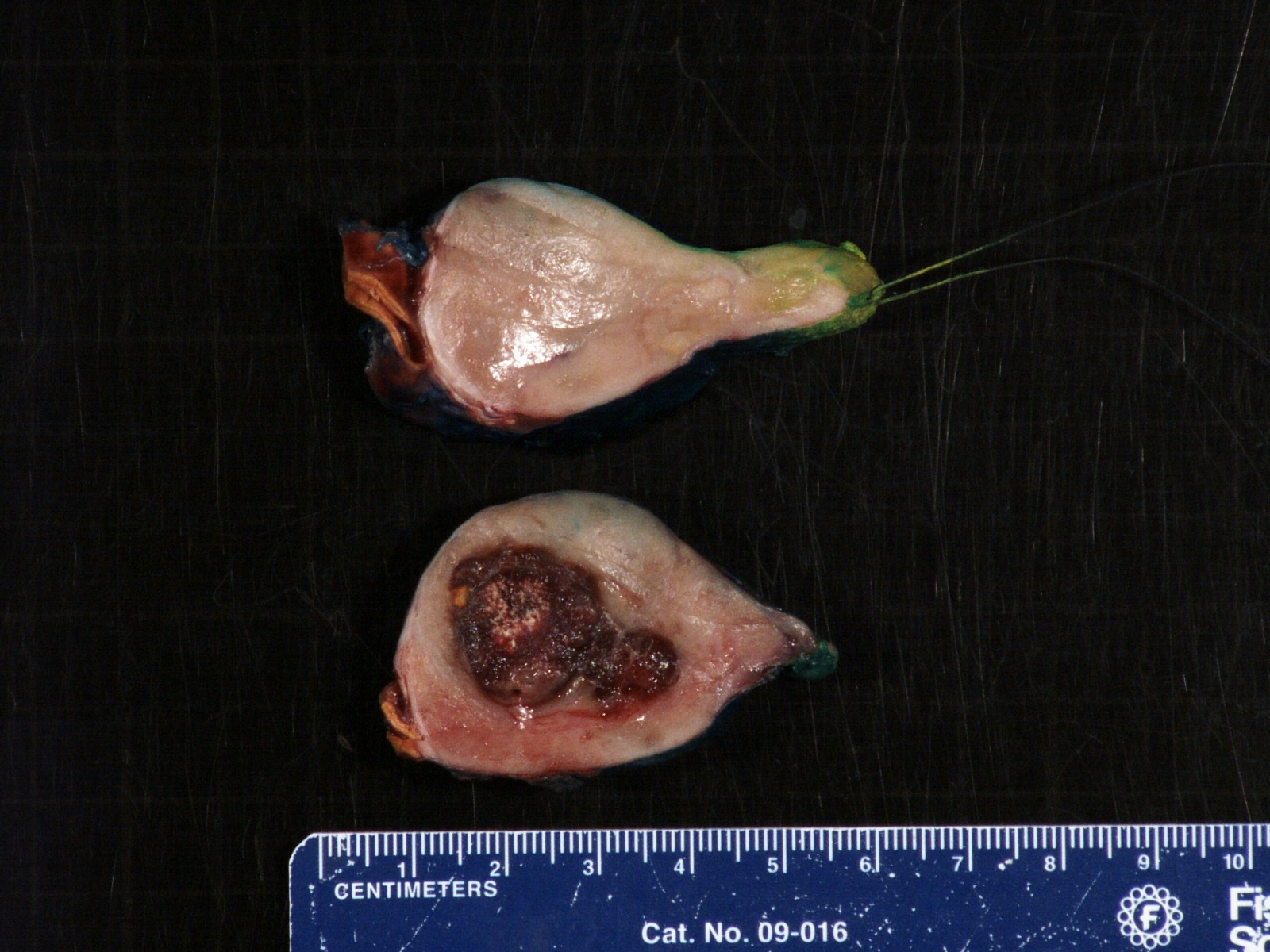
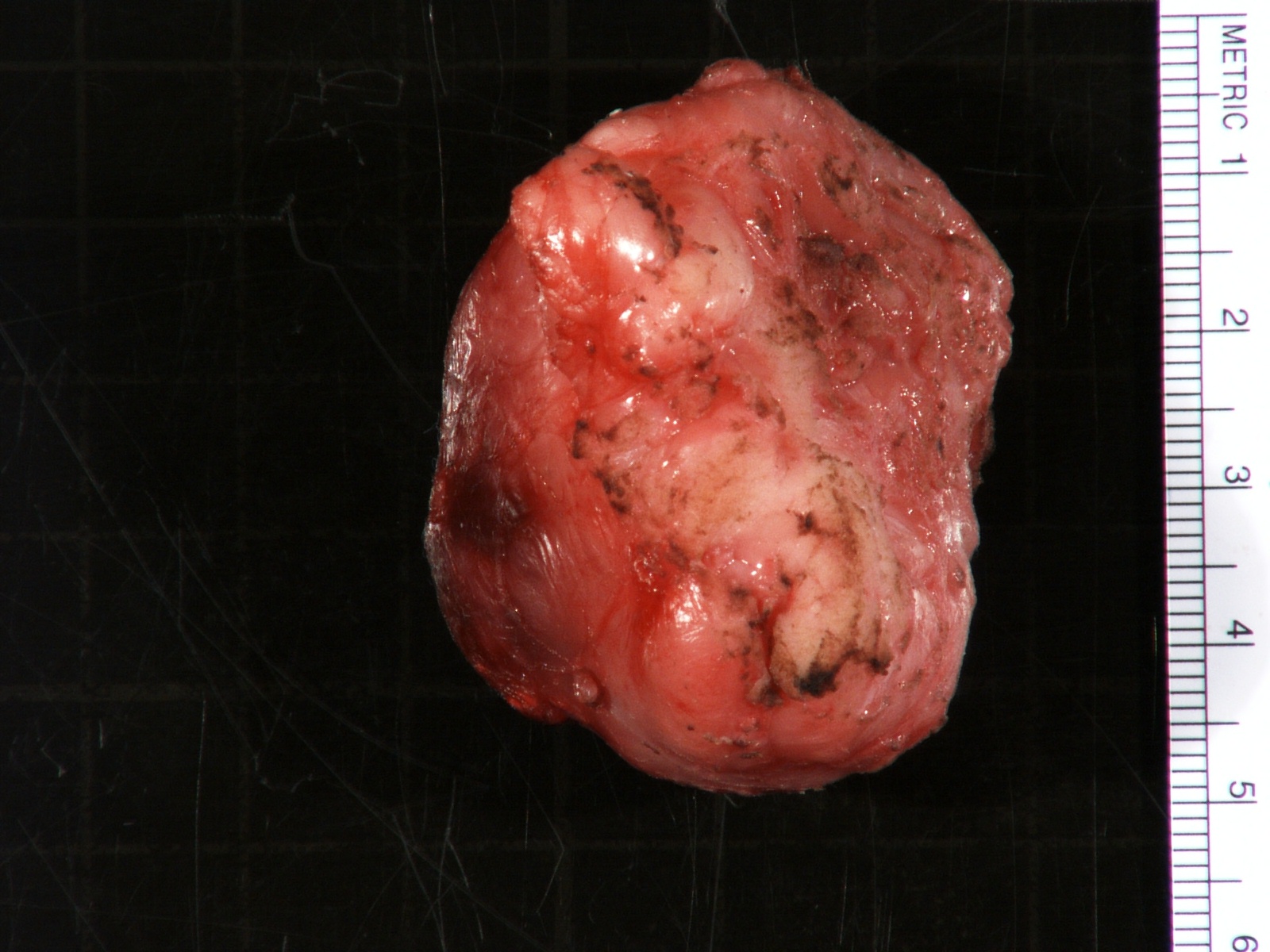
Stroma rich, nodular type
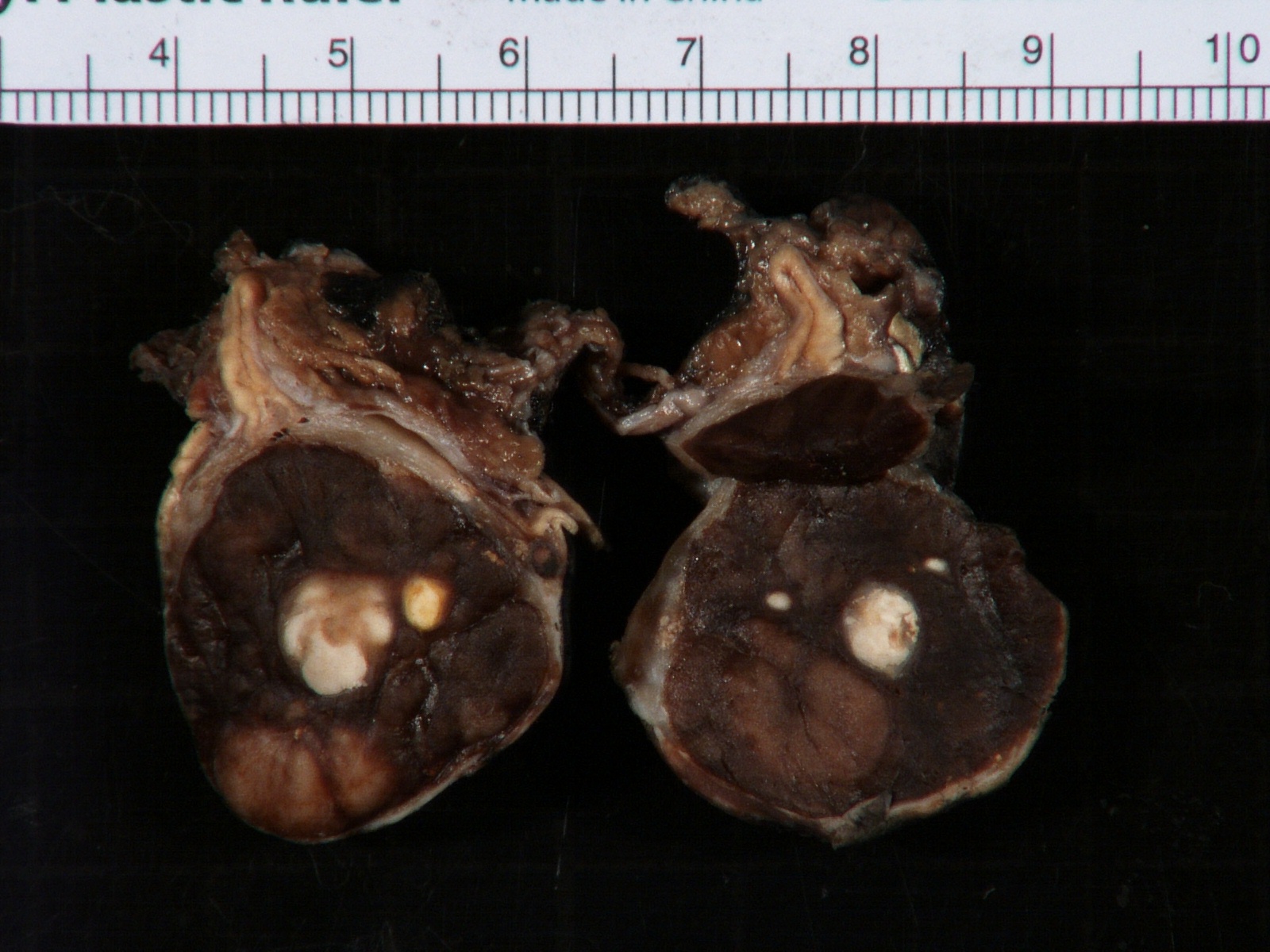
With treatment related changes
Microscopic (histologic) description
- Architecture: lobular, diffuse / solid, organoid
- Neuroblasts
- Homer Wright pseudorosettes = circular, ovoid, angular zones of pale staining neuritic cell processes surrounded by tumor cell nuclei; may rarely palisade
- Minimal cytoplasm, may have cytoplasmic tail
- Round to ovoid nuclei with stippled salt and pepper chromatin, inconspicuous nucleoli
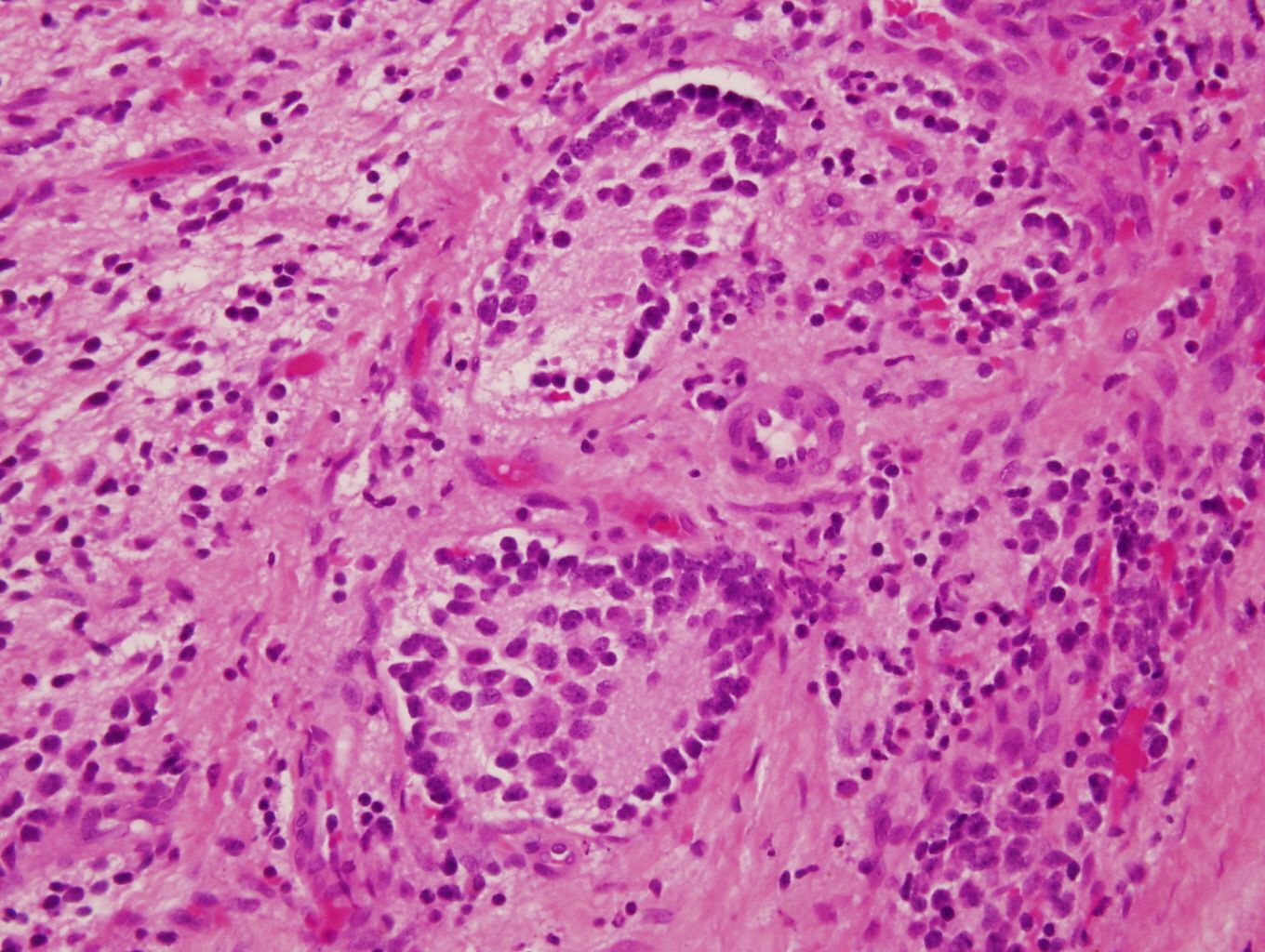
- Ganglion cells
- Abundant granular eosinophilic cytoplasm (Nissl substance = rough endoplasmic reticulum)
- Distinct cell borders
- Nuclear enlargement, eccentric nuclei, prominent nucleoli
- May see neuromelanin pigment (brown, finely granular; rarely present), cystic degeneration, hemorrhage, dystrophic calcification
Microscopic (histologic) images
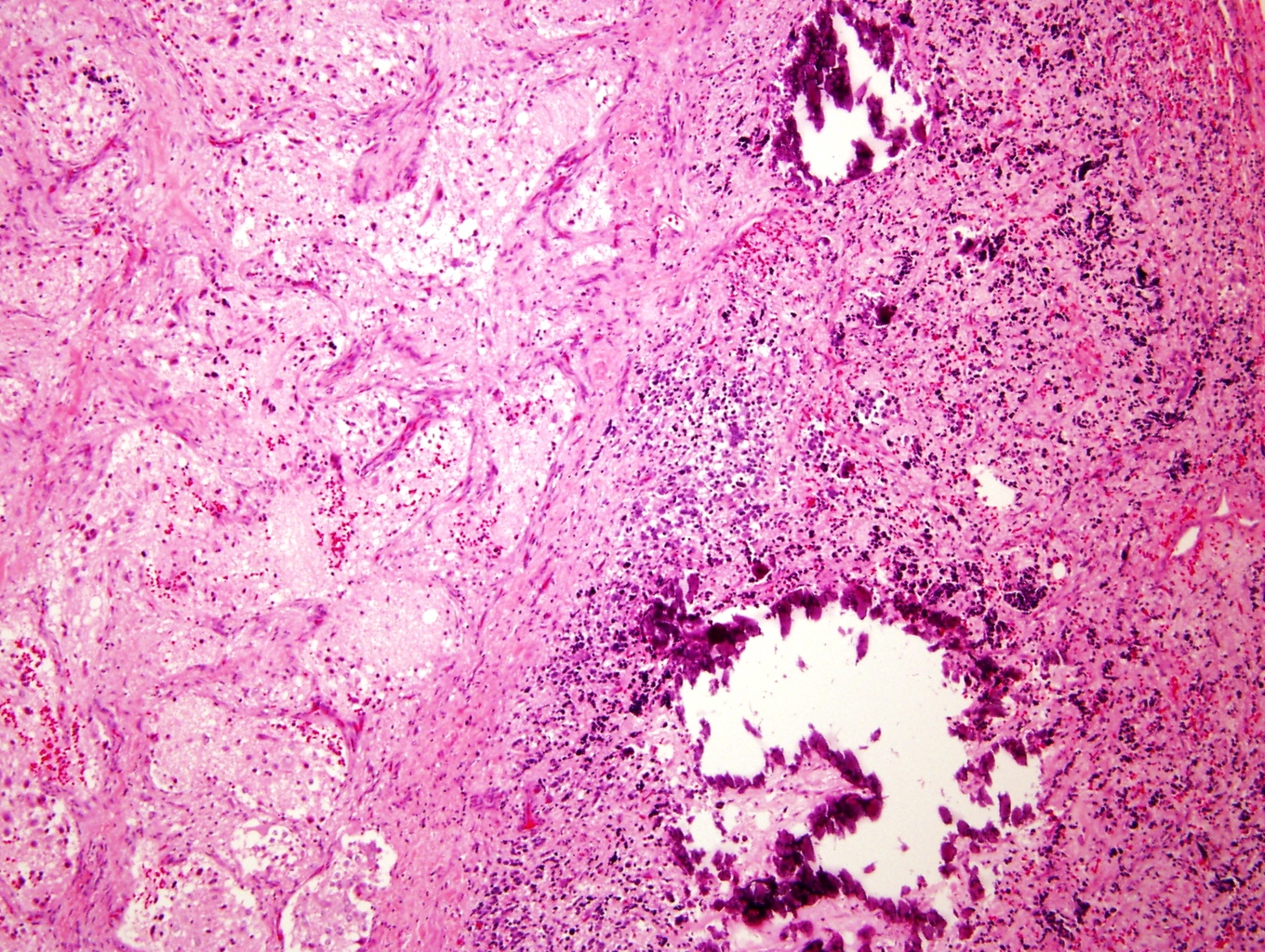
Contributed by Carmen Perrino, M.D. and Debra L. Zynger, M.D.
Intermixed type
Composite types
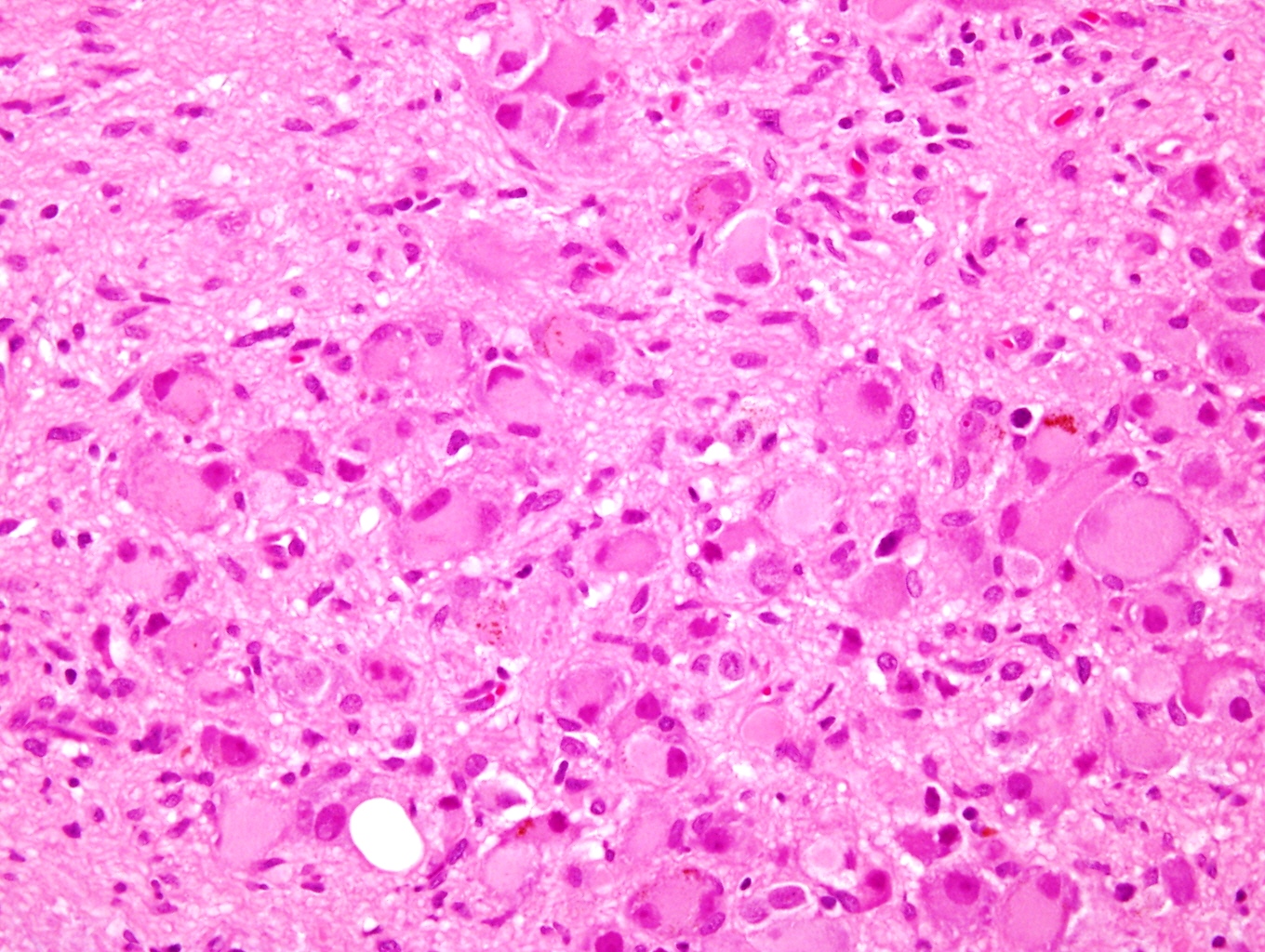
Intermixed type
Ganglion cells
Fibrillary background
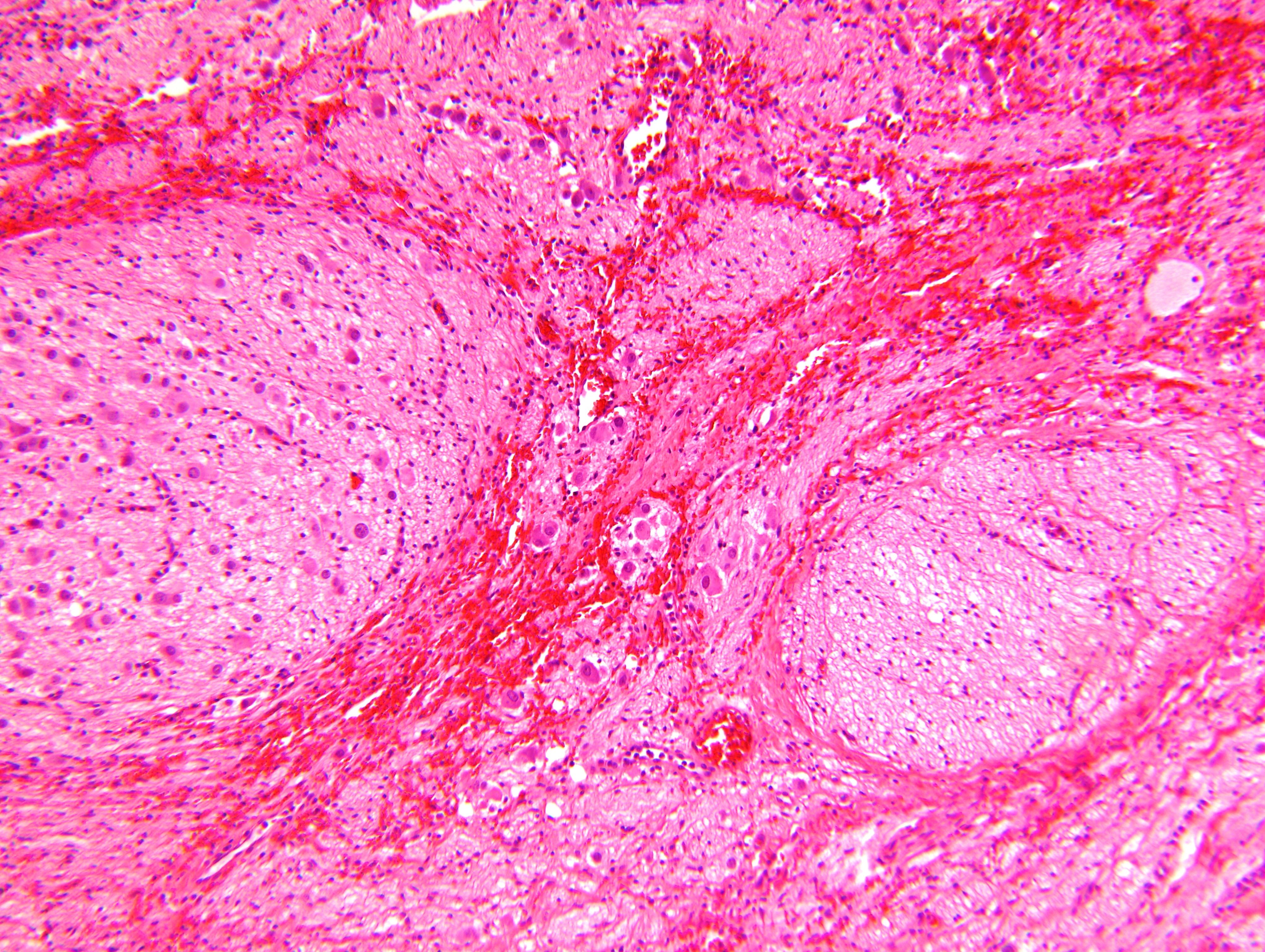
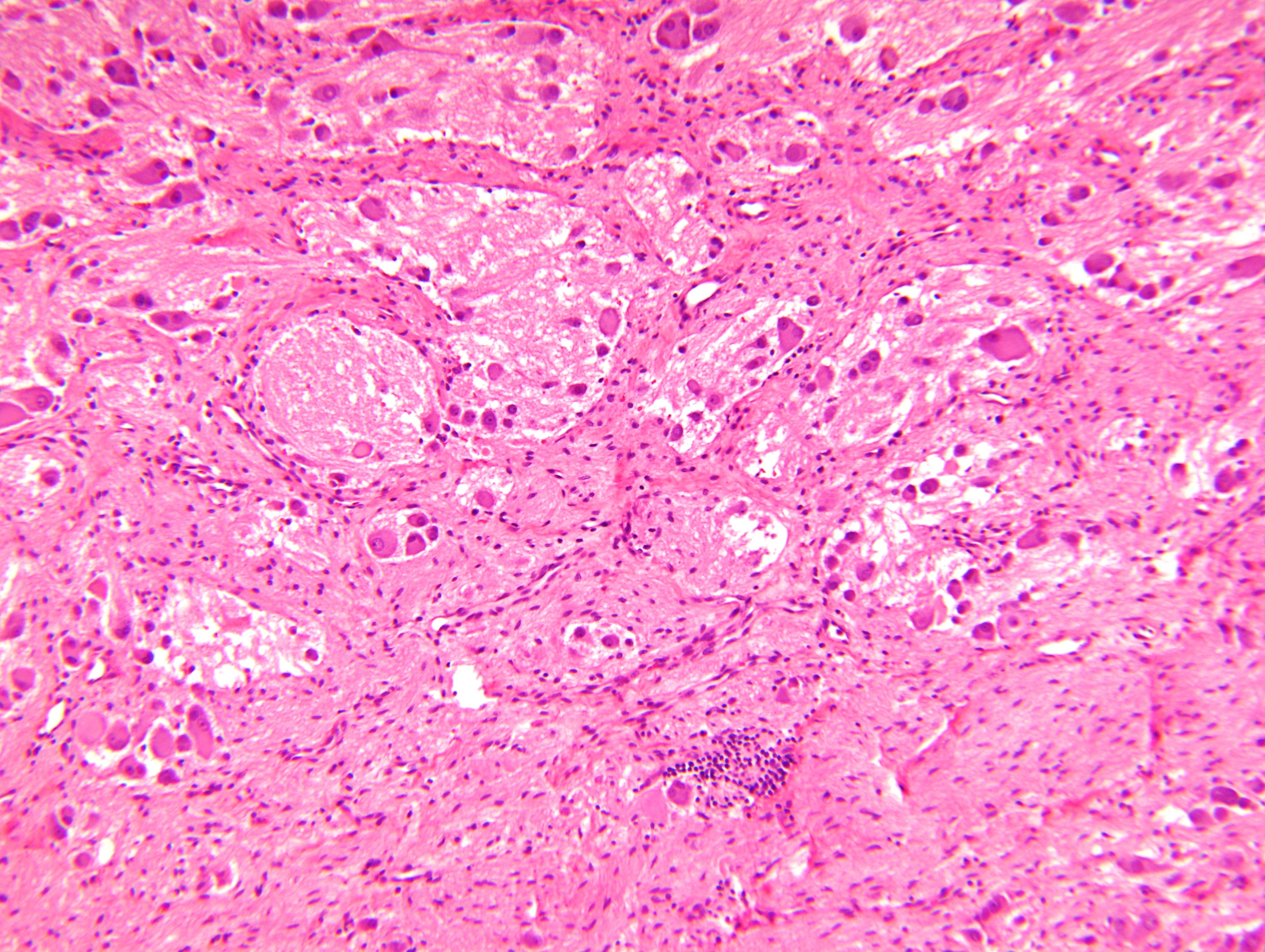
Aggregate of ganglion cells
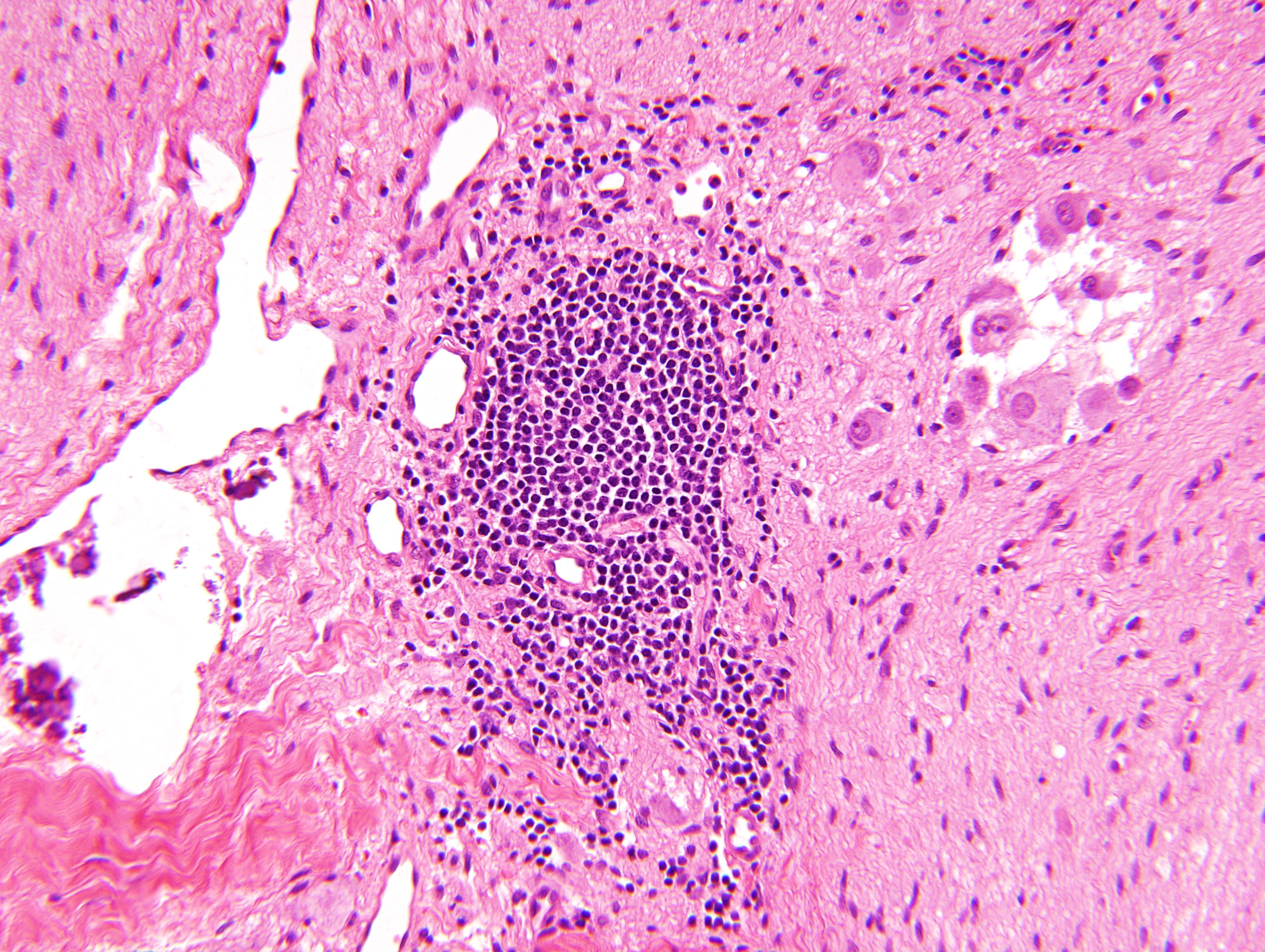
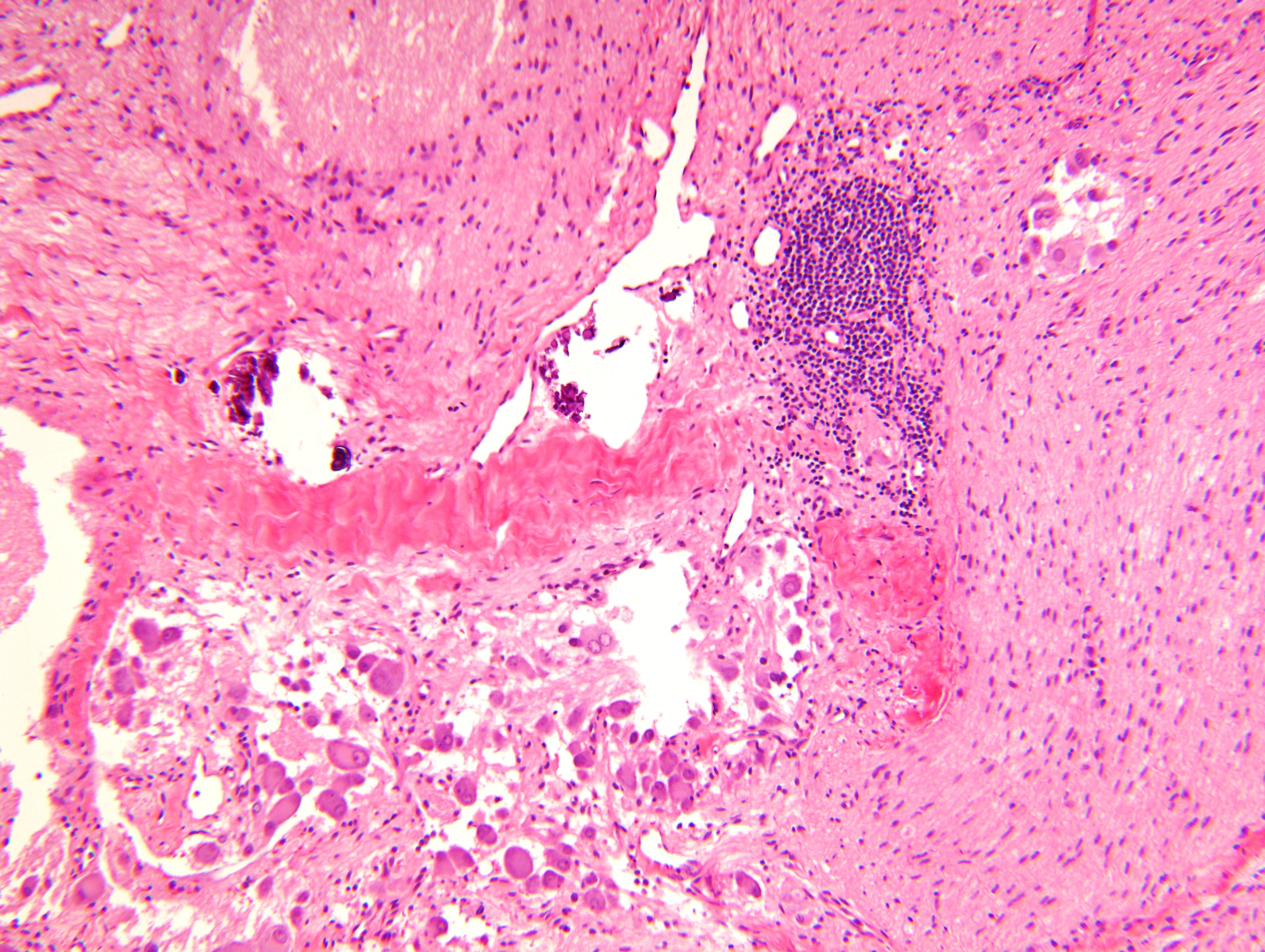
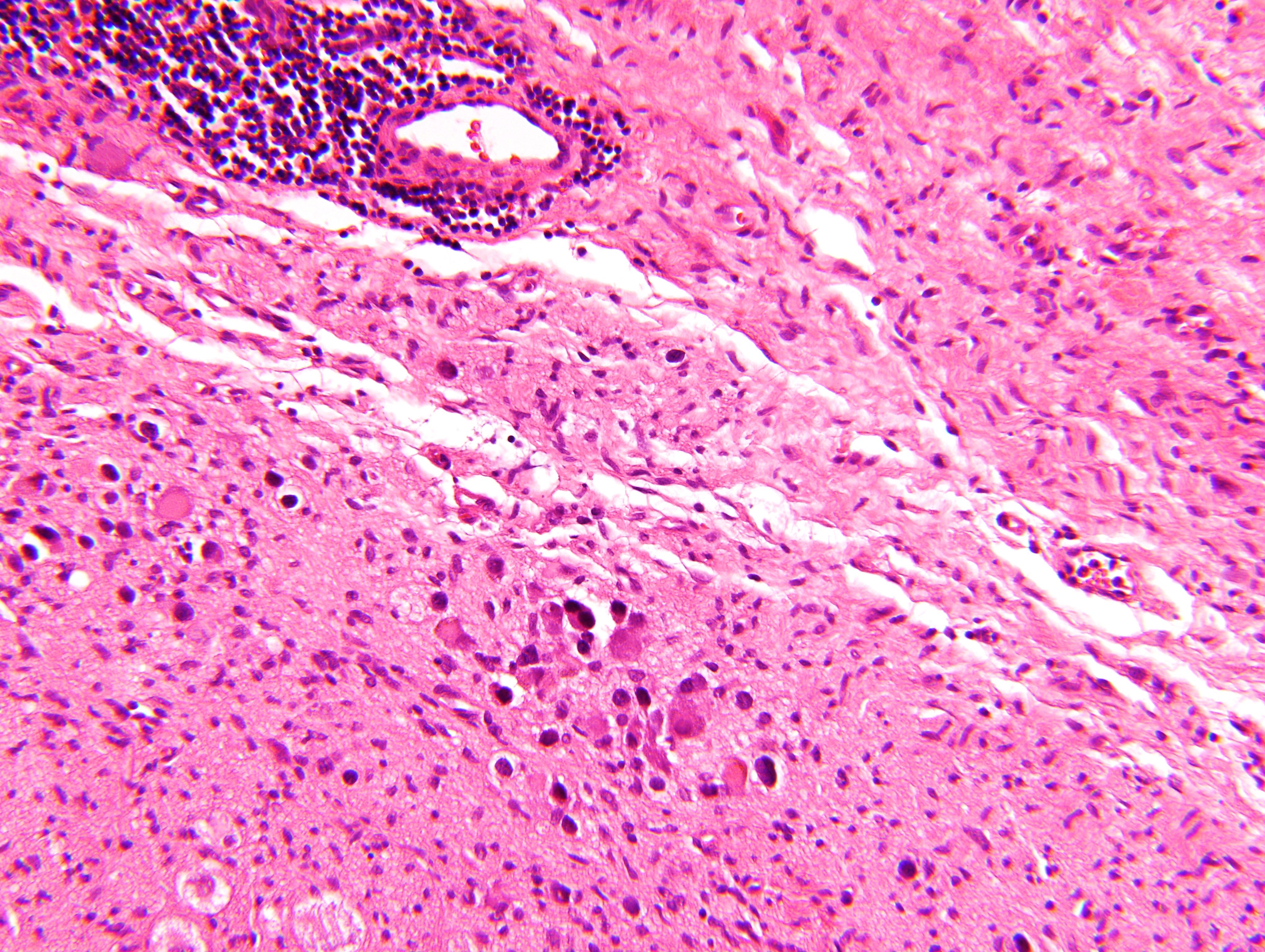
Lymphocyte aggregate
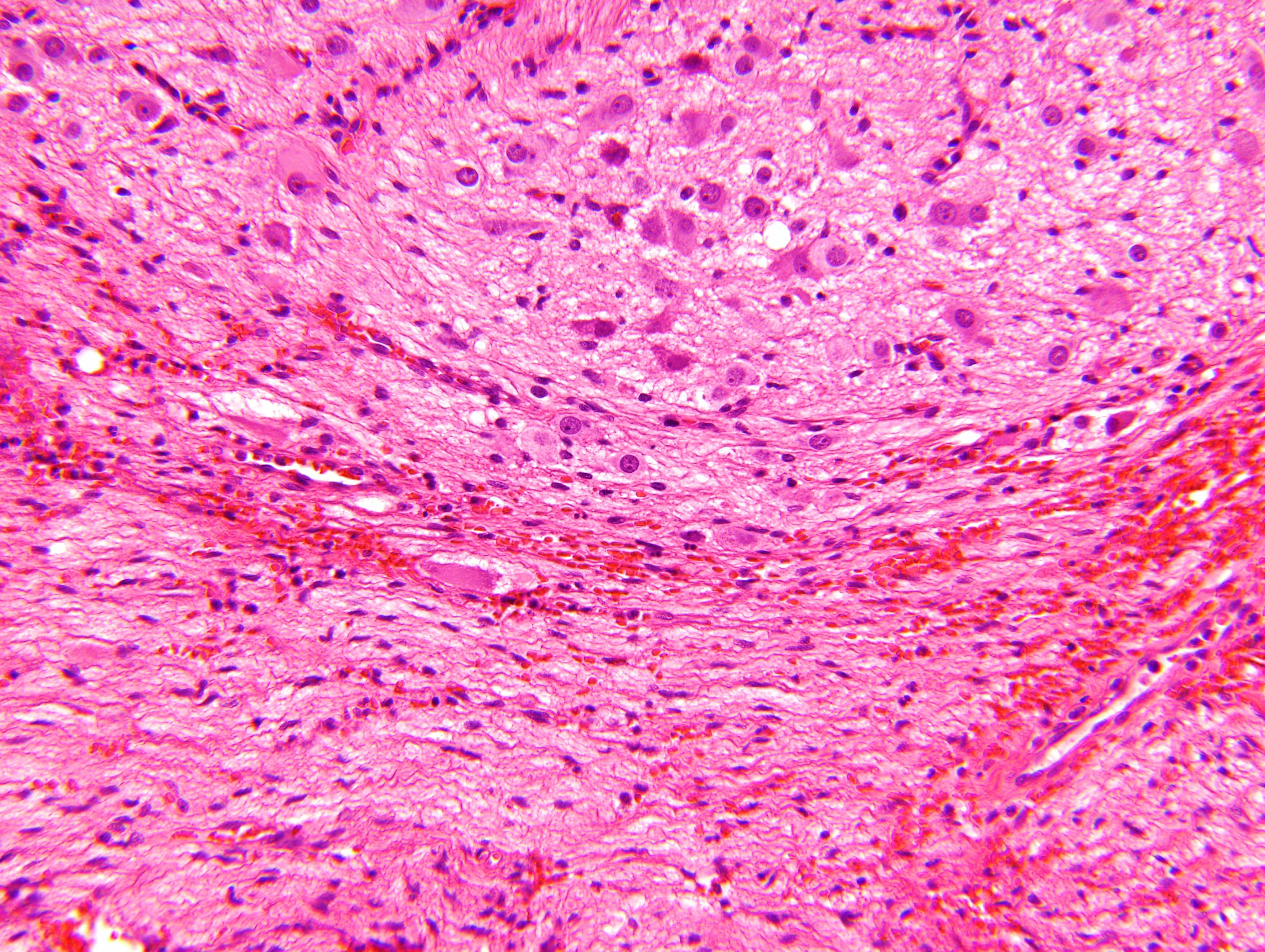
Area with Schwannian stroma
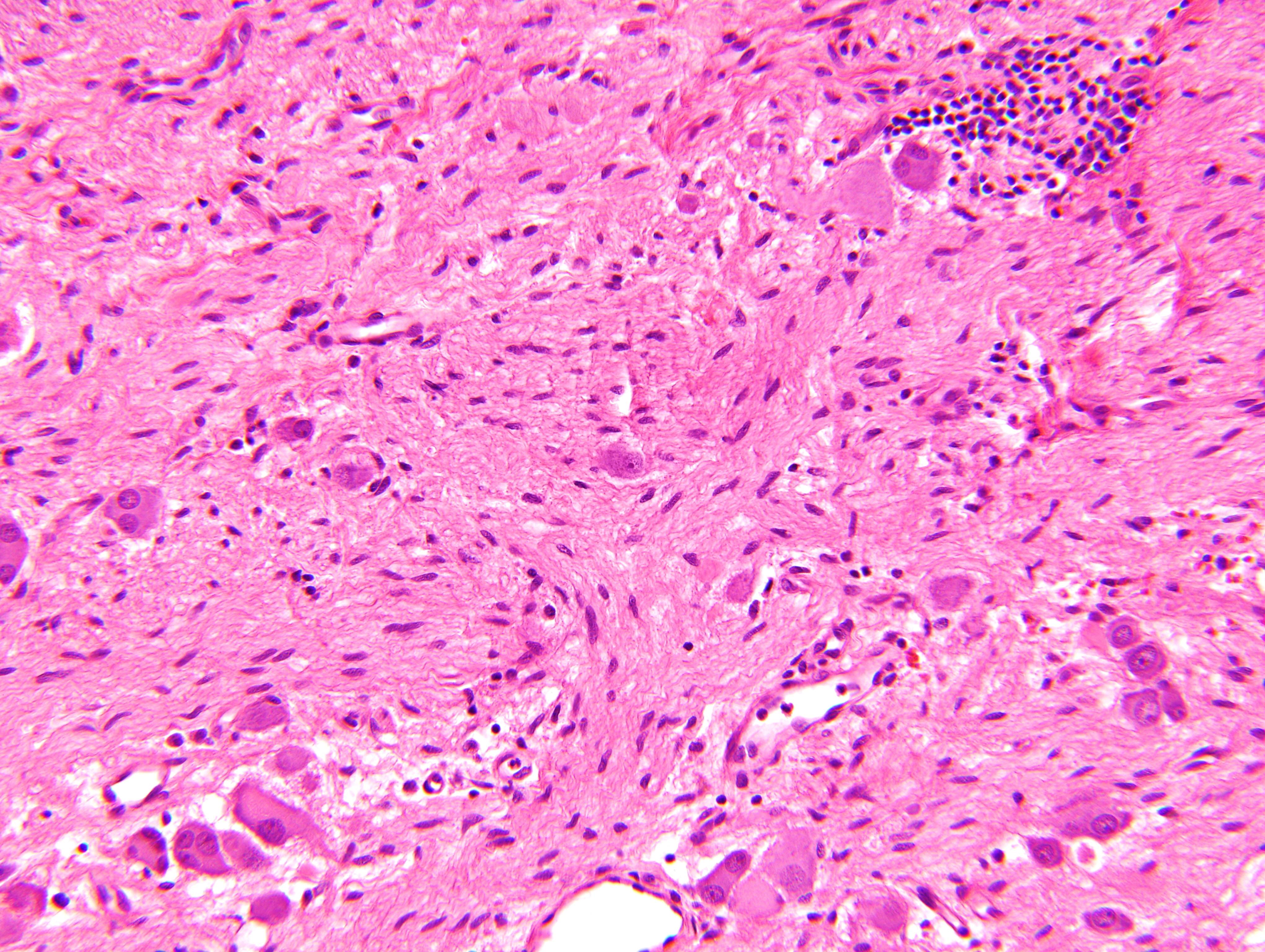
Maturing ganglion cells
Stroma rich, intermixed type
Nodular type
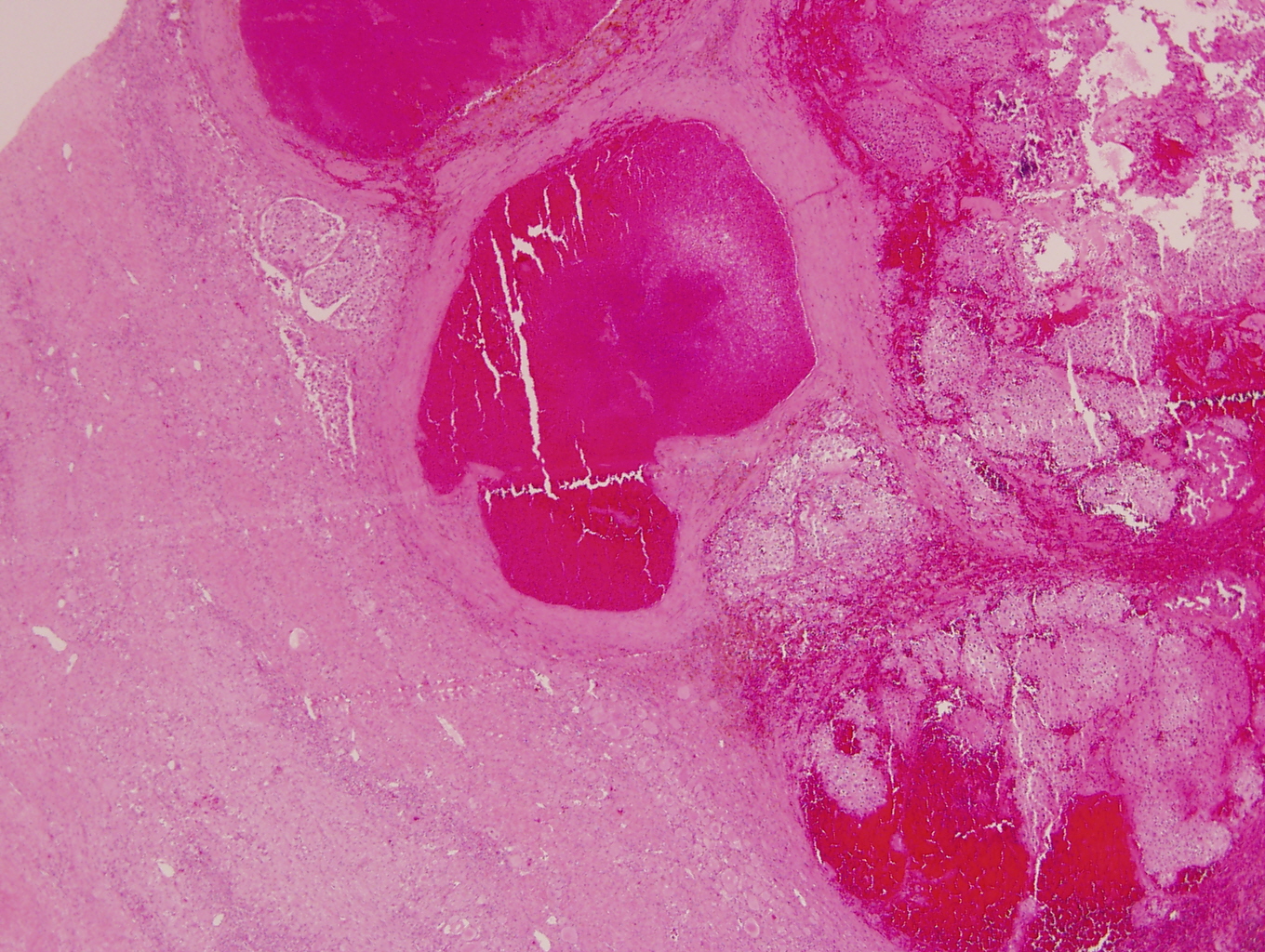
Stroma rich, nodular type
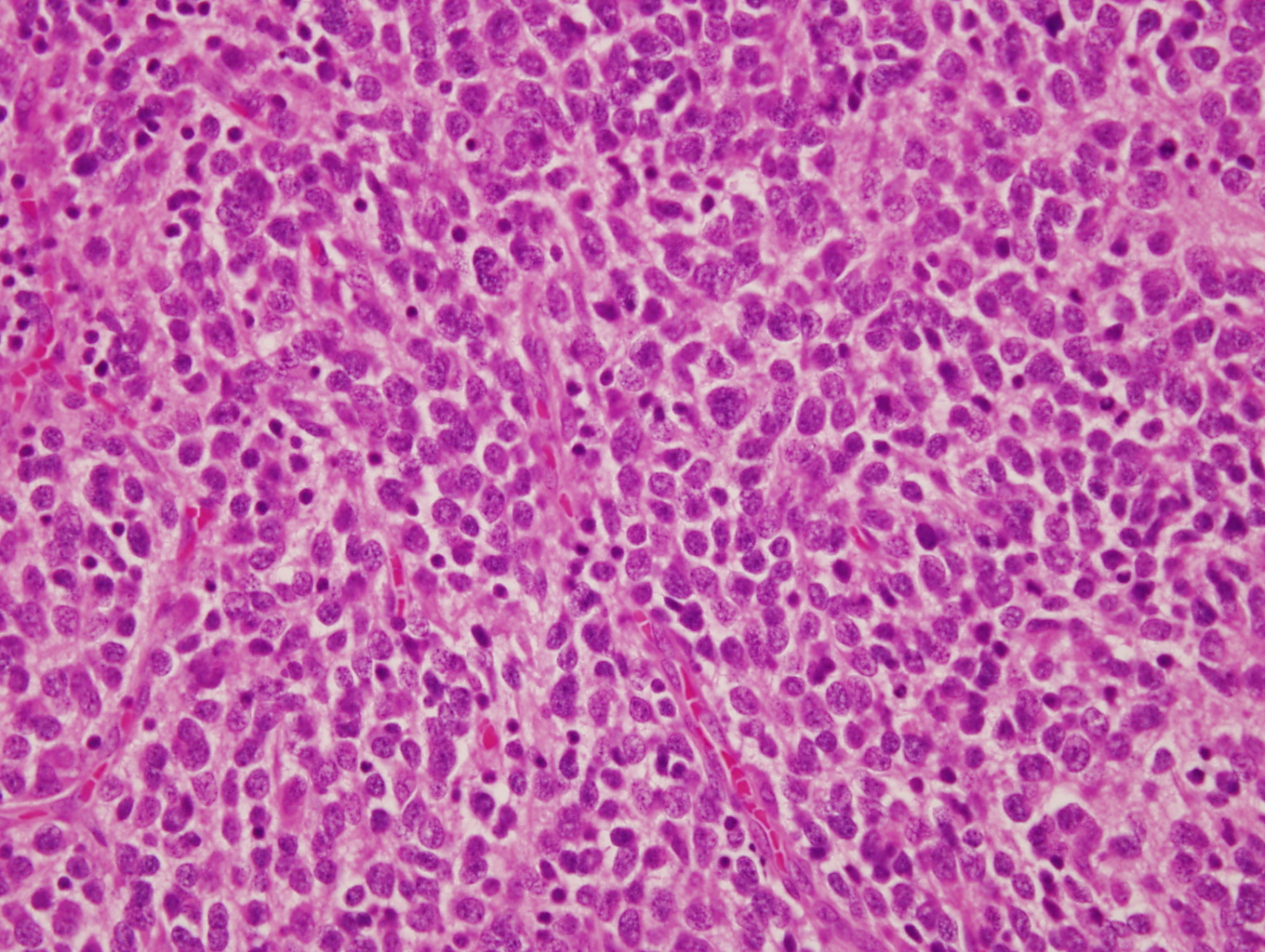
Neuroblast cell component
Homer Wright pseudorosettes

Vaguely formed Homer Wright pseudorosettes
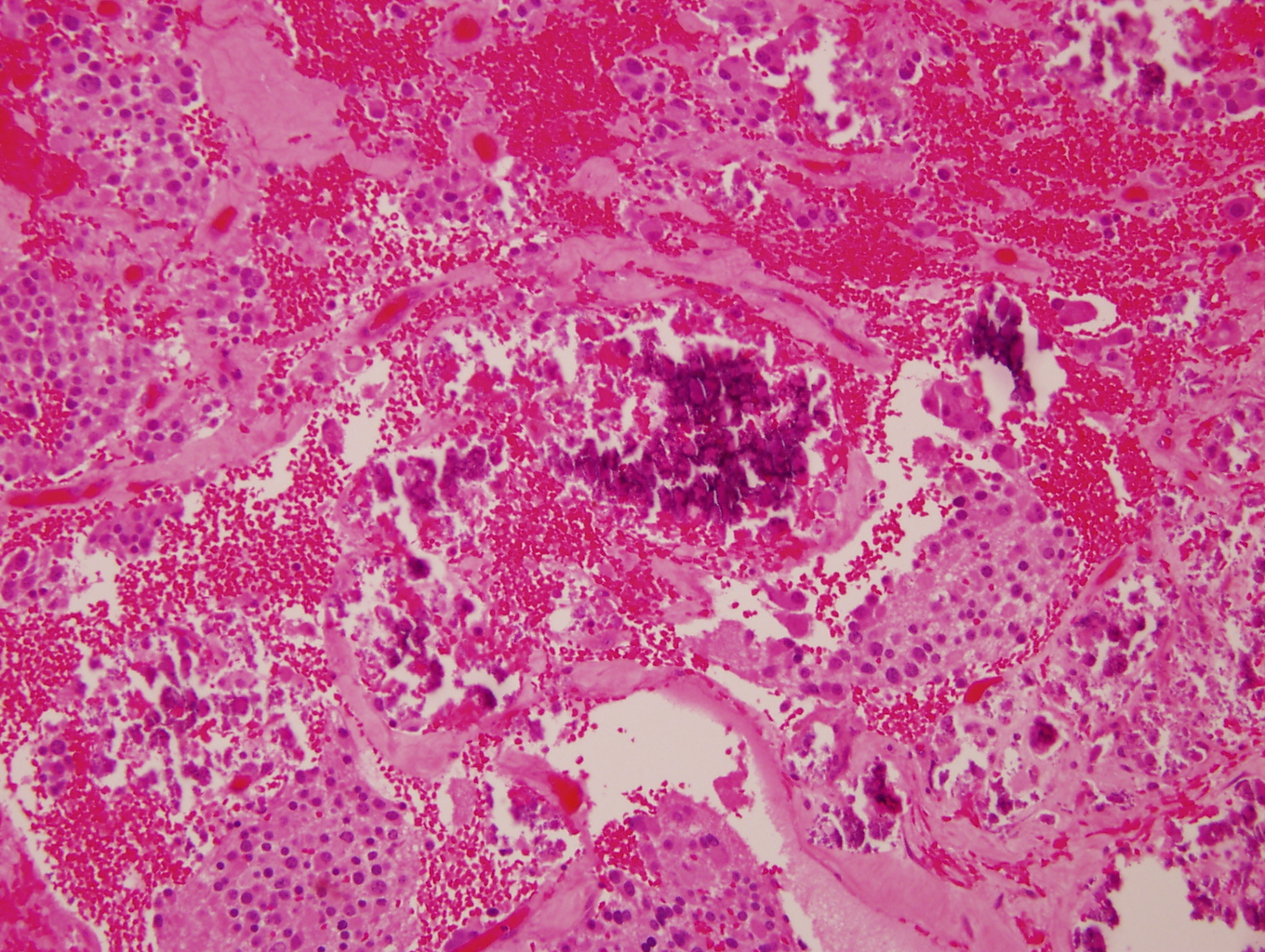
Hemorrhagic component
Cytology description
- Ganglion cells: larger cells, abundant cytoplasm, fine chromatin, prominent nucleoli
- Neuroblasts: uniform, small, blue cells with scant, eosinophilic, fibrillary cytoplasm; hyperchromatic to vesicular chromatin
- May form Homer Wright pseudorosettes
Cytology images
Contributed by Carmen Perrino, M.D. and Debra L. Zynger, M.D.
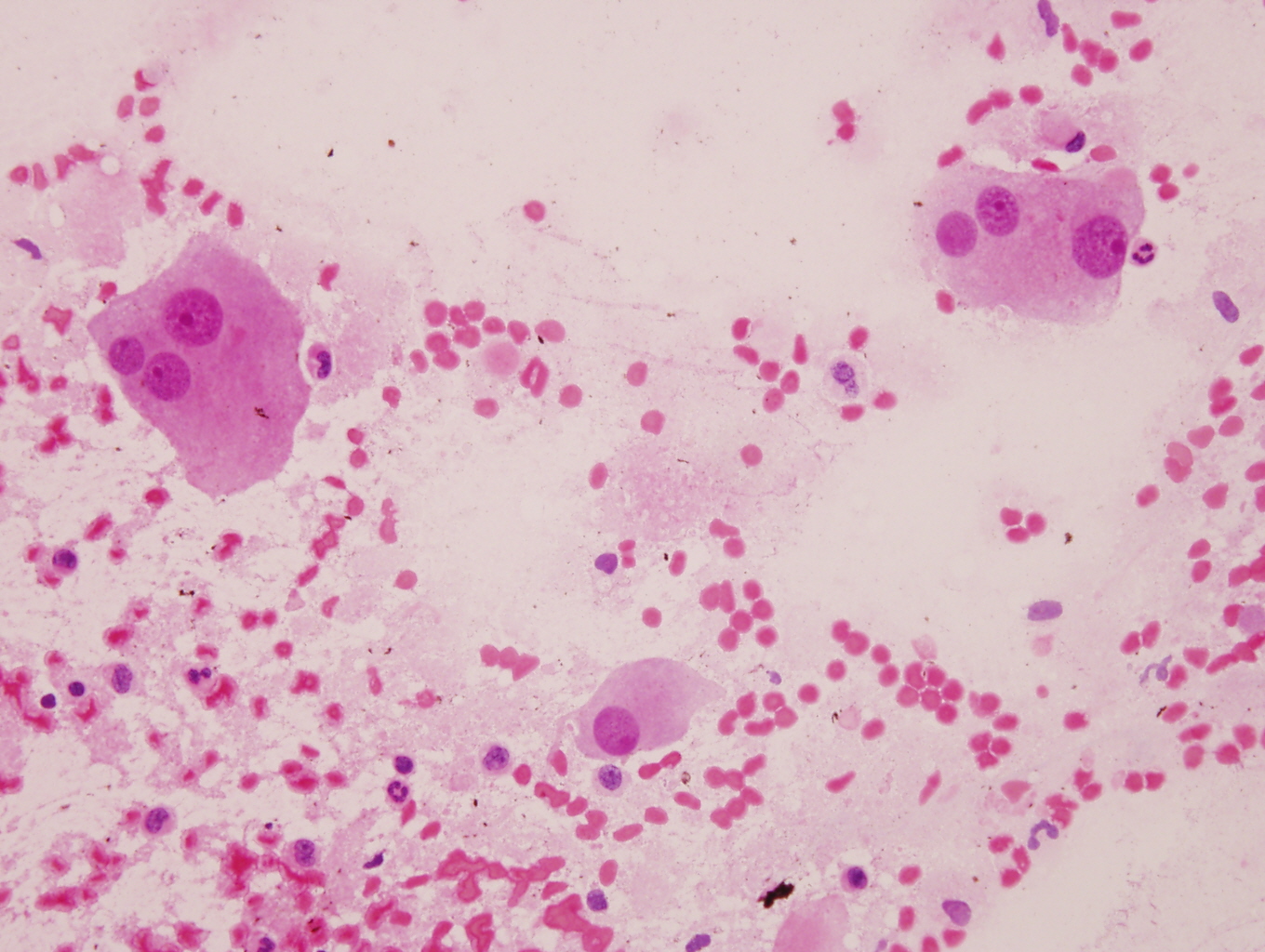
Numerous ganglion cells
Positive stains
- Neuroblasts:
- Neuron specific enolase (NSE), CD57 / Leu7, CD56, protein gene product 9.5 (PGP 9.5), synaptophysin, chromogranin, neurofilament protein, ALK1 (> 90%), PHOX2B (Am J Pathol 2012;180:1223, Am J Surg Pathol 2012;36:1141)
- Schwannian stroma:
- Ganglion cells:
Negative stains
Electron microscopy description
- Neuritic processes with neurotubules and neurofilaments, regular / uniform dense core granules measuring < 200 nm in diameter (Lack: Tumors of the Adrenal Glands and Extraadrenal Paraganglia, Volume 8, AFIP, Series 4)
Molecular / cytogenetics description
- Considered molecularly heterogeneous but much of genetic basis remains unexplained (Cancer 2003;98:2274)
- ALK gene mutations have been implicated in some cases of ganglioneuroblastoma (Am J Pathol 2012;180:1223)
- Ganglioneuroblastoma, stroma rich, nodular subtype, is considered a composite tumor consisting of separate clones (less aggressive stroma rich component; nodular component consisting of a favorable / unfavorable / both clones) (Cancer 2003;98:2274)
Molecular / cytogenetics images
Contributed by Leica Biosystems
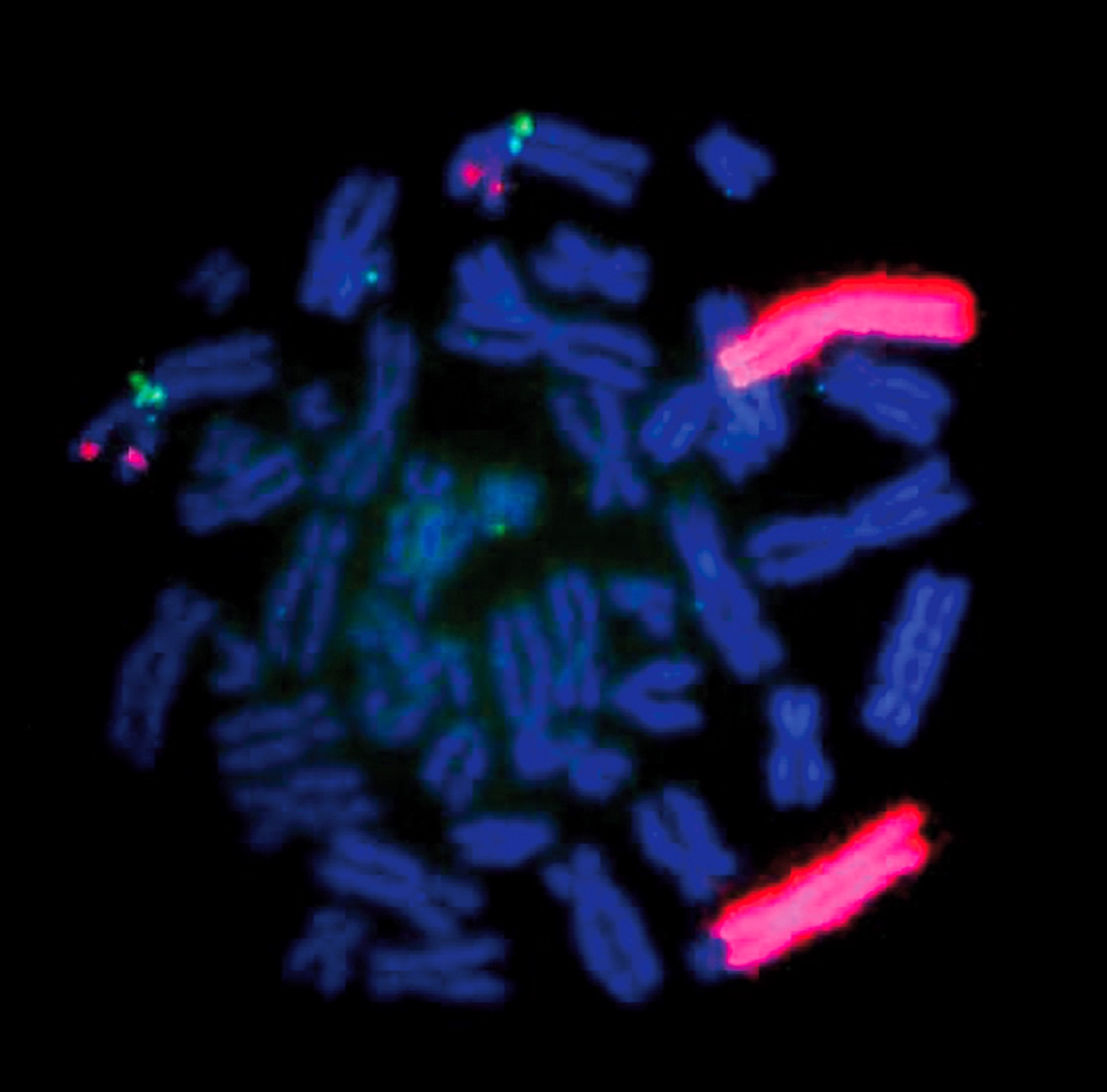
MYCN (2p24) / AFF3 (2q11)
