
Lymphoma & related disorders
Hodgkin lymphoma
CHL lymphocyte rich
Editorial Board Member: Julie Feldstein, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 19 October 2023
Last staff update: 19 October 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Lymphocyte rich classic Hodgkin lymphoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Bárcena C, de Leval L. CHL lymphocyte rich. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomanonBLRHL.html. Accessed April 26th, 2024.
Definition / general
- Subtype of classic Hodgkin lymphoma (CHL) with Hodgkin / Reed-Sternberg (HRS) cells in a nodular or less commonly diffuse background of small lymphocytes (Blood 2022;140:1229, Leukemia 2022;36:1720)
Essential features
- B cell lymphoma derived from germinal center B cells
- Scattered HRS cells in a nodular or diffuse background of small lymphocytes without eosinophils and neutrophils
- Immunophenotype of HRS cells: PAX5+ (dim), CD30+, CD15 variable, CD20 variable
ICD coding
Epidemiology
- Rare subtype of CHL that accounts for 5.8% of classic Hodgkin lymphoma (Cancer Med 2018;7:953)
- Most patients are adults (30 - 50 years)
- Male predominance (70%)
- EBV infection in 30 - 50% of cases; the virus is within the HRS cells and usually shows a type II latency pattern of infection
Sites
- Peripheral lymph nodes (most often cervical) are typically affected (Leuk Lymphoma 2019;60:3426)
- Mediastinal involvement (15%) and bulky disease are rare
Pathophysiology
- Pathophysiology is incompletely understood
- HRS cells derived from preapoptotic germinal center B cells with a disrupted B cell program (Leukemia 2021;35:968)
- HRS cells harbor monoclonal IGH rearrangements with somatic mutations of their Ig variable region genes and lack the capacity of Ig expression (Leukemia 2021;35:968)
- Genetic lesions that promote HRS cell proliferation, survival, immune evasion and interaction with their microenvironment, including alterations in NFκB and JAK / STAT signaling pathways (Leukemia 2021;35:968)
- EBV could play a crucial role by infecting HRS cells with crippled germinal center B cell receptor (BCR), rescuing them from apoptosis and thus inducing lymphomagenesis (Blood 2005;106:4339)
- EBV infection activates the NFκB pathway promoting survival and growth (Histopathology 2021;79:451)
Etiology
- Remains unknown
Clinical features
- Similar to those of nodular lymphocyte predominant Hodgkin lymphoma (WHO 5) / nodular lymphocyte predominant B cell lymphoma (ICC), except that relapses are less frequent in lymphocyte rich CHL (LRCHL) (J Clin Oncol 1999;17:776)
- B symptoms are rare
- Most patients are diagnosed at stage I / II (J Clin Oncol 2005;23:5739)
Diagnosis
- Histopathological analysis of an excisional lymph node biopsy or tissue biopsy supplemented with ancillary techniques (immunohistochemistry, EBER ISH)
Laboratory
- Nonspecific findings: anemia, leukocytosis, lymphocytopenia, elevated C reactive protein (N Engl J Med 1998;339:1506)
Prognostic factors
- Approximately 90 - 95% of patients with early stage CHL and 80 - 85% with advanced stage CHL are cured (Am J Hematol 2020;95:978)
- Prognosis is slightly better than other CHL subtypes and similar to nodular lymphocyte predominant Hodgkin lymphoma (NLPHL), unless for the relapses, that are more common in NLPHL
- Treatment is individualized according to defined risk groups based on following prognostic factors
- Ann Arbor stage (most important predictor of outcome) (J Clin Oncol 2014;32:3059)
- Bulky (mediastinal) disease
- Extranodal involvement
- B symptoms
- International Prognostic Score (N Engl J Med 1998;339:1506)
Case reports
- 35 year old woman with a 2 month history of progressive cough and intermittent fever (Ann Hematol 2014;93:1073)
- 35 year old man with a 4 month history of supraclavicular and cervical lymphadenopathies (J Clin Exp Hematop 2015;55:23)
Treatment
- Intensive polychemotherapy (ABVD or BEACOPP) with or without radiotherapy (Am J Hematol 2020;95:978)
- For refractory cases: stem cell transplant, brentuximab vedotin, checkpoint inhibitors (N Engl J Med 2018;378:331)
Gross description
- Involved lymph node is enlarged
- Vaguely nodular
- Fleshy appearance
- Reference: Leukemia 2022;36:1720
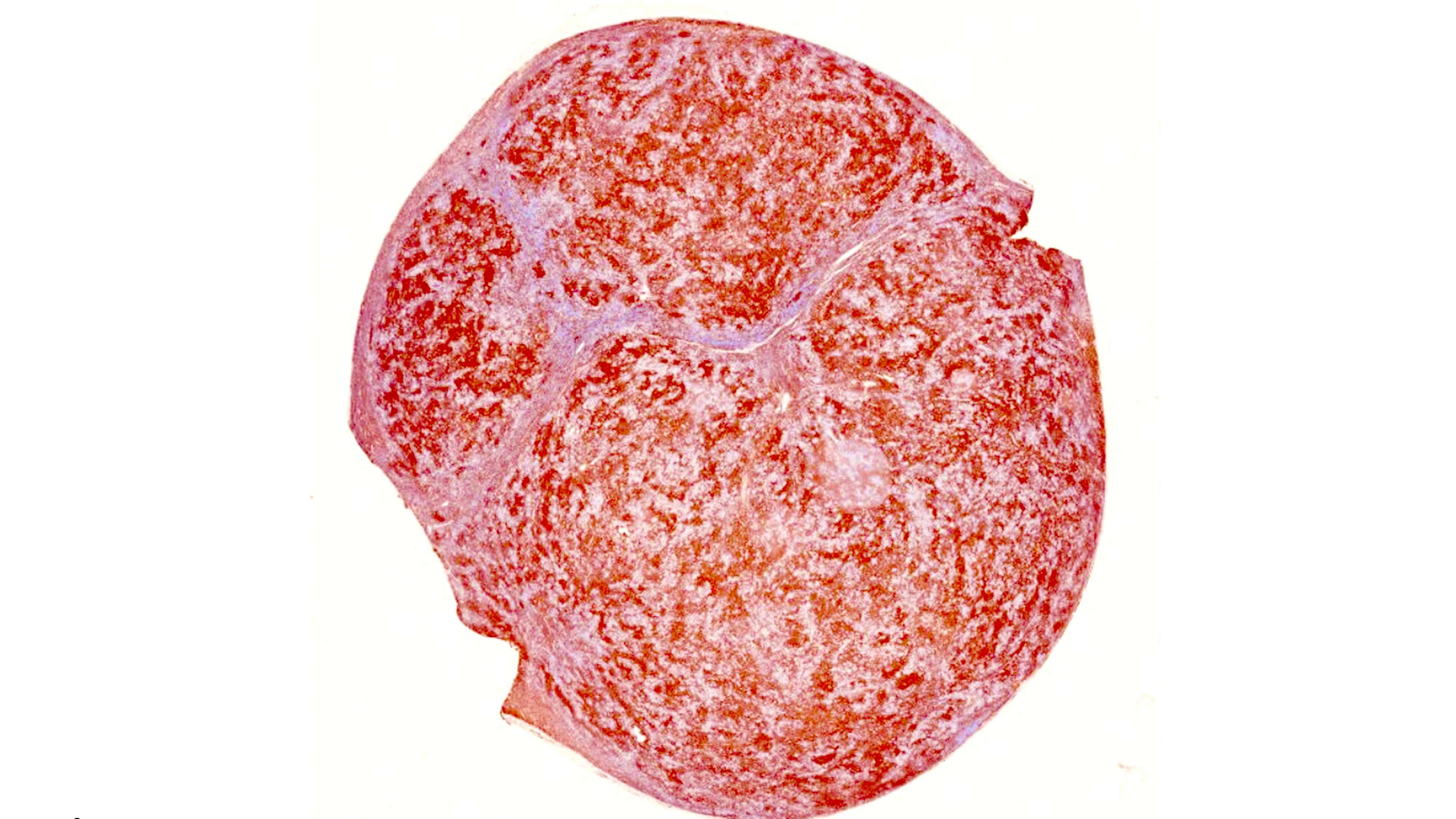
Gross images
Contributed by Laurence de Leval, M.D., Ph.D. and Carmen Bárcena, M.D.

Macroscopy
Microscopic (histologic) description
- 2 patterns of growth: nodular or less often, diffuse proliferation with numerous reactive small lymphocytes and scattered HRS cells (Leukemia 2022;36:1720)
- Neutrophils and eosinophils are absent from the nodules
- In lymphocyte rich classic Hodgkin lymphoma (LRCHL) nodular cases
- Nodules are composed of small lymphocytes and may contain eccentrically located germinal centers (small or regressed)
- Nodules contain dense meshwork of follicular dendritic cells (CD21+)
- HRS cells are within the nodules but outside of the germinal centers
- Some HRS cells resemble lymphocyte predominant cells (LP cells) or lacunar cells
- In LRCHL diffuse cases
- Small lymphocytes of the background can be intermingled with histiocytes with or without epithelioid morphology
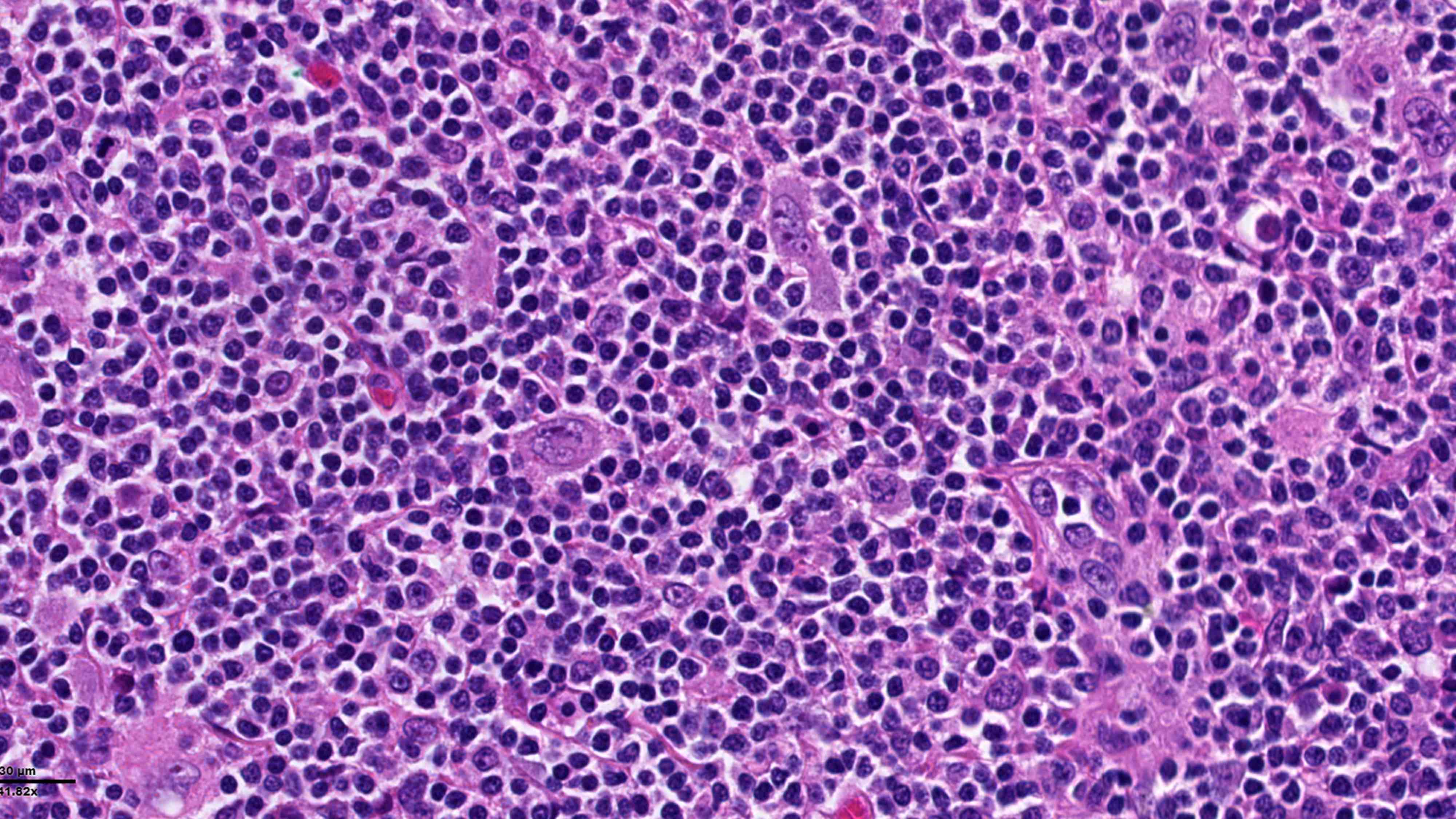
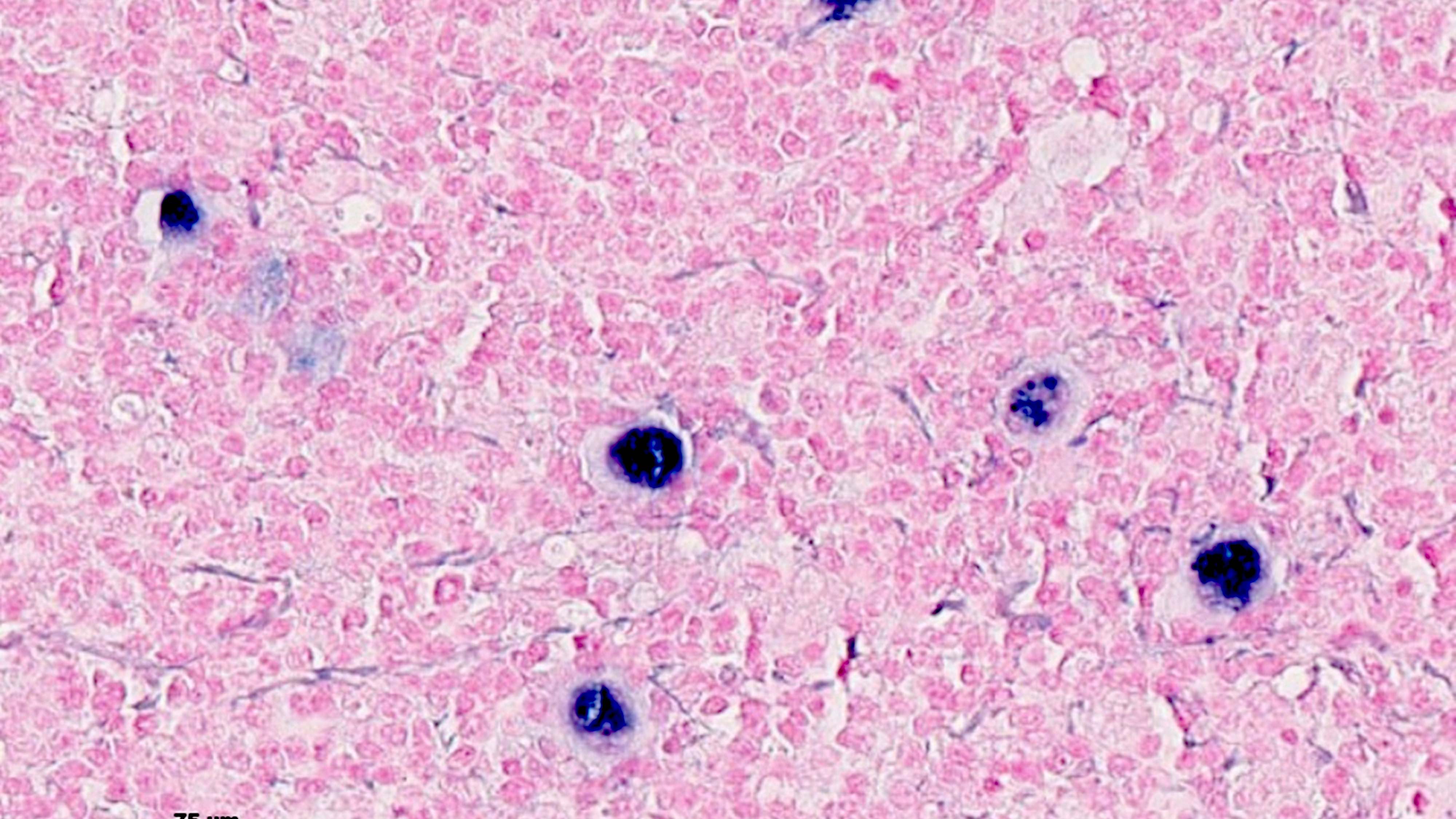
Microscopic (histologic) images
Contributed by Laurence de Leval, M.D., Ph.D. and Carmen Bárcena, M.D.

Nodular pattern
CD20
HRS cells
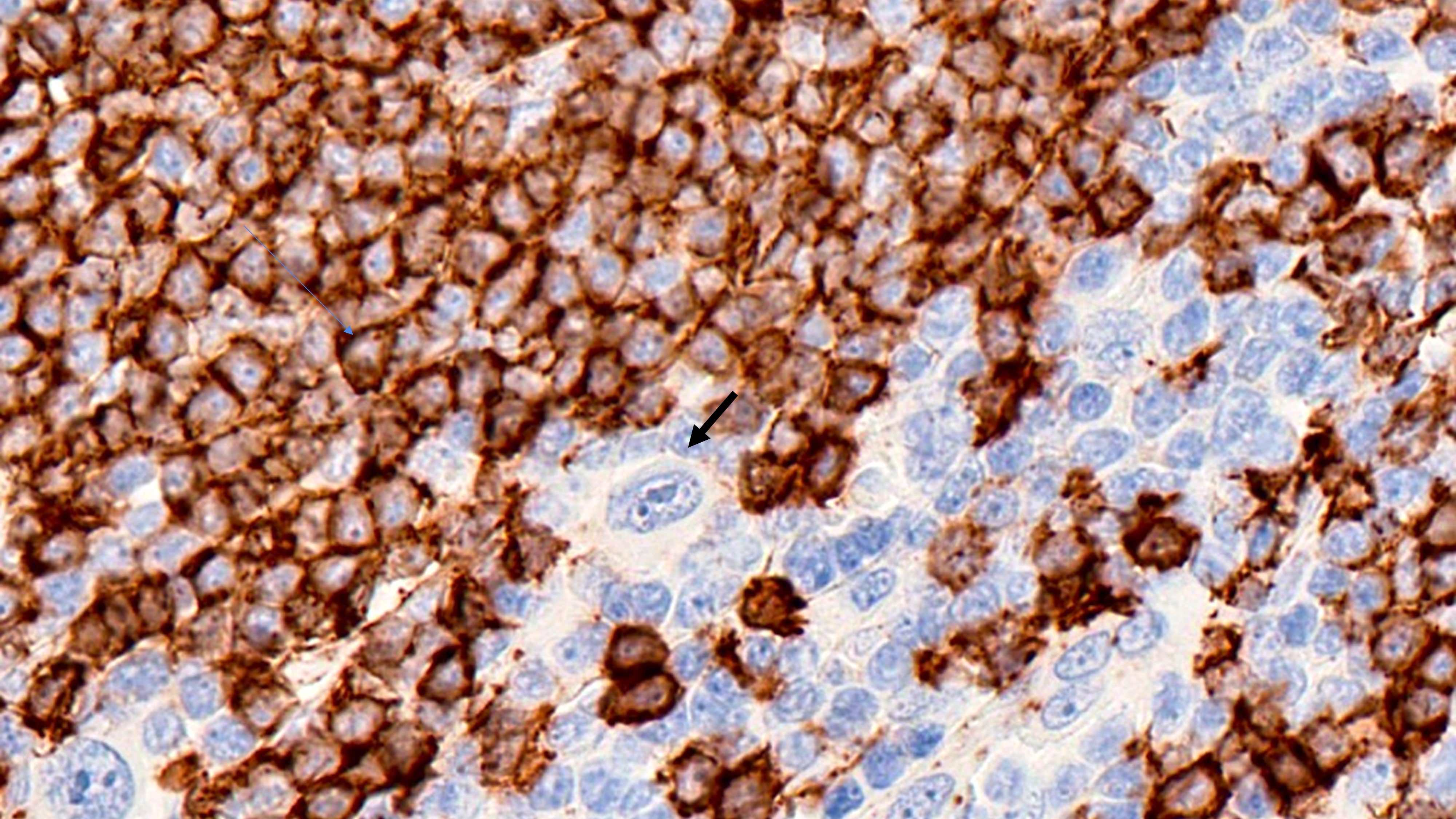
CD20

PAX5

OCT2

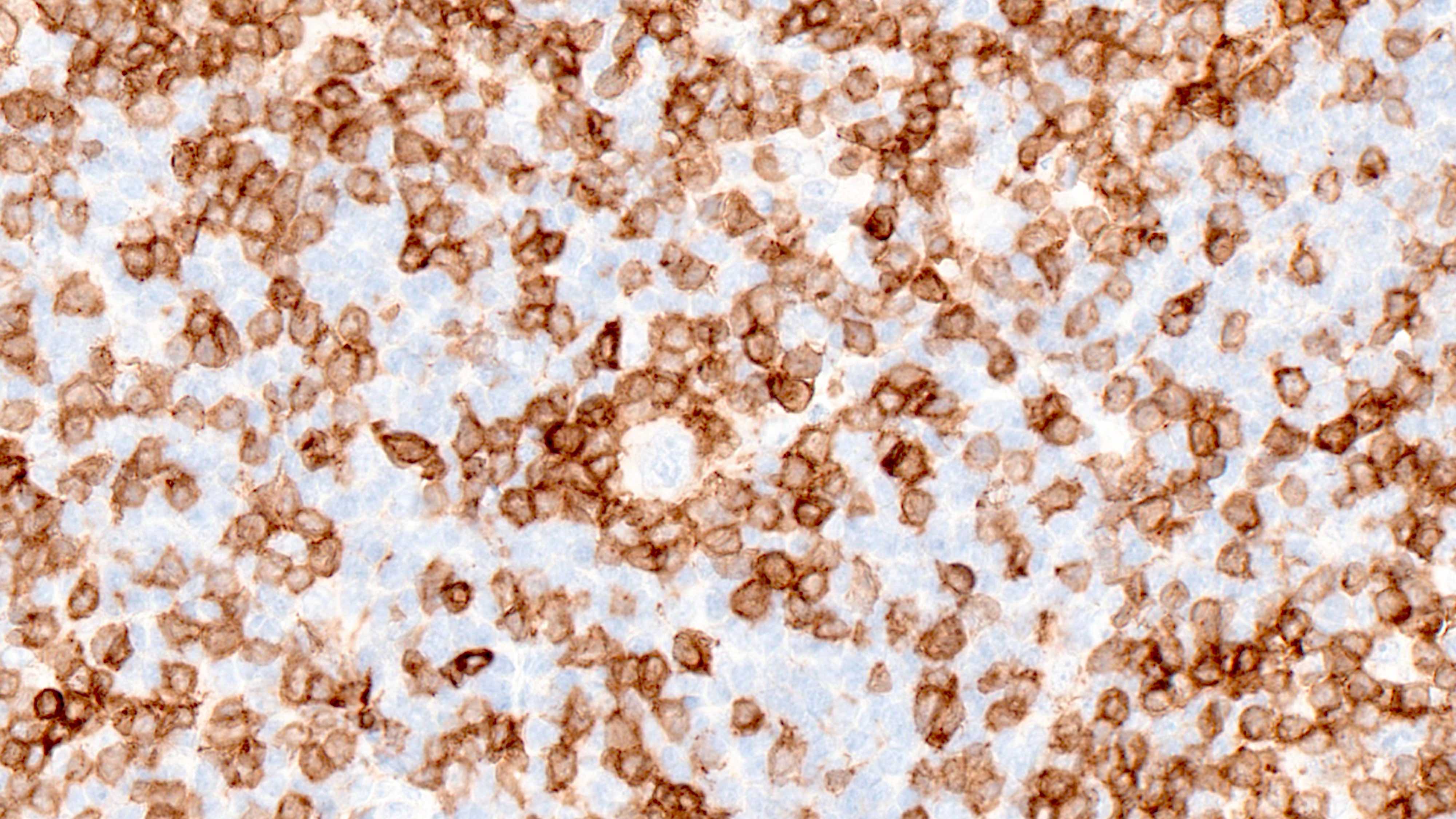
CD30

CD15

MUM1
CD3

PD-1
EBER in situ hybridization
Positive stains
- Hodgkin Reed-Sternberg (HRS) cells
- PAX5 (dim), CD30 (strong and uniform), CD15 variable (75% of cases), MUM1 (Ann Diagn Pathol 2019;39:105)
- OCT2 (56%) and BOB1 (62%) are more frequently expressed than in other CHL subtypes (Mod Pathol 2009;22:1006)
- STAT6YE361 (nuclear or nuclear and cytoplasmic) (Mod Pathol 2020;33:834)
- GATA3 (67%) (Appl Immunohistochem Mol Morphol 2019;27:180, Blood 2010;116:4202, Am J Pathol 2005;166:127, J Clin Pathol 2007;60:1092)
- PDL1, PDL2 (Histopathology 2018;72:1156, Blood 2018;131:68)
- Fascin (Appl Immunohistochem Mol Morphol 2010;18:16)
- EBV positive cases: EBV LMP1 variable, EBER
- Immunophenotype of the small lymphocytes in the background
- Background is composed of both B and T lymphocytes
- B cells are most prominent in LRCHL compared to other CHL subtypes
- B cells are IgM+, IgD+, corresponding to expanded mantle zones
- CD4+ T cells dominate the CHL microenvironment (Cytometry B Clin Cytom 2008;74:1, Blood 2004;103:1755, Lab Invest 2008;88:482)
- In 50% of LRCHL cases, HRS are surrounded by rosettes of T follicular helper cells (CD4+, PD-1+, CD57 variable) (Mod Pathol 2009;22:1006, Proc Natl Acad Sci U S A 2021;118:e2105822118)
Negative stains
- Hodgkin Reed-Sternberg (HRS) cells
- Variable: CD20 (weak), CD79a (Leukemia 2022;36:1720)
- CD20 (31%) and BCL6 (36%) are more frequently expressed than in other CHL subtypes (Mod Pathol 2009;22:1006)
- BCL2 (Leukemia 2022;36:1720)
- CD45, ALK, EMA, CD23 (Curr Hematol Malig Rep 2011;6:157, Ann Diagn Pathol 2019;40:72)
- Immunoglobulins, light and heavy chains, are negative (Leukemia 2022;36:1720)
Molecular / cytogenetics description
- Aneuploidy is seen in nearly all cases (Blood 1995;86:1464, Cancer Res 2006;66:10332, Cancers (Basel) 2018;10:91)
- High constitutive activity of the NFκB pathway is the hallmark of HRS cells which is essential for HRS cell survival (Semin Cancer Biol 2016;39:32)
- Mutations in members of the JAK / STAT signaling pathway, main mediator of cytokine signaling (Nat Genet 2014;46:329)
- Mutations in ITPKB, PI3K / AKT and MAP / ERK pathways (Leukemia 2020;34:151)
- Lesions in genes involved in immune evasion of HRS: PDL1, PDL2, B2M, CIITA, CD58 (Blood 2010;116:3268, J Clin Oncol 2016;34:2690)
- Mutations in additional genes: ARID1A, TNFRS14, XPO1 (Leukemia 2021;35:968)
Sample pathology report
- Lymph node, left neck, excision:
- Lymphocyte rich classic Hodgkin lymphoma (see comment)
- Comment: H&E stained sections display a lymph node with architectural effacement by a nodular proliferation of abundant small lymphocytes and scattered large atypical lymphoid cells. The neoplastic cells have monolobated / bilobated / multilobated nuclei, vesicular chromatin, prominent nucleoli and amphophilic cytoplasm, consistent with HRS cells.
- Immunophenotypically, the large atypical cells are positive for PAX5 (weak), OCT2, CD30 (strong), CD15, MUM1 and GATA3 and negative for CD20 and CD45.
- TFH markers reveal T cell rosettes around HRS cells.
Differential diagnosis
- Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) / nodular lymphocyte predominant B cell lymphoma (NLPBCL) (Blood 2000;96:1889):
- T cell / histiocytic rich large B cell lymphoma (THRLBCL):
- Composed of a background rich in small lymphocytes and histiocytes with scattered large neoplastic B cells CD20+, BCL6+, CD30-, CD15-, EBER-
- Eosinophils, plasma cells and neutrophils are uncommon
- These characteristics argue against a diagnosis of CHL (Leukemia 2022;36:1720)
- B symptoms are more common
- Aggressive clinical course
- Small lymphocytic lymphoma / chronic lymphocytic leukemia:
- Follicular lymphoma:
- Nodal TFH T cell lymphoma:
- Scattered large B cells with an HRS-like morphology may be present
- HRS-like cells have a preserved B cell program (CD79a+, PAX5+, OCT2+, BOB1+, CD20 variable)
- Some cases harbor B cells with a HRS phenotype (CD30+, CD15 variable, EBV variable) in a background of TFH atypical cells
- Monoclonal T cell receptor gene rearrangement and NGS showing mutation of the hotspot RHOA (G17V) and IDH2 (R172) favor the diagnosis of nodal TFH (Histopathology 2014;64:171, Br J Haematol 2008;141:124)
Board review style question #1
What is the characteristic immunophenotype of the large atypical cells shown in the image above?
- CD20+, CD30-, CD15-, BCL6+, IgD-
- CD20+, PAX5+, CD23+, CD30+
- CD45+, OCT2+, CD20+, CD30 -, CD15-, IgD+
- CD45-, PAX5+, CD30+, CD15+
- PAX5-, CD4+, CD30+, ALK-
Board review style answer #1
D. CD45-, PAX5+, CD30+, CD15+. This is the characteristic immunophenotype of Hodgkin / Reed-Sternberg cells. Answer A is incorrect because the large atypical cells of T cell / histiocytic rich large B cell lymphoma express this immunophenotype. Answer B is incorrect because this immunophenotype is characteristic of primary mediastinal B cell lymphoma. Answer C is incorrect because the LP cells in nodular lymphocyte Hodgkin lymphoma (WHO 5) / nodular lymphocyte predominant B cell lymphoma typically express this immunophenotype (ICC 2022). Answer E is incorrect because this immunophenotype is not specific. T cells could show this immunophenotype.
Comment Here
Reference: CHL lymphocyte rich
Comment Here
Reference: CHL lymphocyte rich
Board review style question #2
What is the typical composition of the background of lymphocyte rich classic Hodgkin lymphoma (LRCHL) with nodular pattern?
- Small atypical B cells: CD20+, BCL2+, BCL6+, CD10+
- Small B cells: CD20+, CD5+, CD23+, LEF1+
- Small B cells IgD+ admixed with CD4+ PD-1+ T cells
- Small T cells, eosinophils, plasma cells and neutrophils
Board review style answer #2
C. Small B cells IgD+ admixed with CD4+ PD-1+ T cells. The background is typically composed of B cells corresponding to expanded mantle zones (IgD+) admixed with CD4+, PD-1+ T cells, rosetting Hodgkin / Reed-Sternberg (HRS) cells. Answer B is incorrect because this is the characteristic composition of small lymphocytic lymphoma. Answer D is incorrect because this background is not specific but in the present of HRS cells it is diagnostic of mixed cellularity classic Hodgkin lymphoma. Answer A is incorrect because this is the characteristic composition of follicular lymphoma.
Comment Here
Reference: CHL lymphocyte rich
Comment Here
Reference: CHL lymphocyte rich
