Skin nonmelanocytic tumor
Adnexal tumors
Sweat gland derived (apocrine & eccrine glands)
Endocrine mucin producing sweat gland carcinoma
Author: Robert E. LeBlanc, M.D.

Last author update: 29 September 2020
Last staff update: 30 March 2023
Copyright: 2018-2025, PathologyOutlines.com, Inc.
PubMed Search: Endocrine mucin producing sweat gland carcinoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: LeBlanc R. Endocrine mucin producing sweat gland carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticendocrinemucinsweatglcarcinoma.html. Accessed September 16th, 2025.
Definition / general
- Low grade adenocarcinoma of cutaneous sweat gland origin
- Predilection for the eyelids of older women
Essential features
- Rare, low grade adenocarcinoma of sweat gland origin that often arises on or near the eyelids of older women
- Can recur if incompletely excised and may be a precursor to mucinous carcinoma; however, there are no reported cases of metastases
- Must be distinguished from metastatic adenocarcinoma; resembles mammary solid papillary carcinoma / endocrine ductal carcinoma with cystic and solid architecture (solid components show cribriform, papillary and pseudopapillary patterns punctuated by mucin filled spaces)
- Key feature is neuroendocrine expression; elaboration of a myoepithelial layer by immunohistochemistry is helpful to confirm primary cutaneous origin and exclude metastatic adenocarcinoma
ICD coding
- C44.191 (eyelid): other specified malignant neoplasm of skin of unspecified eyelid, including canthus
Epidemiology
- Higher incidence among women than men (Am J Surg Pathol 2005;29:1330)
- Often elderly adults, not described in children
Sites
- Head and neck, eyelid most common
Etiology
- Given the low incidence of this disease, its etiology is incompletely understood
- Tumor is thought to be analogous to mammary solid papillary carcinoma / endocrine ductal carcinoma in situ of and exhibits a similar immunophenotype, including evidence of a surrounding myoepithelial cell layer
Clinical features
- Lesions can be solitary or less often multiple (regional)
- Translucent cyst (sometimes multiloculated) may resemble hidradenoma
- Cases with lesser developed cystic components appear as skin colored nodules
Diagnosis
- Diagnosis requires correlations with immunohistochemistry, clinical history and clinical examination findings to exclude metastatic adenocarcinomas from breast, salivary gland or viscera
Prognostic factors
- No reported cases of metastasis
- Some cases have contiguous primary cutaneous mucinous carcinoma
- Recurrence is common when the tumor is incompletely excised
Case reports
- 71 year old woman with a papule on her left upper eyelid (Am J Dermatopathol 2016;38:636)
- 75 year old woman with a skin colored eyelid nodule and a left breast mass (Am J Dermatopathol 2015;37:425)
- 83 year old woman with nodules on her bilateral lower eyelids (Am J Dermatopathol 2016;38:789)
Treatment
- Excision or Moh's micrographic surgery
Clinical images
Images hosted on other servers:

EMPSGC on the eyelid
Microscopic (histologic) description
- Nodular, often multilobulated dermal tumor with solid areas and cystic spaces
- Solid areas may show cribriform architecture or pseudorosettes, papillae with fibrovascular cores or smaller pseudopapillae
- Solid areas are often punctuated by mucin filled cystic spaces that range in appearance from small holes and clefts to large, hidrocystoma-like components
- Some lesions closely resemble hidrocystoma on low power but show multilayering of neoplastic cells and Roman bridges analogous to breast ductal carcinoma in situ
- Lesions frequently appear contiguous with benign ducts
- Most lesions have an inconspicuous and discontinuous myoepithelial cell layer surrounding them; however, there is disagreement as to whether to classify endocrine mucin producing sweat gland carcinoma as purely in situ carcinoma or invasive adenocarcinoma (Am J Surg Pathol 2005;29:1330, Am J Dermatopathol. 2013;35:117, Requena: Cutaneous Adnexal Neoplasms, 1st Edition, 2018)
- Has 1 to 3 layers of bland columnar secretory cells with occasional apical snouts, intracellular and extracellular mucin, moderate amounts of cytoplasm with a basophilic hue, ovoid nuclei (slightly larger than those of surrounding eccrine ductal epithelia), bland or sometimes stippled nuclear chromatin and minimal to no nuclear pleomorphism or mitotic activity (Am J Surg Pathol 2005;29:1330)
- Lesions are sometimes contiguous with primary cutaneous mucinous carcinoma (or adjacent acellular pools of mucin suspicious for mucinous carcinoma) or have a component of infiltrative nests of cells with mild nucleomegaly and hyperchromasia
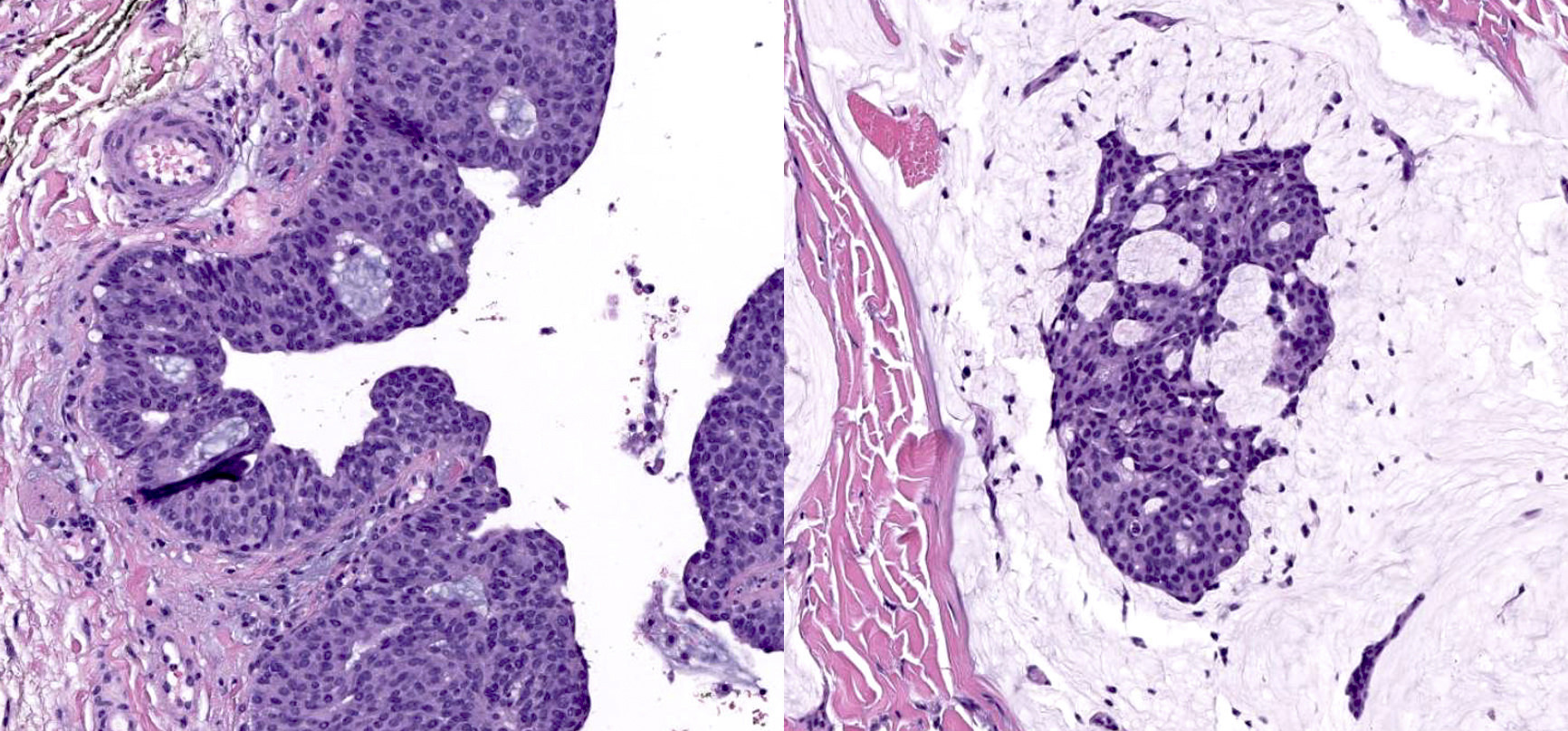
Microscopic (histologic) images
Contributed by Robert E. LeBlanc, M.D.
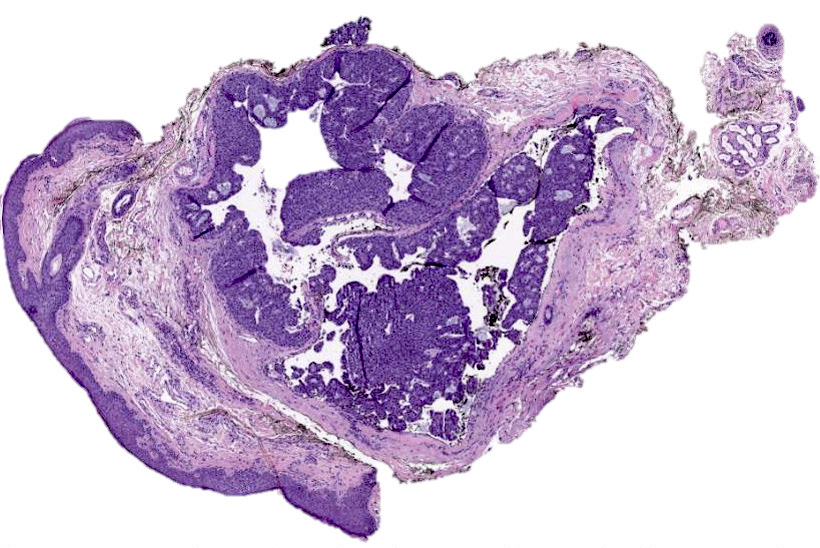
Anodular, solid and cystic appearance

Solid component with cribriform architecture
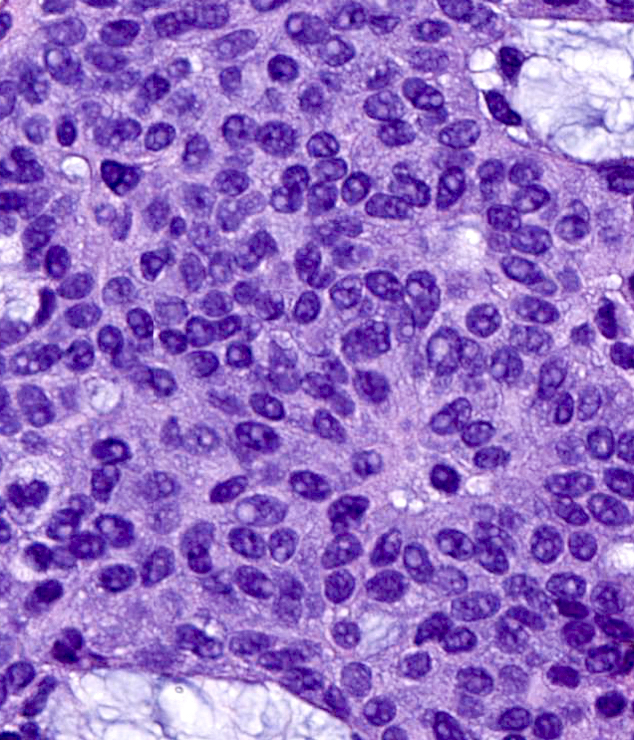
Small and monotonous columnar epithelial cells
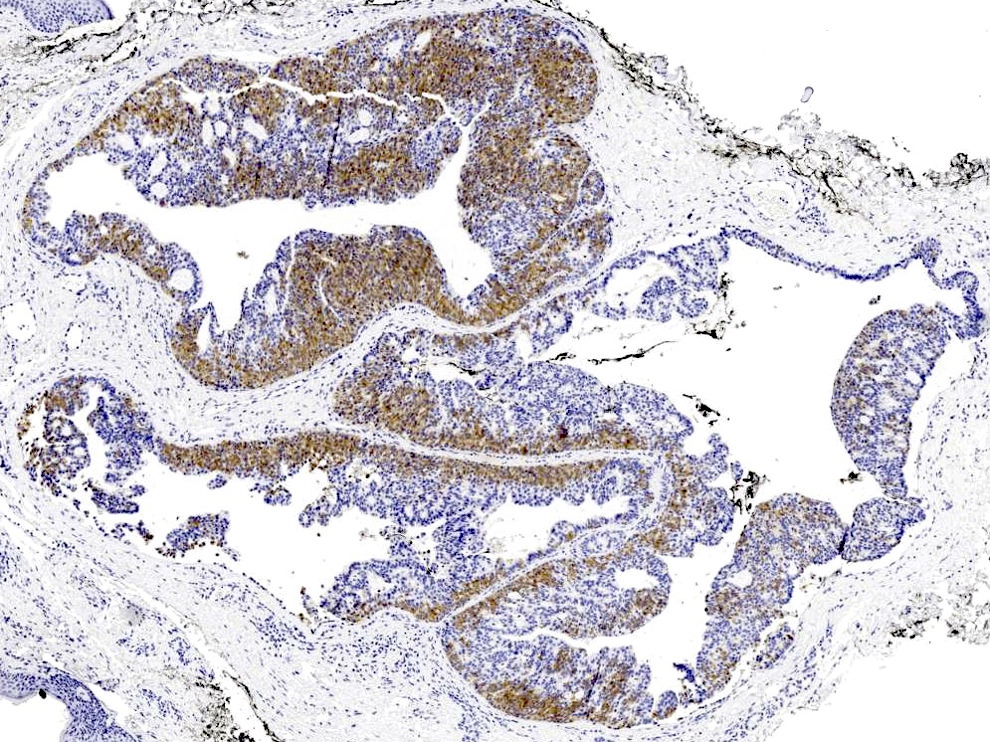
Synaptophysin
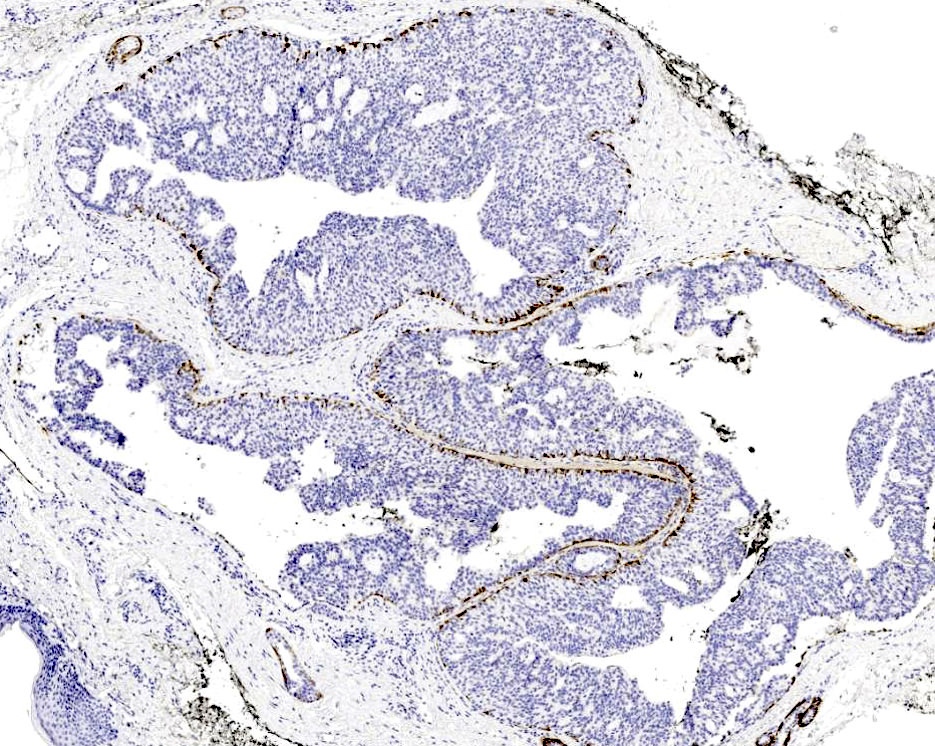
Calponin
Comparison with
primary cutaneous
mucinous carcinoma
Positive stains
- Neuroendocrine expression: NSE, synaptophysin, chromogranin, CD56, INSM1
- Mucicarmine highlights intracellular and extracellular mucin
- CK7, ER / PR, GCDFP-15 and GATA3 (Am J Dermatopathol 2016;38:789) are also positive in adenocarcinoma of breast and salivary gland and cannot distinguish it from endocrine mucin producing sweat gland carcinoma
- Calponin, SMA and p63 highlight myoepithelial layer around the dermal nodules and intraductal components, providing evidence of a primary cutaneous origin but care should be taken not to overinterpret staining of adjacent benign eccrine structures
- AE1 / AE3, CAM 5.2, EMA, E-cadherin, CD57, CEA (patchy in areas with ductal differentiation)
Molecular / cytogenetics description
- Cytogenetics reveal diploidy (J Dermatol 1994;21:117, Am J Dermatopathol 2000;22:166)
- No mutations in TP53, PIK3CA, AKT1, KRAS, GNAS and EGFR or HER2/neu amplifications have been identified to date in EMPSGC or cutaneous mucinous carcinoma (Am J Dermatopathol 2000;22:166, Am J Surg Pathol 2005;29:764, Am J Dermatopathol 2016;38:636, Am J Surg Pathol 2005;29:764, J Cutan Pathol 2020 [Online ahead of print])
Sample pathology report
- Skin, left upper eyelid, shave:
- Endocrine mucin producing sweat gland carcinoma, present at the peripheral edge and base of specimen (see comment)
- Comment: The bland cytomorphology, evidence of neuroendocrine expression (INSM1 stains tumoral nuclei and synaptophysin stains tumoral cytoplasm) and variable presence of a p63 positive myoepithelial layer surrounding the lesion together support this diagnosis.
Differential diagnosis
- Apocrine adenoma:
- Extensive decapitation secretion, absence of neuroendocrine differentiation, absence of mucin and enlarged epithelioid nuclei with conspicuous nucleoli
- Apocrine carcinoma:
- High grade cytologic atypia exceeding that of endocrine mucin producing sweat gland carcinoma (EMPSGC), usually no mucin production
- Basal cell carcinoma:
- Rare cases exhibit neuroendocrine differentiation; however, palisading of peripheral cells with retraction of the adjacent stroma and increased apoptoses and mitoses favor the latter
- Dermal duct tumor:
- Absence of neuroendocrine differentiation, no cribriform architecture or mucin filled clefts, more prominent ductular differentiation with secretory spaces lined by cuticle, foci of necrosis
- Hidrocystoma:
- Bland lining lacks architectural complexity, cytologic atypia or neuroendocrine marker expression
- Nodular hidradenoma:
- Also has variable cystic and solid conformation but an absence of neuroendocrine differentiation, attachment to the epidermis and vascular spaces favor hidradenoma and a greater diversity of cell types including eosinophilic polygonal cells, squamous cells, clear cells and goblet cells
- Primary cutaneous mucinous adenocarcinoma:
- May be contiguous with EMPSGC suggesting that EMPSGC could be a precursor lesion; small cribriform or tubular islands of epithelioid cells in pools of mucin partitioned by strands of dermal collagen
Additional references
Practice question #1
Staining with which of the following markers would favor the diagnosis of metastatic adenocarcinoma over endocrine mucin producing sweat gland carcinoma?
- CK7
- CK20
- GATA3
- p63
Practice answer #1
B. CK20 expression would raise consideration for metastatic carcinoma of colorectum. Endocrine mucin producing sweat gland carcinoma otherwise shares an immunophenotype with metastatic carcinomas of breast and salivary gland and expresses CK7 and GATA3. p63 is not expressed by the epithelial cells of EMPSGC but highlights a discontinuous myoepithelial layer surrounding the neoplasm.
Comment Here
Reference: Endocrine mucin producing sweat gland carcinoma
Comment Here
Reference: Endocrine mucin producing sweat gland carcinoma
Practice question #2
Which of the following is the most common site of origin for endocrine mucin producing sweat gland carcinoma?
- Eyelid
- Inferior helix
- Nasal ala
- Scalp
Practice answer #2
A. Endocrine mucin producing sweat gland carcinoma has a predilection for the head and neck and is most often located on or around the eyelids of older adults.
Comment Here
Reference: Endocrine mucin producing sweat gland carcinoma
Comment Here
Reference: Endocrine mucin producing sweat gland carcinoma
