
Lymphoma & related disorders
Mature T/NK cell disorders
Aggressive NK/T cell disorders
Hepatosplenic T cell lymphoma
Authors: Mario L. Marques-Piubelli, M.D., Maria C. Ferrufino-Schmidt, M.D., Roberto N. Miranda, M.D.
Editorial Board Member: Anamarija M. Perry, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 2 May 2022
Last staff update: 4 October 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Hepatosplenic T cell lymphoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Pathophysiology | Etiology | Clinical features | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Flow cytometry description | Flow cytometry images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Marques-Piubelli ML, Ferrufino-Schmidt MC, Miranda RN. Hepatosplenic T cell lymphoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomanonBhepatosplenic.html. Accessed May 6th, 2024.
Definition / general
- Rare, aggressive extranodal neoplasm that originates from nonactivated cytotoxic T cells; it usually expresses the T cell receptor (TCR) γδ (gamma delta) (Ann Diagn Pathol 2017;26:16, Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Cancer Treat Res 2019;176:185)
- First described in 1981 by Marshall Kadin as erythrophagocytic Tγ lymphoma; recognized as a distinct entity in 1994 (N Engl J Med 1981;304:648)
Essential features
- Rare, aggressive extranodal neoplasm that originates from cytotoxic T cells; it usually expresses the T cell receptor (TCR) γδ (gamma delta) (Am J Surg Pathol 2017;41:82)
- Hepatomegaly and splenomegaly are the most common clinical manifestations (Ann Diagn Pathol 2017;26:16)
- Liver and bone marrow: sinusoidal infiltration (Histopathology 2014;64:171)
- Median bone marrow tumor burden ~30% (5 - 80%) (Am J Surg Pathol 2016;40:676)
- Spleen
- Diffuse involvement; expansion of the red pulp cords and sinusoids, with atrophy or absence of white pulp (Hum Pathol 2018;74:5)
- Cytology: variable
- Usually monotonous, small to intermediate size cells with pale agranular cytoplasm, round / oval nuclei, moderately condensed chromatin and inconspicuous nucleoli (Blood 2003;102:4261)
Terminology
- Obsolete term: erythrophagocytic Tγ lymphoma
ICD coding
- ICD-O: 9716/3 - hepatosplenic T cell lymphoma
Epidemiology
- < 1% of all non-Hodgkin lymphomas and 1 - 2% of all T / NK cell lymphomas (Hum Pathol 2018;74:5, Semin Diagn Pathol 2020;37:47, Clin Lymphoma Myeloma Leuk 2021;21:106)
- Most common T cell lymphoma that affects the spleen (Semin Diagn Pathol 2020;37:47)
- M > F (Am J Surg Pathol 2017;41:82, Blood 2020;136:2018, Int J Gen Med 2021;14:8399)
- More common in young adult men, median age ~35 years (range: 4 - 82 years) (Ann Diagn Pathol 2017;26:16, Hum Pathol 2016;50:109, Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Blood 2003;102:4261)
- Increased incidence in the United States in the last 2 decades (Am J Hematol 2017;92:E99)
Pathophysiology
- Neoplastic clonal proliferation of γδ T cells induced by the upregulation of the JAK / STAT (STAT3 and STAT5B) and PI3K signaling pathways or mutations of chromatin modifiers (SETD2, INO80 and ARID1B) (Hum Pathol 2018;74:5, Haematologica 2019;104:e104, Blood 2020;136:2018)
Etiology
- Unknown in 80% of cases
- Up to 20% of cases arise in a context of chronic immunosuppression (Hum Pathol 2018;74:5, Blood 2020;136:2018, Curr Opin Oncol 2021;33:406)
- Posttransplantation (kidney or liver) (Am J Clin Pathol 2000;113:487, Cancer Treat Res 2019;176:185)
- Patients with immunodysregulatory disorders (inflammatory bowel disease, rheumatoid arthritis) that are using immunosuppressive agents (mercaptopurine, azathioprine, infliximab) (Ann Diagn Pathol 2017;26:16, Am J Surg Pathol 2016;40:676, Cancer Treat Res 2019;176:185, Blood 2020;136:2018)
- TNFα inhibitors in Crohn's disease: fourfold increased risk of lymphomas (B cell lymphomas and hepatosplenic T cell lymphoma) (Am J Gastroenterol 2013;108:99)
- Risk factors for hepatosplenic T cell lymphoma (HSTCL) in patients with inflammatory bowel disease: male sex and long term thiopurine therapy (≥ 2 years)
- Genetic predisposition and chronic antigenic stimulation
Clinical features
- Hepatomegaly and splenomegaly are the most common clinical manifestations (Ann Diagn Pathol 2017;26:16, Am J Surg Pathol 2017;41:82, Clin Lymphoma Myeloma Leuk 2021;21:106)
- 70 - 80% of patients
- Massive splenomegaly is found in most patients, defined as ≥ 6 cm below costal margin, or ≥ 20 cm in greatest dimension, or splenectomy > 1,000 g
- Abdominal discomfort
- B symptoms (Am J Surg Pathol 2016;40:676)
- Lymphadenopathy is uncommon (< 25%); when present, splenic peripheral lymph nodes are most commonly involved (Histopathology 2014;64:171, Blood 2020;136:2018, Semin Diagn Pathol 2020;37:47)
- Peripheral blood involvement at initial presentation is uncommon
- Cytopenia or pancytopenia (Blood 2003;102:4261, Cancer Treat Res 2019;176:185, Blood 2020;136:2018):
- Moderate anemia, thrombocytopenia and neutropenia
- Hypersplenism, bone marrow infiltration or immune related
- Moderate anemia, thrombocytopenia and neutropenia
- Lymphocytosis in ~10% of the cases
- Cytopenia or pancytopenia (Blood 2003;102:4261, Cancer Treat Res 2019;176:185, Blood 2020;136:2018):
- Elevated levels of lactate dehydrogenase (LDH), β2 microglobulin and bilirubin (Hum Pathol 2018;74:5)
- Bone marrow (BM) is usually involved at initial presentation (Hum Pathol 2016;50:109)
- Cutaneous involvement is rare
Radiology description
- CT or MRI (Blood 2020;136:2018):
- Homogeneous hepatosplenomegaly
- Fluorodeoxyglucose (FDG) PET / CT (Blood 2020;136:2018):
- Diffuse FDG uptake in affected areas
- Usually liver, spleen and bone marrow
- Diffuse FDG uptake in affected areas
Prognostic factors
- Poor prognosis, with relapse in most cases (Am J Surg Pathol 2016;40:676)
- Median overall survival (OS) is 12 months (range: 3 - 34 months) (Hum Pathol 2018;74:5, Hum Pathol 2016;50:109, Int J Gen Med 2021;14:8399)
- 3 year overall survival: 37.6%
- 5 year overall survival: 31.6%
- Median progression free survival (PFS): 9.5 months 95% (CI, 1.8 - 16.3) (Clin Lymphoma Myeloma Leuk 2021;21:106)
- Prognostic factors correlated with worse outcomes:
- Serum bilirubin level > 1.5 mg/dl
- Expression of TCRαβ
- Trisomy 8
Case reports
- 20 year old man hepatosplenic T cell lymphoma αβ subtype presenting with Coombs negative hemolytic anemia (Clin Med Insights Oncol 2015;9:123)
- 47 year old man with Crohn's disease on thiopurine monotherapy (World J Gastroenterol 2016;22:10465)
- 53 year old woman with coexisting hairy cell leukemia and hepatosplenic T cell lymphoma (Diagn Pathol 2014;9:58)
- 56 year old woman with hemophagocytic lymphohistiocytosis associated with hepatosplenic T cell lymphoma (Autops Case Rep 2014;4:19)
- 59 year old man with hepatosplenic αβ T cell lymphoma masquerading as cirrhosis (J Gastrointest Oncol 2013;4:131)
- 59 year old man with hepatosplenic T cell lymphoma successfully treated with PD-1 inhibitor, chidamide and chemotherapy (J Dig Dis 2022;23:50)
Treatment
- No standard therapeutic guideline
- Cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP), or CHOP-like, hyper CVAD (cyclophosphamide, vincristine sulfate, adriamycin and dexamethasone) or hyper CVAD-like; or non CHOP induction regimen (2' deoxycoformycin) (Ann Diagn Pathol 2017;26:16, Am J Surg Pathol 2016;40:676)
- Consolidative stem cell transplant (SCT) for eligible patients (Haematologica 2005;90:ECR14, Clin Lymphoma Myeloma Leuk 2013;13:8, Cancer Treat Res 2019;176:185, Curr Opin Oncol 2021;33:406)
- Potential target therapy: CD52, JAK1 / 2, STAT3, STAT5B and PI3KCD (Hum Pathol 2018;74:5, Cancer Treat Res 2019;176:185)
Gross description
- Diffuse and homogeneous, enlarged liver and spleen; without distinct macroscopic lesions; lymph nodes are usually not enlarged (Blood 2003;102:4261)
Microscopic (histologic) description
- Spleen
- Diffuse involvement; expansion of the red pulp cords and sinusoids, with atrophy or absence of white pulp (Hum Pathol 2018;74:5, Blood 2020;136:2018)
- Hemophagocytosis may be present (Blood 2020;136:2018)
- Liver and bone marrow: sinusoidal infiltration (Histopathology 2014;64:171, Blood 2003;102:4261, Blood 2020;136:2018)
- Median bone marrow tumor burden ~30% (5 - 80%) (Am J Surg Pathol 2016;40:676, Blood 2020;136:2018)
- Bone marrow tumor burden directly related to neutropenia (Hum Pathol 2016;50:109)
- Median bone marrow tumor burden ~30% (5 - 80%) (Am J Surg Pathol 2016;40:676, Blood 2020;136:2018)
Microscopic (histologic) images
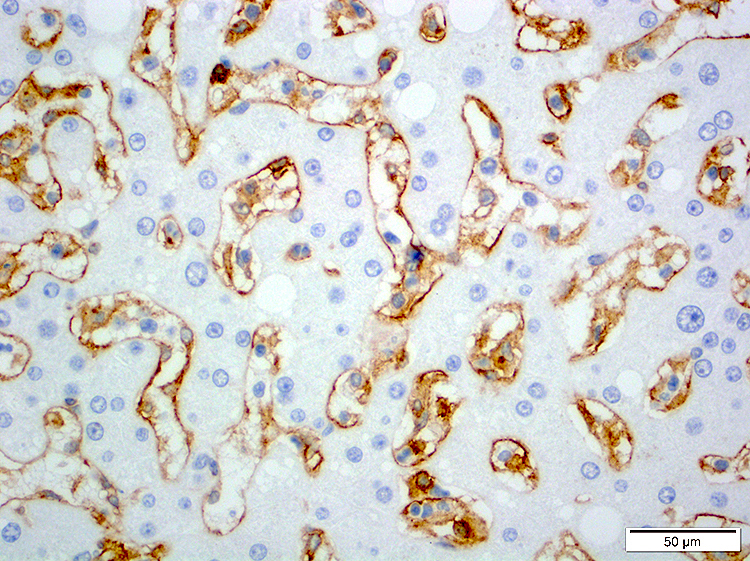
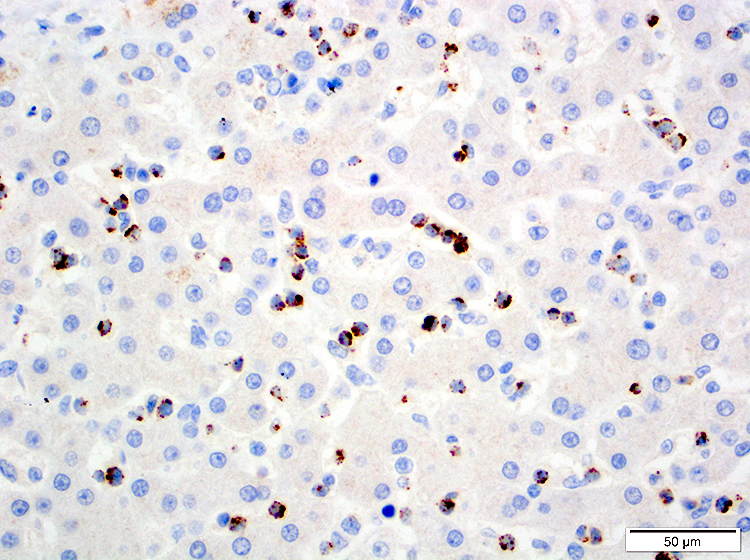
Contributed by Roberto N. Miranda, M.D.
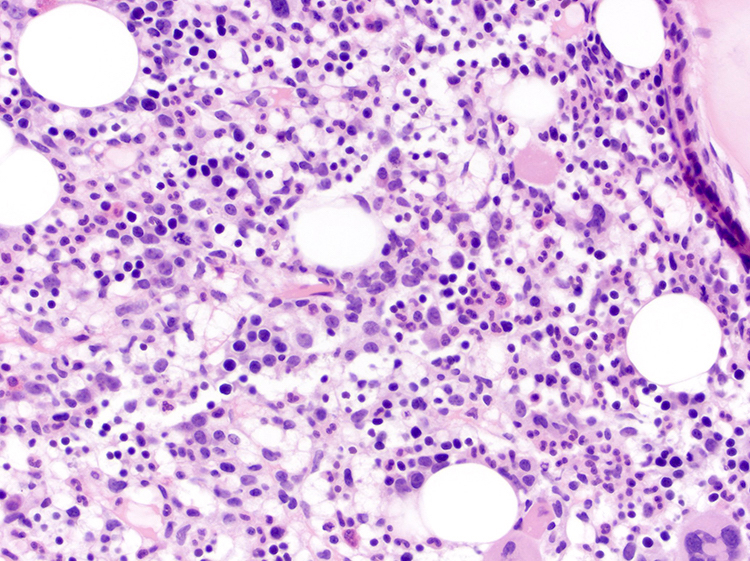

Bone marrow infiltration
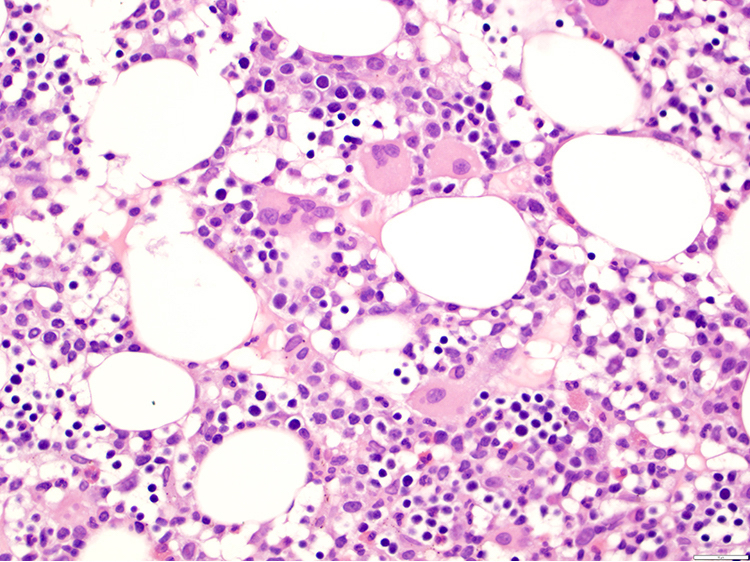
Bone marrow with dyspoietic changes
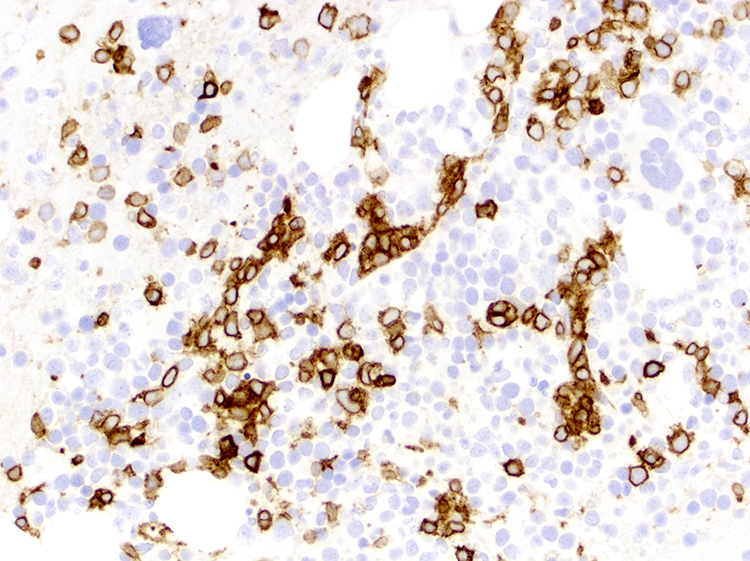
CD3 positive
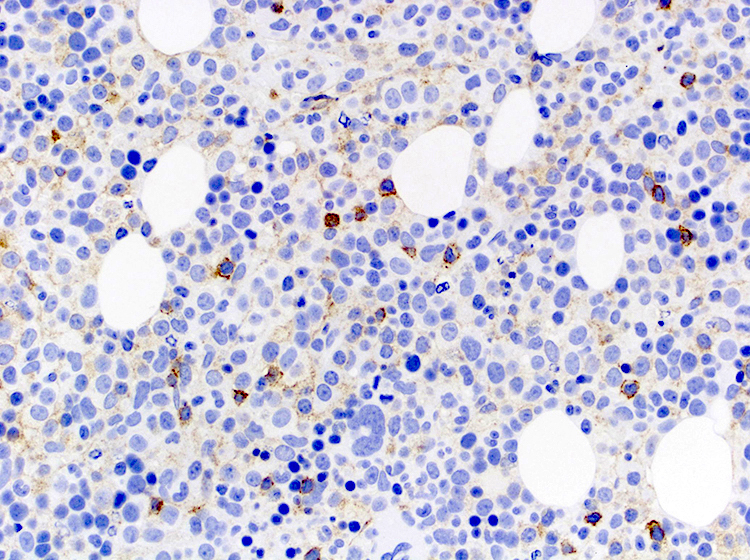
CD4 negative

CD8 negative
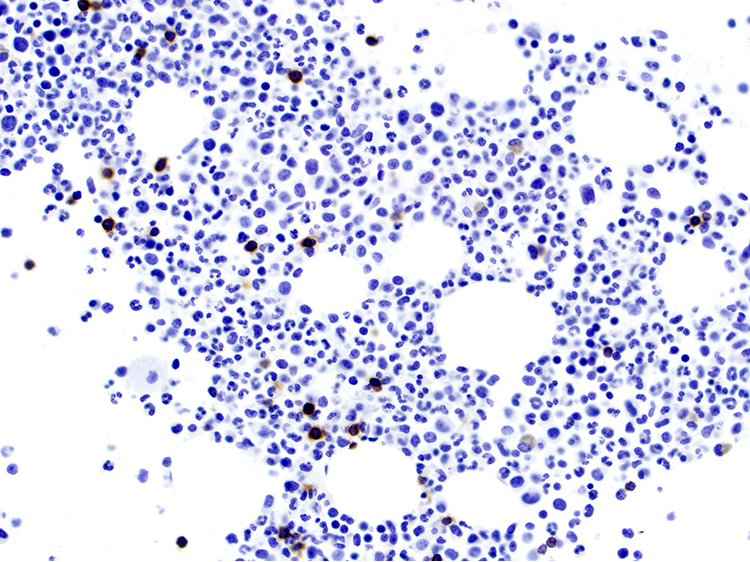
TCR βF1 negative
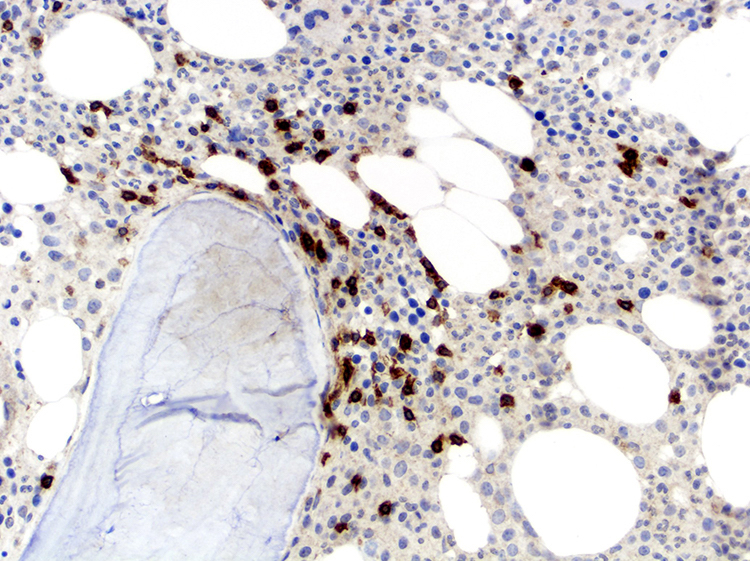
TCRγδ positive
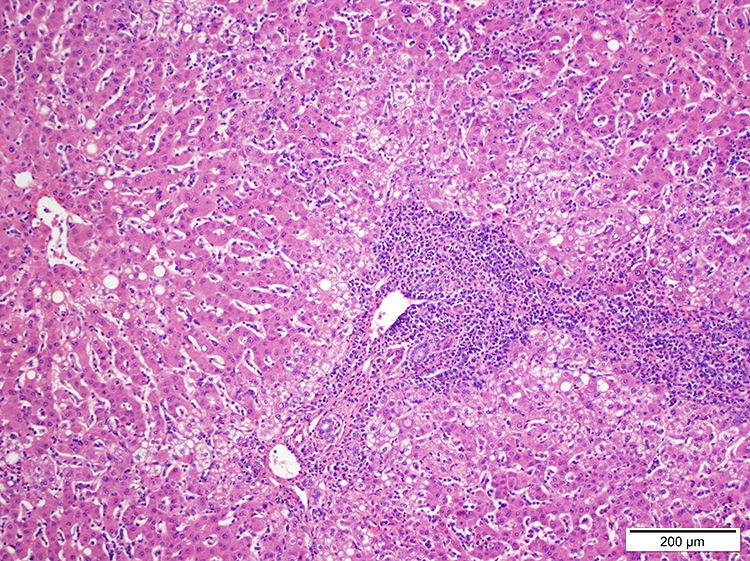
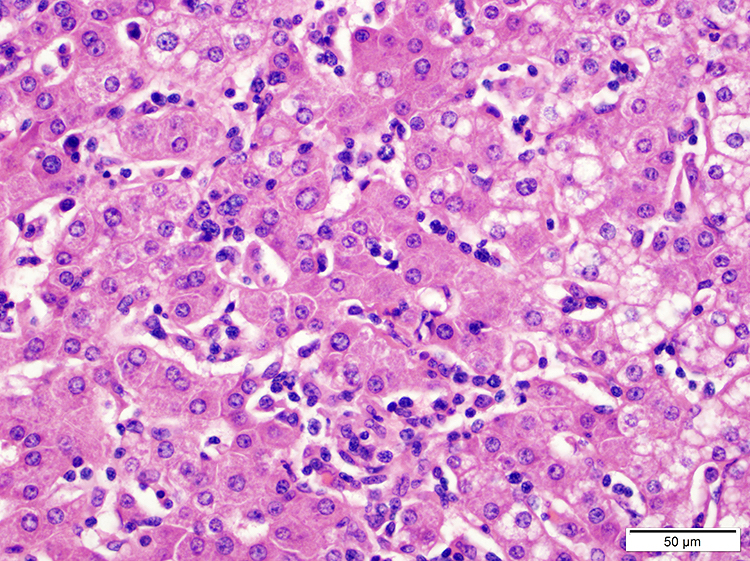
Liver infiltration
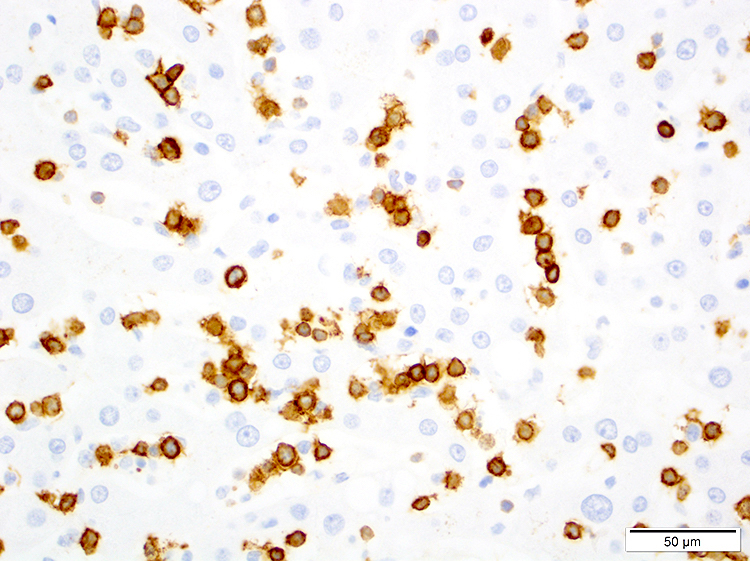
HSTCL: CD3 positive
HSTCL: CD4 negative

CD8 positive
TIA1 positive
Small size morphology
Intermediate size morphology
Blastic morphology
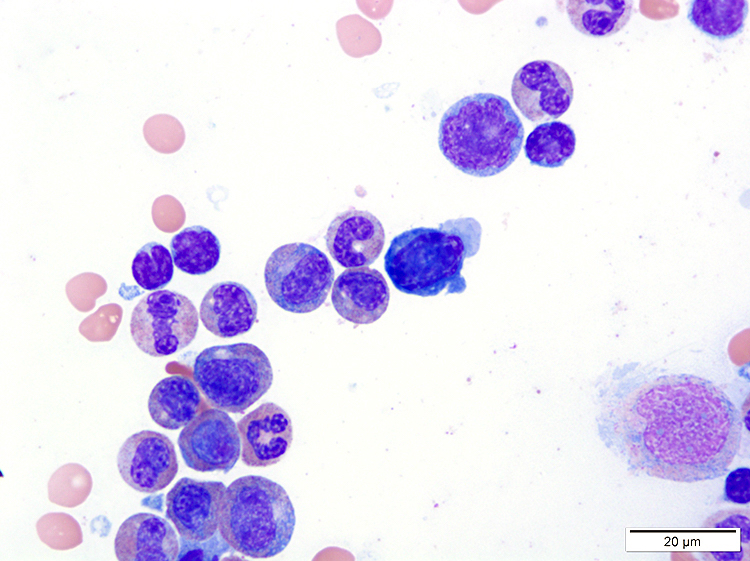
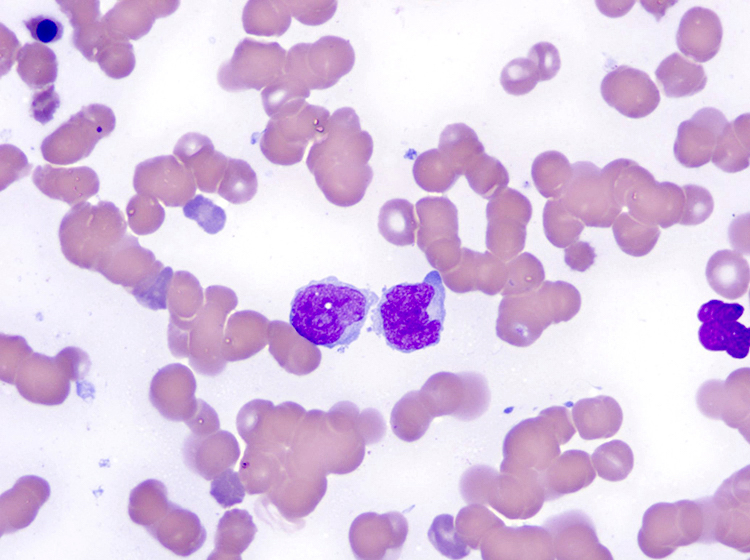
Cytology description
- Variable
- Usually monotonous, small to intermediate size cells with pale agranular cytoplasm, round / oval nuclei, moderately condensed chromatin and inconspicuous nucleoli (Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Blood 2003;102:4261, Blood 2020;136:2018, Semin Diagn Pathol 2020;37:47)
- Blastic cells (medium to large cells with high nucleus to cytoplasm ratio, fine chromatin, without nucleoli) (Am J Clin Pathol 2001;116:410)
- Usually monotonous, small to intermediate size cells with pale agranular cytoplasm, round / oval nuclei, moderately condensed chromatin and inconspicuous nucleoli (Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Blood 2003;102:4261, Blood 2020;136:2018, Semin Diagn Pathol 2020;37:47)
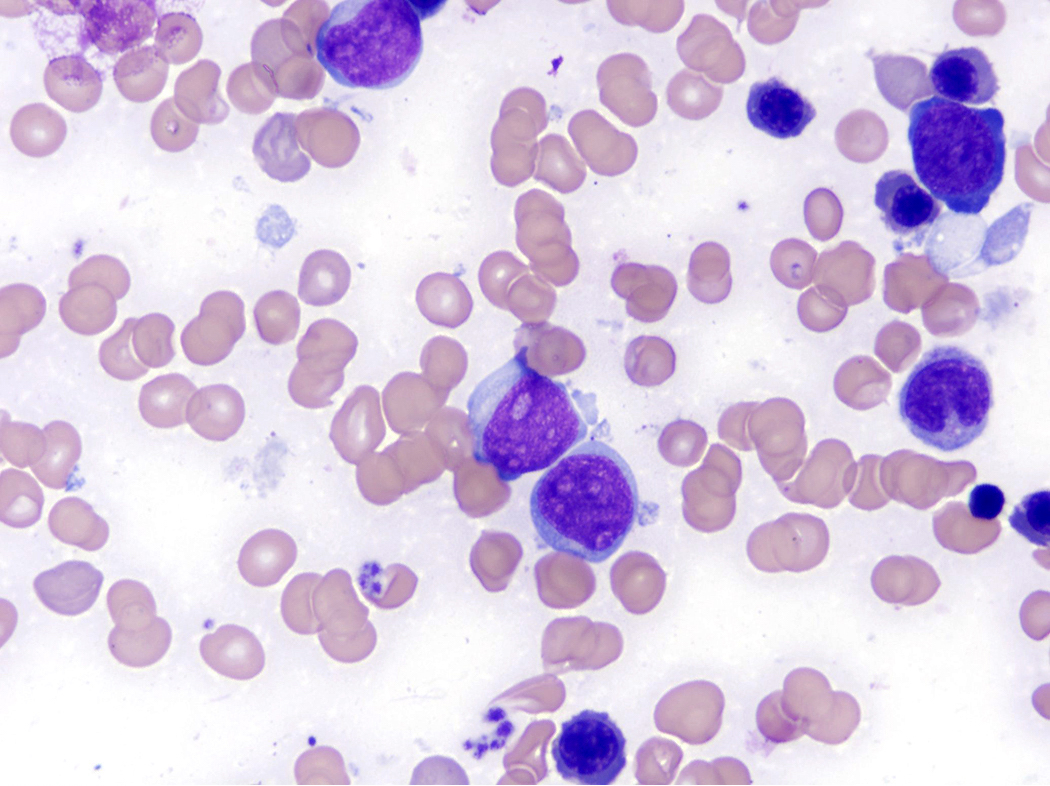
- Background trilineage dyspoietic changes in bone marrow (Hum Pathol 2016;50:109)
- Dysmegakaryopoiesis is most common: hypolobated or small size nuclei
- Hemophagocytosis (< 5%) (Hum Pathol 2018;74:5, Semin Diagn Pathol 2020;37:47)
Positive stains
- T cell antigens: CD2, CD3, CD7, TIA1, granzyme M, Fas ligand (Ann Diagn Pathol 2017;26:16, Hum Pathol 2016;50:109, Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Histopathology 2014;64:171, Blood 2003;102:4261, Blood 2020;136:2018)
- CD56: 67% of cases; related to immune disorders
- Ki67 variable (Hum Pathol 2018;74:5)
- TCRγδ
Negative stains
- CD1a, CD4, CD5, CD8, CD10, CD57, CD94, TdT, Epstein-Barr virus encoded small RNAs (EBER) (Ann Diagn Pathol 2017;26:16, Hum Pathol 2016;50:109, Am J Surg Pathol 2016;40:676, Am J Surg Pathol 2017;41:82, Histopathology 2014;64:171, Blood 2003;102:4261, Blood 2020;136:2018)
- B cell antigens: CD19, CD20 and CD25
- Mature and nonactivated cytotoxic T cell immunophenotype: granzyme B (albeit positive in 38% of cases) and perforin
- TCRαβ (20%): when present appears to carry a poor prognosis
- Follicular T cell markers (Semin Diagn Pathol 2020;37:47):
- Rare cases negative for TCRγδ and αβ (TCR silent) (Hum Pathol 2018;74:5)
Flow cytometry description
- Helpful for diagnosis (Semin Diagn Pathol 2020;37:47, Leuk Res 2021;108:106614):
Flow cytometry images
Contributed by Roberto N. Miranda, M.D.
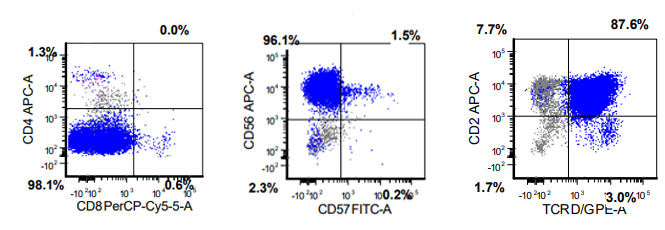
Positivity for CD2, TCRγδ and CD56
Molecular / cytogenetics description
- Gamma delta origin: biallelic rearrangement of TRG (Am J Surg Pathol 2017;41:82, Blood 2003;102:4261)
- Chromatin modifying genes (~60%): SETD2, INO80, TET3 and SMARCA2 (Hum Pathol 2018;74:5, Blood 2020;136:2018)
- Mutations in JAK / STAT pathway
- STAT3 (10%) and STAT5B (30%) mutations
- RHOA, CD28 and CCR4 are usually absent (more common in other T cell lymphomas) (PLoS One 2014;9:e102977)
- DNA methylation profiling (Haematologica 2019;104:e104)
- Hypermethylated genes: CD5, BCL11B, CXCR6, GIMAP7
- Hypomethylated genes: ADARB1, NFIC, NR1H3, ST3GAL3
- Mutation of PIK3CD in up to 10% of cases (Cancer Discov 2017;7:369)
- Aberrant karyotype (67%)
- Isochromosome (7q) or ring chromosome 7 (Ann Diagn Pathol 2017;26:16, Genes Chromosomes Cancer 2002;33:243, Cancer Treat Res 2019;176:185, Blood 2020;136:2018)
- ~50% of cases
- Primary chromosomal aberration
- Loss of 7p22.1p14.1
- Gain of 7q22.11q31.1
- Trisomy 8 is usually present (Hum Pathol 2016;50:109, Am J Surg Pathol 2016;40:676, Blood 2020;136:2018)
- ~ 70% of cases
- Secondary event
- If present at time of diagnosis, there is a significantly shorter overall survival and progression free survival
Sample pathology report
- Bone marrow (right iliac crest) core and clot specimen; aspirate smears and peripheral blood:
- Hepatosplenic T cell lymphoma
- Flow cytometry immunophenotype demonstrated aberrant T cells with loss of CD4 and CD8, positive for T cell receptor gamma delta chain (see comment)
- Comment: According to clinical records, patient is a 28 year old man who has a history of Crohn's disease, for which he was receiving azathioprine and tumor necrosis alpha receptor antagonist. Patient reports malaise and fever for 3 months. On physical exam, patient had massive splenomegaly (8 cm below costal margin) and hepatomegaly. Laboratory findings showed leukopenia, severe anemia and thrombocytopenia. Additional testing proved negative for antiglobulin testing, negative for HIV, hepatitis B, hepatitis C and HTLV1.
- Bone marrow core biopsy and clot sections show similar features. There is 70% cellularity with trilineage hematopoiesis. Megakaryocytes are adequate in number and range from small, hypolobated forms to megakaryocytes of normal size and shape. There are scattered small clusters of small to intermediate size lymphocytes with hyperchromatic nuclei with irregular nuclear contours.
- Bone marrow aspirate smears show trilineage hematopoiesis with mild dysmegakaryopoiesis. There are approximately 15% lymphocytes, of small to intermediate size, with clear and agranular cytoplasm and central hyperchromatic nuclei with irregular nuclear contours.
- Immunohistochemical studies were performed in bone marrow core biopsy and the T cell marker CD3 highlights lymphocytes in an interstitial and sinusoidal pattern, representing approximately 10% of marrow cells. Atypical lymphocytes are also highlighted with CD2, CD7, CD56, TIA1 and granzyme M. The T cell receptor gamma delta is positive in lymphocytes, while the T cell receptor alpha beta (βF1 clone) is negative. CD4 and CD8 are negative in atypical lymphocytes. The following markers are also negative in lymphocytes: CD1a, CD5, CD10, CD57, EBER (EBV in situ hybridization), TCL1 and TdT.
- Concurrent flow cytometry immunophenotype demonstrates that approximately 15% of marrow cells are T lymphocytes, positive for CD2, CD7, CD52, CD56 and T cell receptor gamma delta. The atypical lymphocytes are negative for CD4, CD5, CD8, CD57 and T cell receptor alpha beta. The B lymphocytes are polytypic.
- Molecular testing revealed monoclonal T cell receptor gene rearrangement of gamma (V gamma 4 family) and beta chains. Next generation sequencing showed mutation of STAT5B. The specimen was negative for IGH gene rearrangement.
- Cytogenetic analysis revealed isochromosome 7 and trisomy 8
- Clinical correlation and followup is recommended.
Differential diagnosis
- T cell large granular lymphocytic (LGL) leukemia (Am J Clin Pathol 2015;144:607, Am J Surg Pathol 2017;41:82):
- Elderly patients
- Absent or mild splenomegaly
- Liver may be involved but not enlarged
- Neoplastic lymphocytes with azurophilic granules and hyperchromatic nuclei
- Expression of CD5, CD8, CD57, granzyme B and TCRαβ
- Diagnostic challenge in cases of γδ T LGL:
- When compared with HSTCL, has a higher presence of azurophilic granules and unlikely to have massive splenomegaly
- Marrow infiltration is interstitial and may be focally sinusoidal but without expanding sinuses
- Aggressive NK cell leukemia / lymphoma:
- T cell prolymphocytic leukemia (Blood 2019;134:1132):
- T cell lymphoblastic leukemia / lymphoma (Haematologica 2020;105:2524):
- Splenic marginal zone lymphoma:
- Infiltration of white pulp and secondarily red pulp
- Small sized lymphocytes with abundant pale cytoplasm in spleen and villous lymphocytes in peripheral blood
- Chronic active EBV infection (Blood 2020;136:2018):
- Bone marrow infiltration of EBV+ small to intermediate sized lymphocytes (B, T or NK cells)
- Hemophagocytosis may be present
- No significant lymphocytic atypia or phenotypic abnormalities
- Nonsplenic cytotoxic T cell lymphoma with γδ+ phenotype (Histopathology 2014;64:171):
- Skin involvement
- Absence of hepatosplenomegaly
Additional references
Board review style question #1
Which of the following immunophenotypic patterns corresponds to hepatosplenic T cell lymphoma?
- CD2+, CD3+, CD4+, CD5-, TIA1+, granzyme B+, TCRγδ+
- CD2+, CD3+, CD4-, CD5-, TIA1+, granzyme M+, TCRγδ+
- CD2+, CD3-, CD4+, CD5+, CD7+, CD8+, TCRγδ+
- CD2+, CD3-, CD4+, CD5+, CD7-, CD8-, TCRγδ+
- CD2-, CD3-, CD4-, CD5+, CD7-, CD8-, TCRγδ+
Board review style answer #1
B. CD2+, CD3+, CD4-, CD5-, TIA1+, granzyme M+, TCRγδ+
Comment here
Reference: Hepatosplenic T cell lymphoma
Comment here
Reference: Hepatosplenic T cell lymphoma
Board review style question #2
Which of the following cytogenetic and molecular abnormalities are found in hepatosplenic T cell lymphoma?
- Del(6q) and RHOA1 mutation
- Inversion 14 and TCL1 rearrangement
- Isochromosome 7 and STAT5B mutation
- t(2;5) and JAK / STAT activation
- 6p25 and DUSP22 / IRF4
Board review style answer #2
