Ovary
Sex cord stromal tumors
Pure stromal tumors
Fibroma
Author: Gulisa Turashvili, M.D., Ph.D.
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 16 March 2021
Last staff update: 20 May 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Fibroma[TI] ovary[TIAB] "last 10 years"[dp]
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Turashvili G. Fibroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarytumorfibroma.html. Accessed September 15th, 2025.
Definition / general
- Benign stromal tumor composed of fibroblastic cells within a variably collagenous stroma
Essential features
- Benign stromal tumor composed of spindled, ovoid to round cells within a variably collagenous stroma
- Variants include fibroma with minor sex cord elements, cellular fibroma and mitotically active cellular fibroma
- Important differential diagnoses for cellular fibroma include diffuse adult type granulosa cell tumor and fibrosarcoma
- Gorlin syndrome should be suspected in young patients with bilateral ovarian fibroma
- Long term follow up is recommended for cellular fibromas associated with rupture and adhesions due to increased risk of recurrence
ICD coding
Epidemiology
- Most common ovarian stromal tumor
- ~4% of all ovarian tumors (Cancer 1981;47:2663)
- Cellular fibromas represent ~10% of all ovarian fibromas
- Mean age 48 years, uncommon before 30
- Occurs in ~25% of patients with nevoid basal cell carcinoma syndrome (Gorlin syndrome) (J Med Genet 1993;30:460)
- Autosomal dominant disease due to mutations of the human homologue of the Drosophila gene PTCH (patched)
Sites
- Ovary
Pathophysiology
- Neoplastic transformation of ovarian stromal cells due to hereditary or sporadic genetic abnormalities (see Molecular / cytogenetics description)
Clinical features
- Most commonly symptoms related to an ovarian mass, such as abdominal pain or distension and increased urinary frequency or may be incidental
- Can be associated with ovarian torsion (BMC Surg 2014;14:38)
- Rarely hormonal manifestations
- Ascites in large (> 10 cm) tumors in 10% of cases (Am J Obstet Gynecol 1970;107:538)
- Syndromic ovarian fibromas:
- Often diagnosed before the age of 30 years, including children
- Usually bilateral (75%), calcified and nodular, often overlapping medially (leading to misdiagnosis as calcified uterine leiomyoma) (Genet Med 2004;6:530)
- May be renin secreting, leading to gestational hypertension (Br J Obstet Gynaecol 1994;101:1015)
- May recur (Hum Reprod 2001;16:1261, Obstet Gynecol 1983;61:95S)
- Meigs syndrome occurs in ~1% of cases (Am J Obstet Gynecol 1937;33:249, Eur J Obstet Gynecol Reprod Biol 2000;92:199)
- Characterized by the triad of benign adnexal mass, ascites and pleural effusion
- Due to seepage of fluid from ovary into peritoneal cavity and then into 1 or both pleural cavities either via lymphatics or through a communication between abdominal and pleural cavity (lumbocostal triangle)
Diagnosis
- Histologic examination for definitive diagnosis
- Tentative diagnosis can be made grossly and at frozen section evaluation (Semin Diagn Pathol 2002;19:237)
Laboratory
- Can lead to nonspecific increase in serum CA125 (Gynecol Oncol 1995;59:405)
Radiology description
- Ultrasonography:
- Usually solid, homogeneous and hypoechoic mass with posterior acoustic shadowing, similar to a pedunculated subserosal uterine leiomyoma (AJR Am J Roentgenol 1985;144:1239)
- Heterogeneous echogenicity in tumors with necrosis, hemorrhage or cystic degeneration
- Computed tomography:
- Slightly hypoattenuating solid mass with poor, very slow contrast enhancement (Radiographics 2002;22:1305)
- Rarely calcifications
- Magnetic resonance imaging (MRI):
- T1: homogeneous low signal intensity
- T2:
- Well circumscribed mass with low signal intensity (J Magn Reson Imaging 1997;7:465)
- Hyperintense areas due to edema or cystic degeneration
- Characteristic feature is a band of T2 hypointensity separating the tumor from the uterus on all imaging planes
- Gadolinium: heterogeneous enhancement
- May mimic malignancy (Radiographics 2002;22:1305)
Radiology images
Images hosted on other servers:

Bilateral ovarian fibroma on MRI

Unilateral ovarian fibroma on MRI
Prognostic factors
- Excellent in most cases
- Ovarian surface involvement and extraovarian adhesions occur in 6% of cellular fibromas and 10% of mitotically active cellular fibromas (Am J Surg Pathol 2006;30:929)
- Extraovarian spread at surgery in 11% of cellular fibromas and 13% of mitotically active cellular fibromas (Am J Surg Pathol 2006;30:929)
- Cellular fibromas may recur, often after a long interval, warranting long term follow up (Cancer 1981;47:2663)
Case reports
- 15 year old girl with bilateral ovarian fibroma associated with Gorlin syndrome (J Pediatr Adolesc Gynecol 2011;24:e5)
- 19 year old woman with large ovarian fibroma presenting with spontaneous abdominal bleeding (Case Rep Obstet Gynecol 2019;2019:9834915)
- 34 year old woman with mitotically active cellular fibroma that recurred 16 years later (Int J Gynecol Pathol 2020 [Epub ahead of print])
- 40 year old woman with bilateral ovarian fibroma presenting as Meigs syndrome (J Obstet Gynaecol 2013;33:636)
- 66 year old woman with extraovarian fibroma with minor sex cord elements (Int J Surg Pathol 2017;25:472)
Treatment
- Surgical excision (salpingo-oophorectomy, oophorectomy or ovarian sparing procedure with or without hysterectomy depending on patient’s age)
- Cellular fibromas require long term follow up, particularly in the setting of ovarian surface involvement, intraoperative rupture or extraovarian spread (Cancer 1981;47:2663)
Gross description
- Well circumscribed mass with smooth, lobulated surface
- Firm, chalky, solid, white to yellow-white to tan-yellow cut surface that may be whorled
- Frequent edema resulting in softer consistency
- Mean size 6 cm (range 1 - 21.5)
- Usually unilateral (< 10% bilateral)
- Cystic degeneration in ~25% of cases
- Calcifications in ~10% of cases
- ~20% present as pedunculated or polypoid growths on ovarian surface
- With or without hemorrhage or necrosis
- Cellular fibroma:
- Mean size 8 - 9 cm (range 1 - 19)
- Tan-yellow, soft and fleshy cut surface (Cancer 1981;47:2663)
- With or without surface adhesions
- Fibroma associated with Gorlin syndrome:
- Bilateral, multinodular and calcified (J Pediatr Adolesc Gynecol 2011;24:e5)
Gross images
Contributed by Rex Bentley, M.D. and AFIP
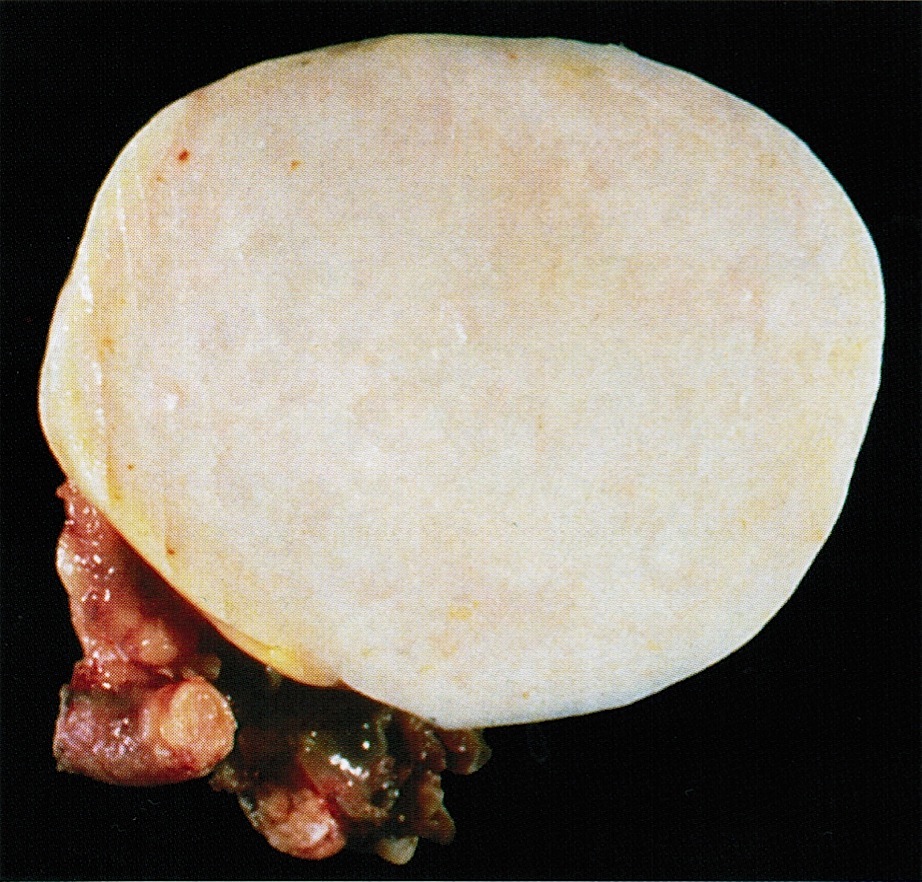
Chalky white surface

Edematous and focally hemorrhagic

Dense white mass
Images hosted on other servers:

Hard white tumor

Fibrothecoma
Frozen section description
- Variably cellular spindle cell neoplasm with fascicular or storiform growth with or without hyaline plaques or calcifications
Frozen section images
Contributed by Gulisa Turashvili, M.D., Ph.D.
Spindle cell neoplasm
Bland spindle cells
Microscopic (histologic) description
- Conventional fibroma:
- Recapitulates ovarian cortex
- Usually well circumscribed but nonencapsulated
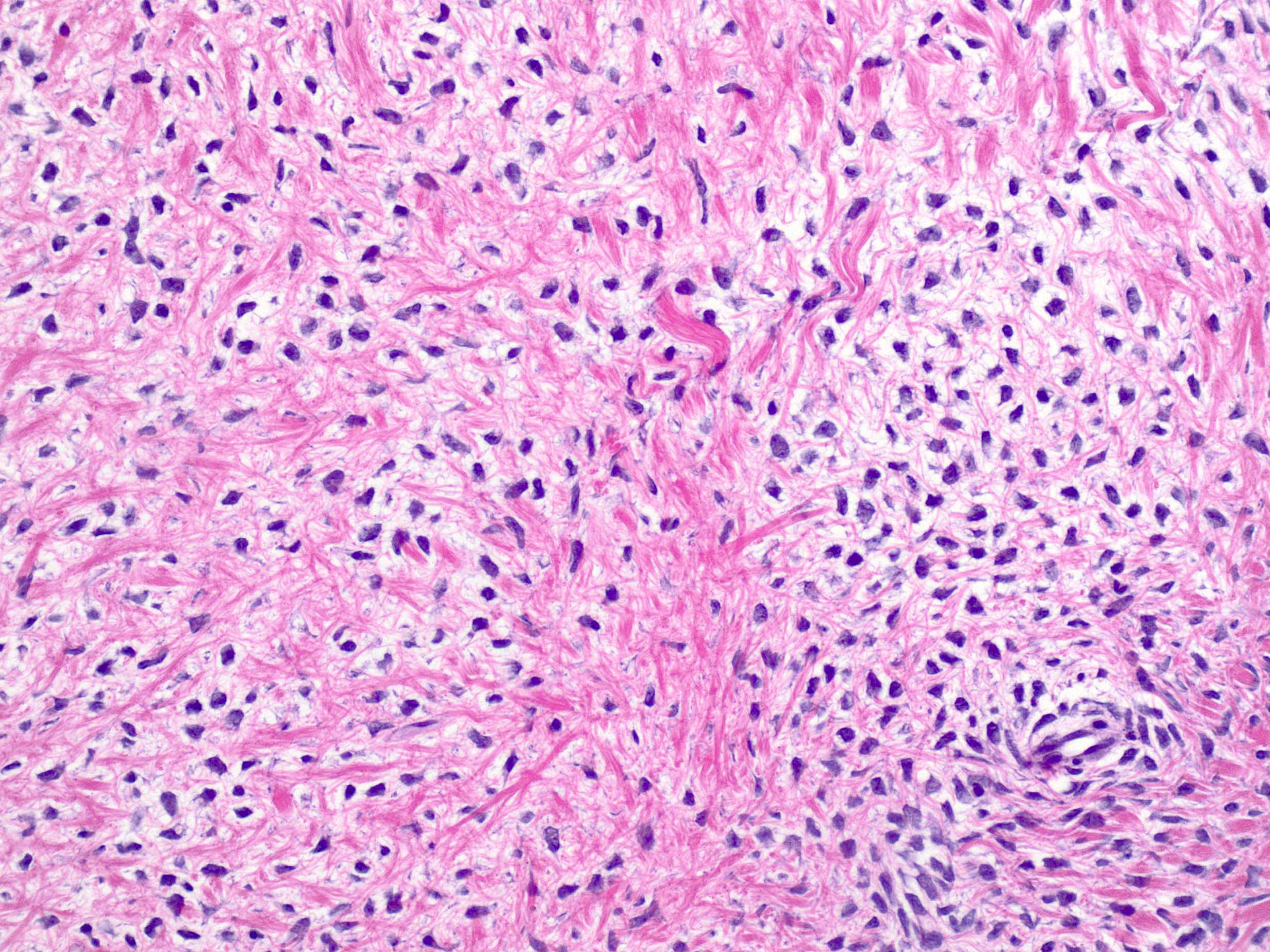
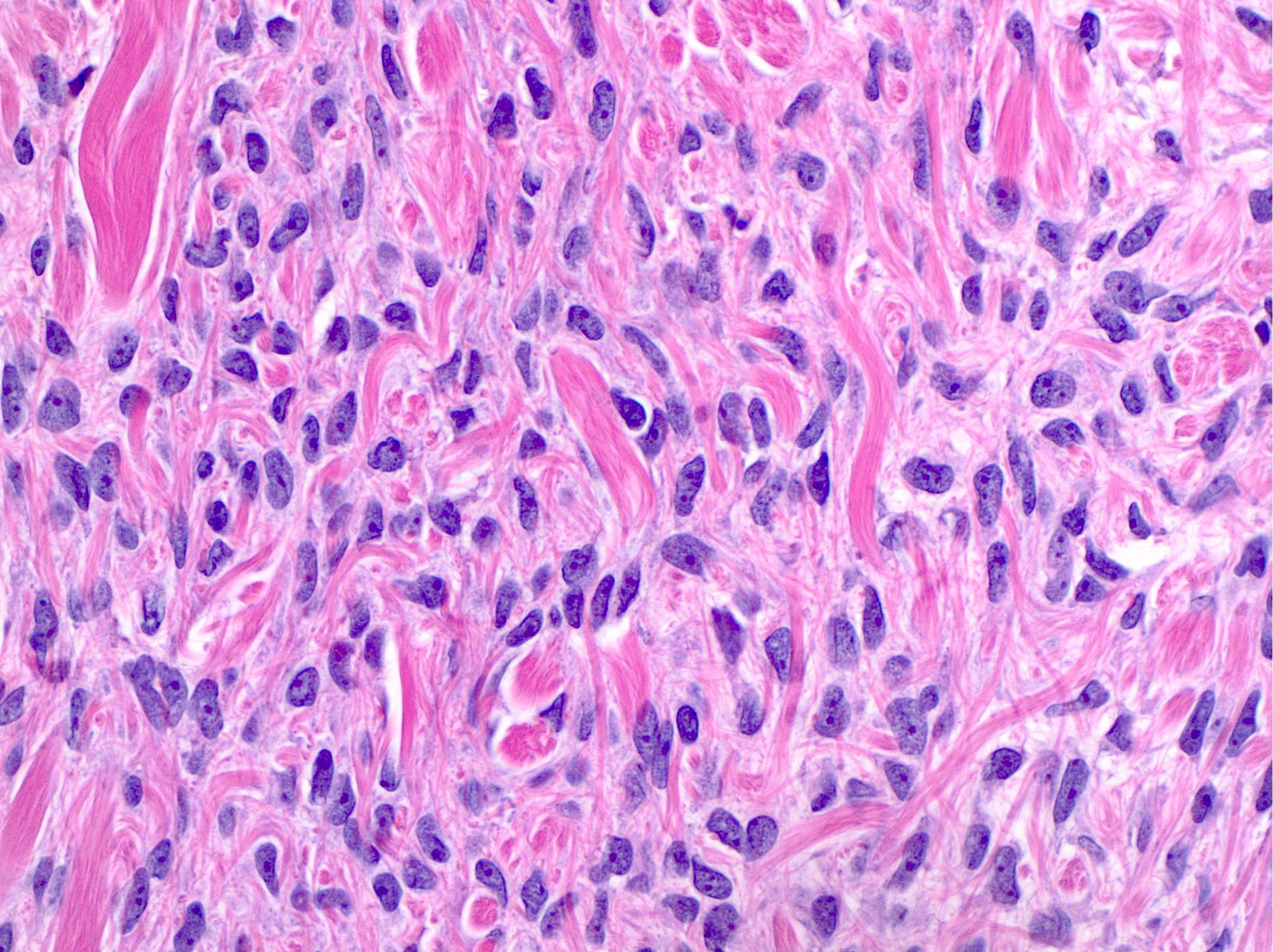
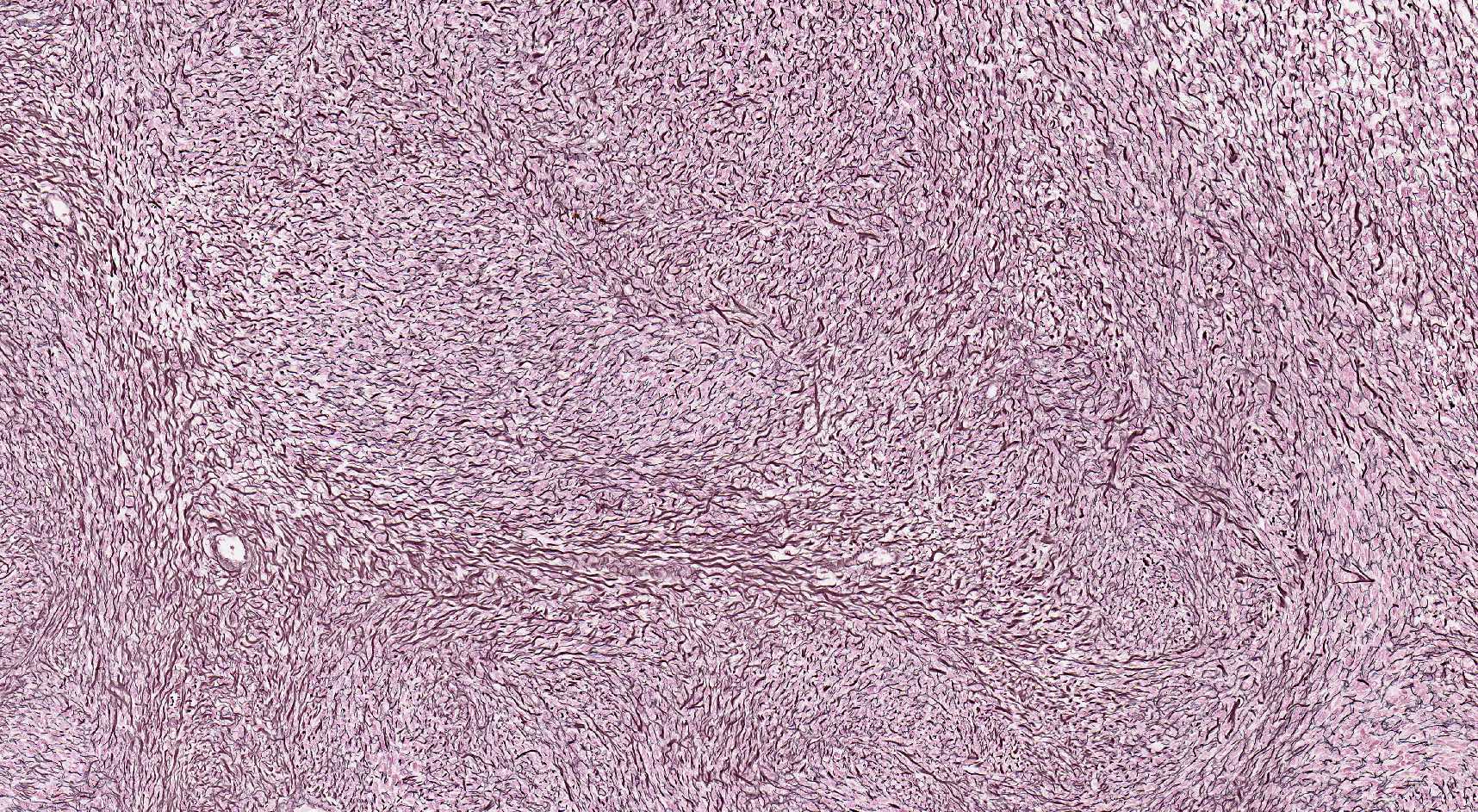
- Variably cellular fascicular or less frequently, storiform growth of tumor cells within a variably collagenous stroma, sometimes with hyaline plaques (Cancer 1981;47:2663)
- Bland spindled to ovoid nuclei with pointy ends and scant eosinophilic cytoplasm blending with surrounding stroma
- Occasional mitoses (usually up to 3 mitoses per 10 high power fields)
- With or without Verocay-like areas (slightly wavy, parallel arrays of spindled nuclei), calcification, edema, hemorrhage, infarct type necrosis, rare groups of luteinized cells
- Rarely intracytoplasmic lipid (may be diagnosed as thecoma), eosinophilic hyaline globules, melanin pigment or bizarre nuclei (Int J Gynecol Pathol 2009;28:356, Int J Gynecol Pathol 2019;38:92, Int J Surg Pathol 2020 [Epub ahead of print])
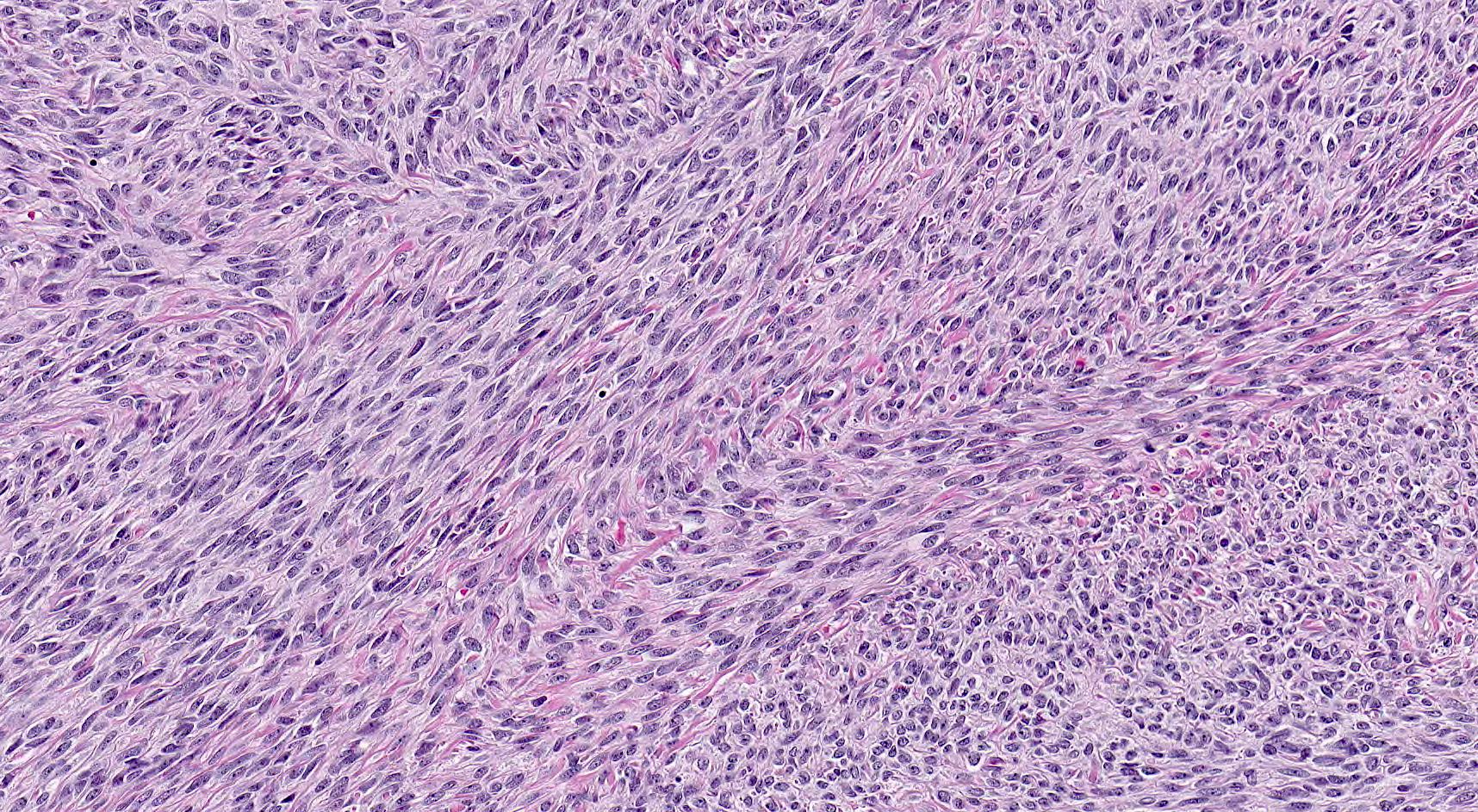
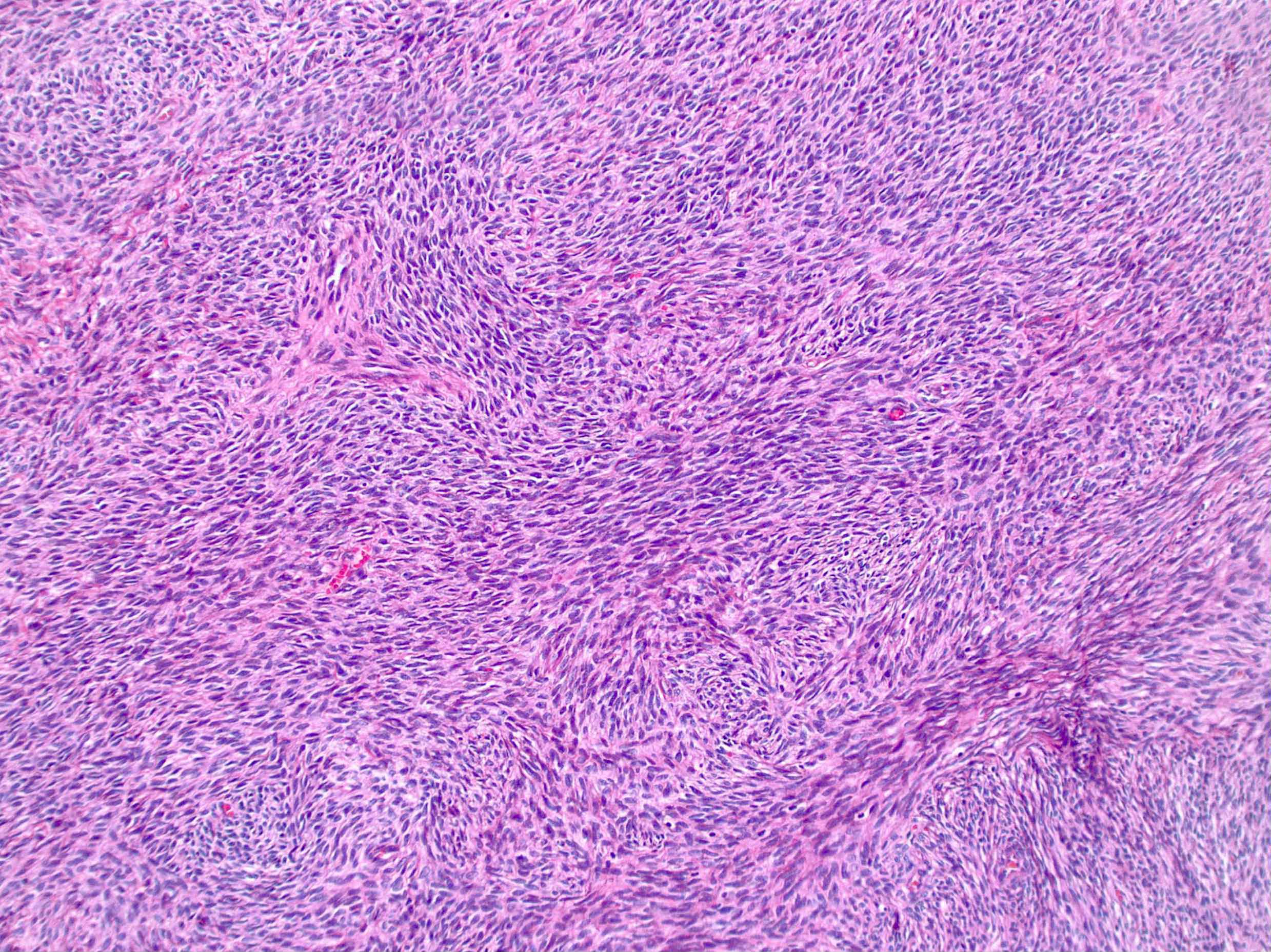
- Cellular fibroma (10% of cases):
- Resembles diffuse type of adult granulosa cell tumor
- Densely cellular with little intercellular collagen
- Bland spindled nuclei with up to 3 mitoses per 10 high power fields (Cancer 1981;47:2663)
- "Mitotically active cellular fibroma" has been proposed for cellular fibromas with ≥ 4 mitoses per 10 high power fields (Am J Surg Pathol 2006;30:929)
- Fibroma with minor sex cord elements:
- Sex cord component accounting for < 10% of overall tumor volume
- No prognostic significance
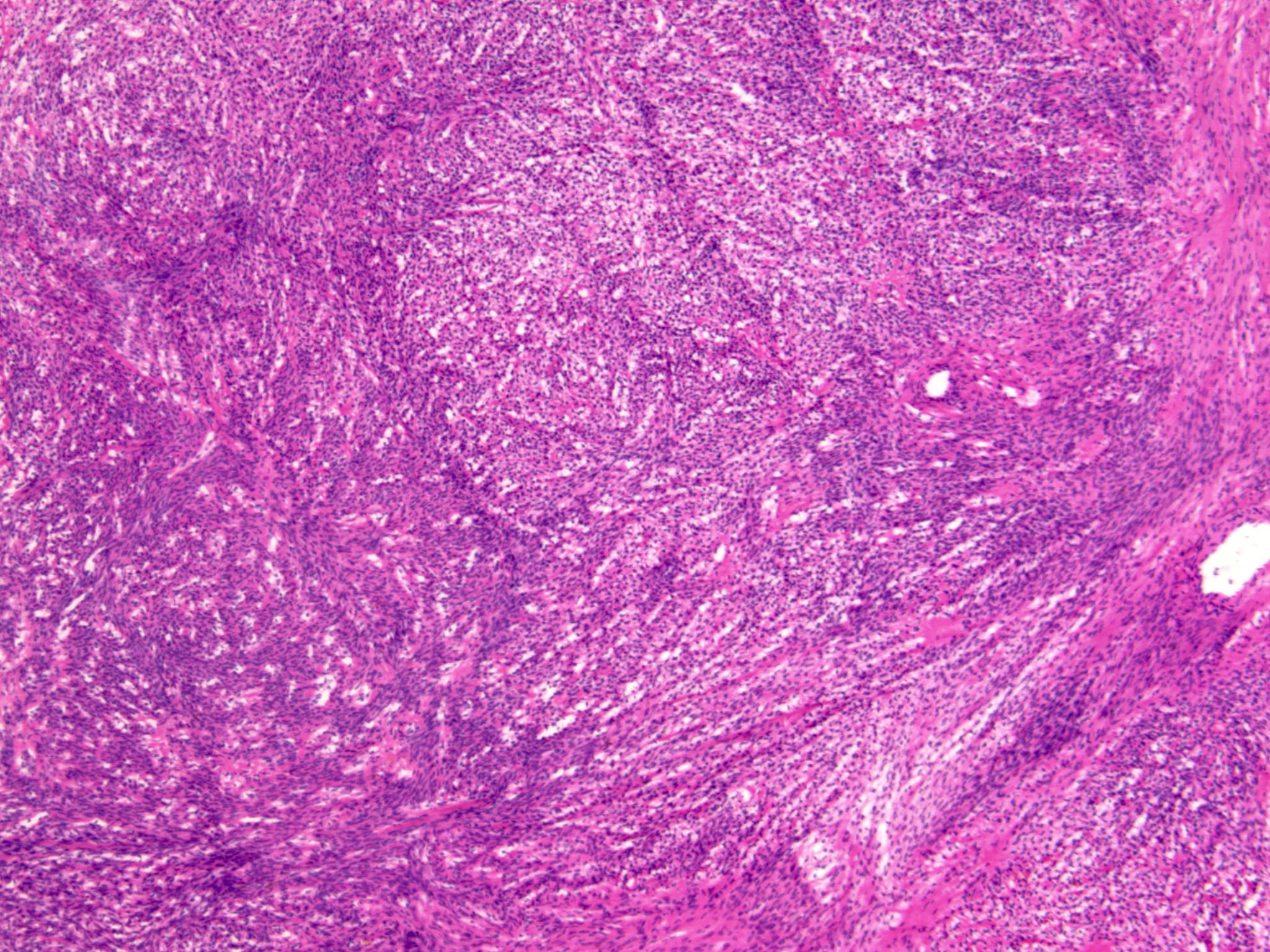
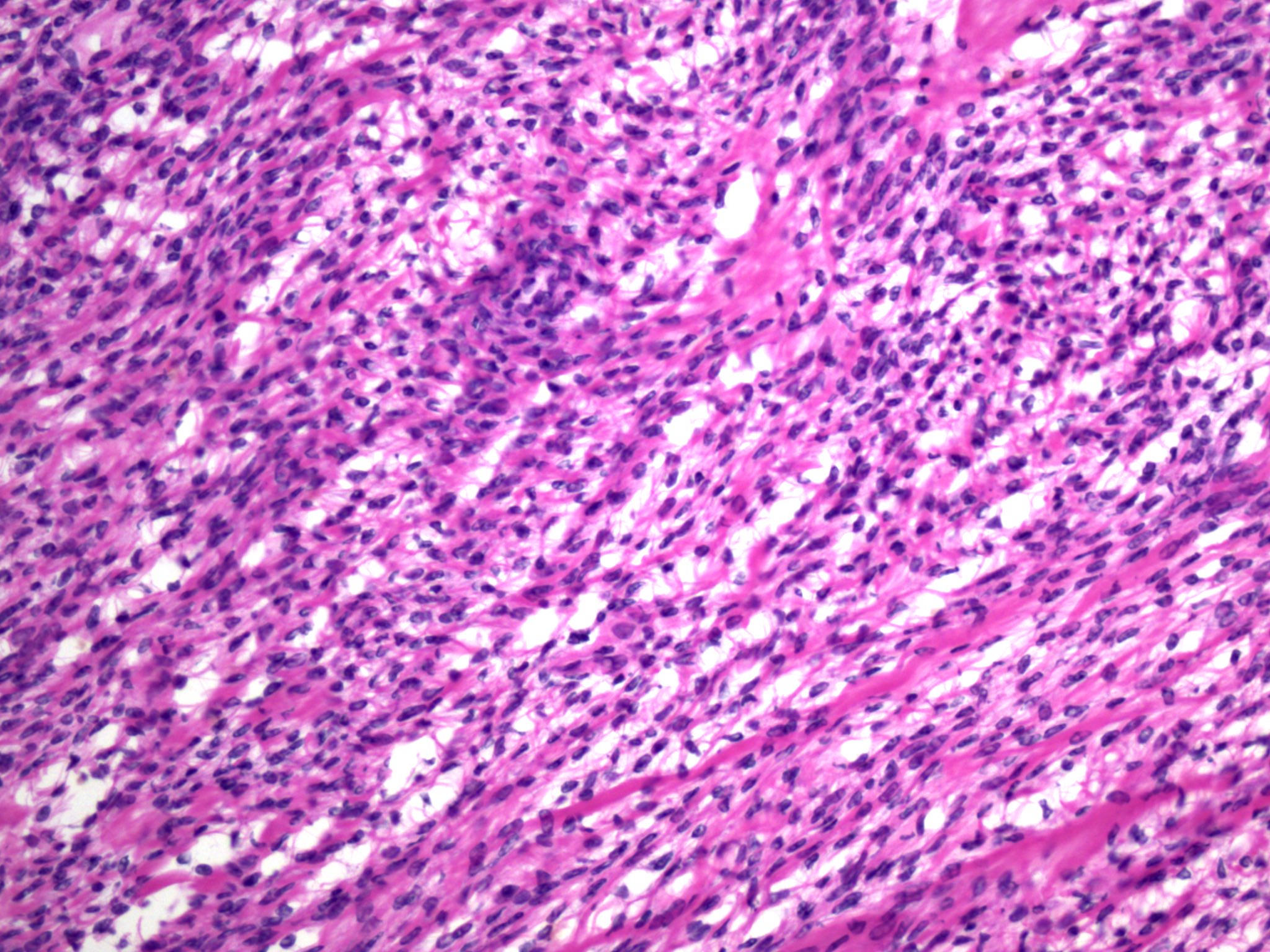
Microscopic (histologic) images
Contributed by Gulisa Turashvili, M.D., Ph.D., Kyle C. Strickland, M.D., Ph.D. and Rex Bentley, M.D.
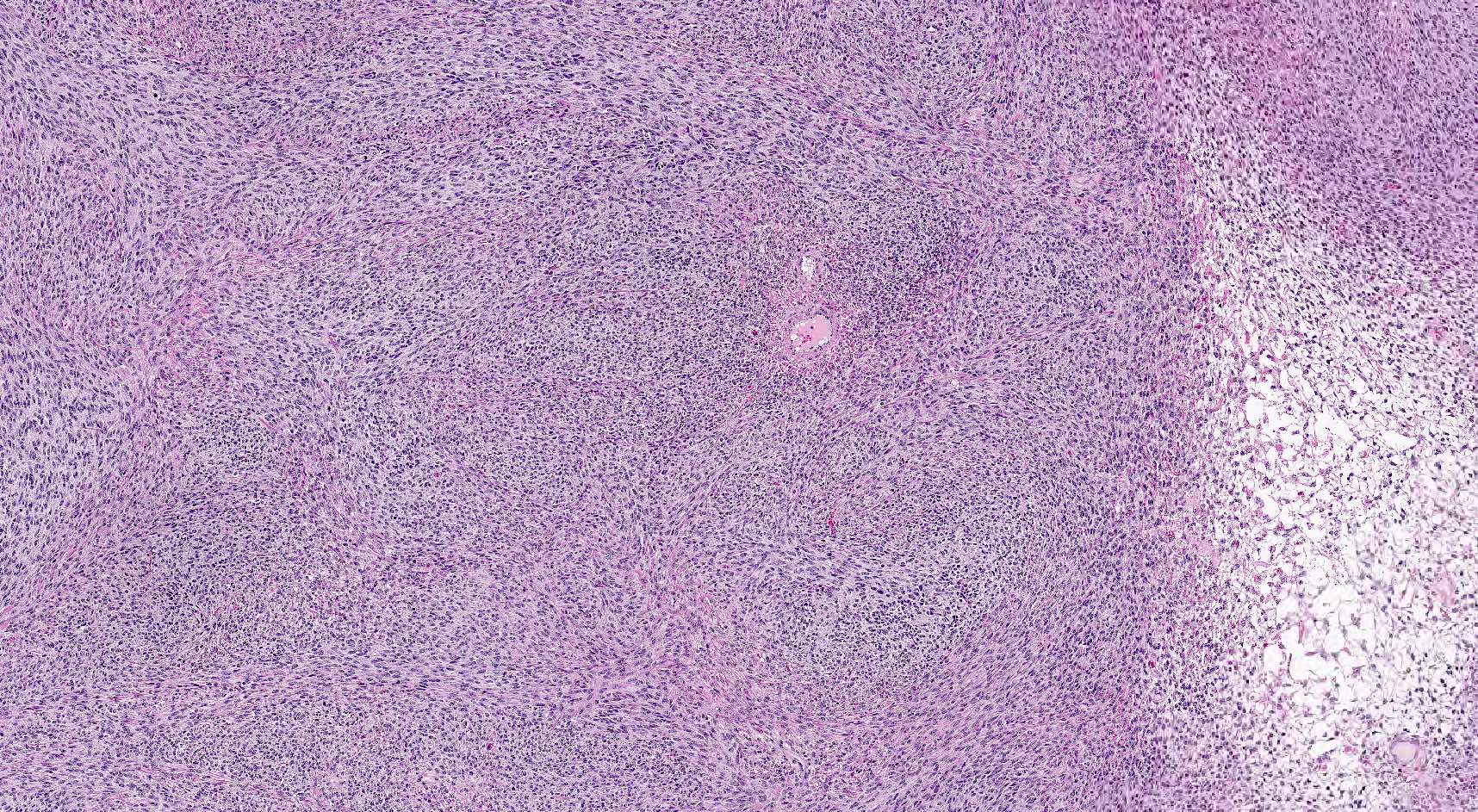
Cellular spindle cell neoplasm
Mild cytologic atypia
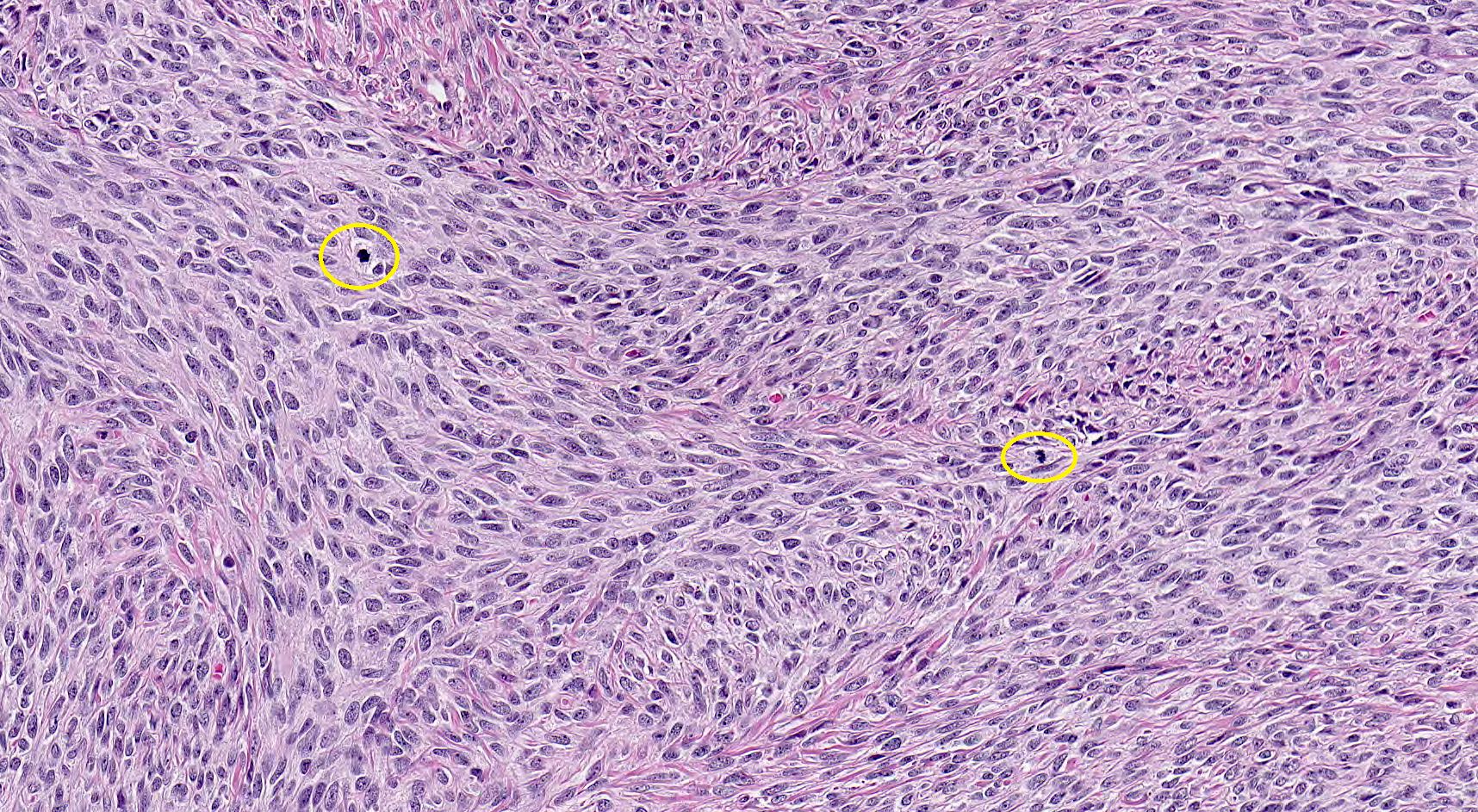
Mitotic activity
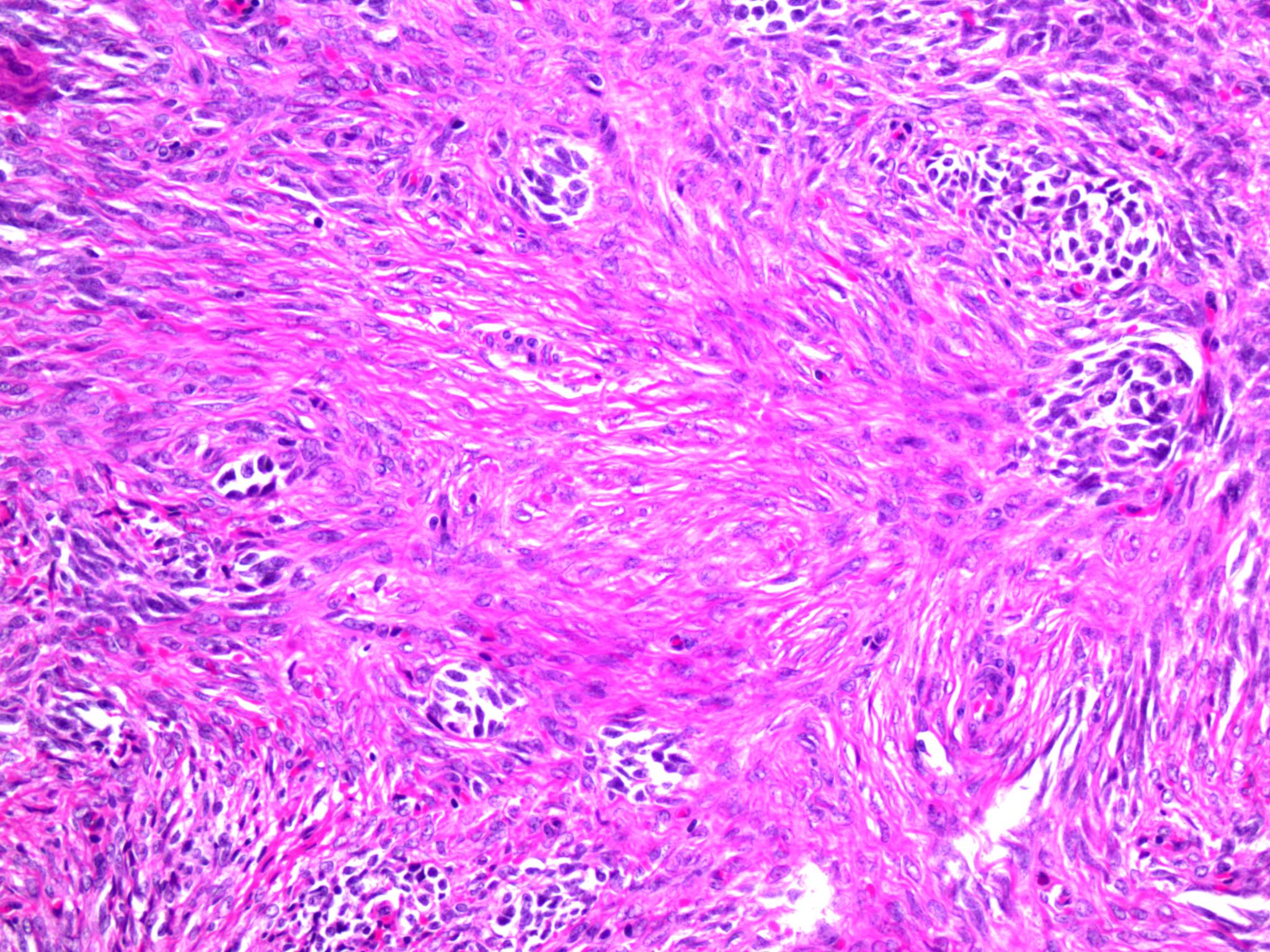
Small tubules
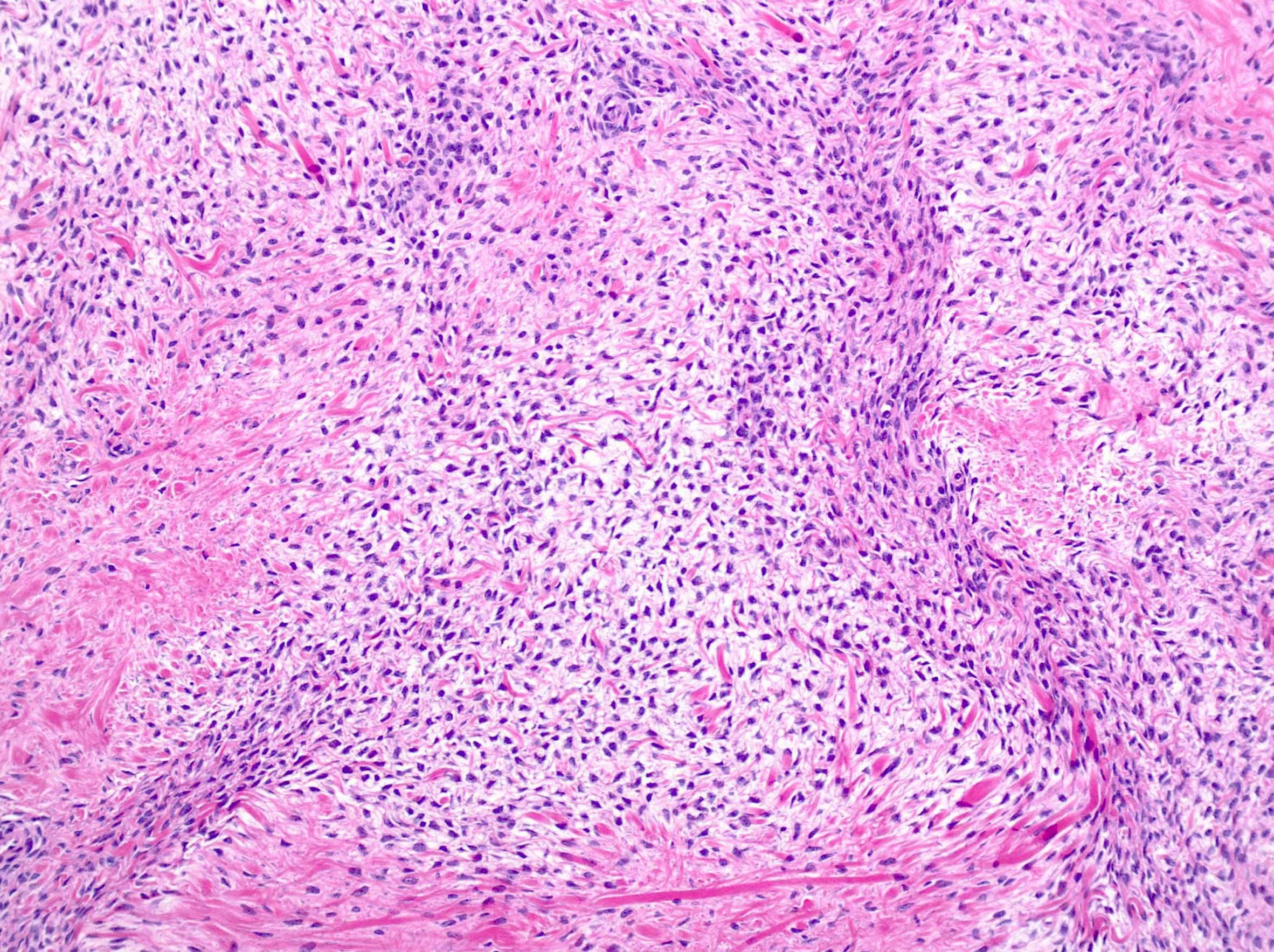
Variable cellularity
Bland spindle cells
Spindled to ovoid nuclei
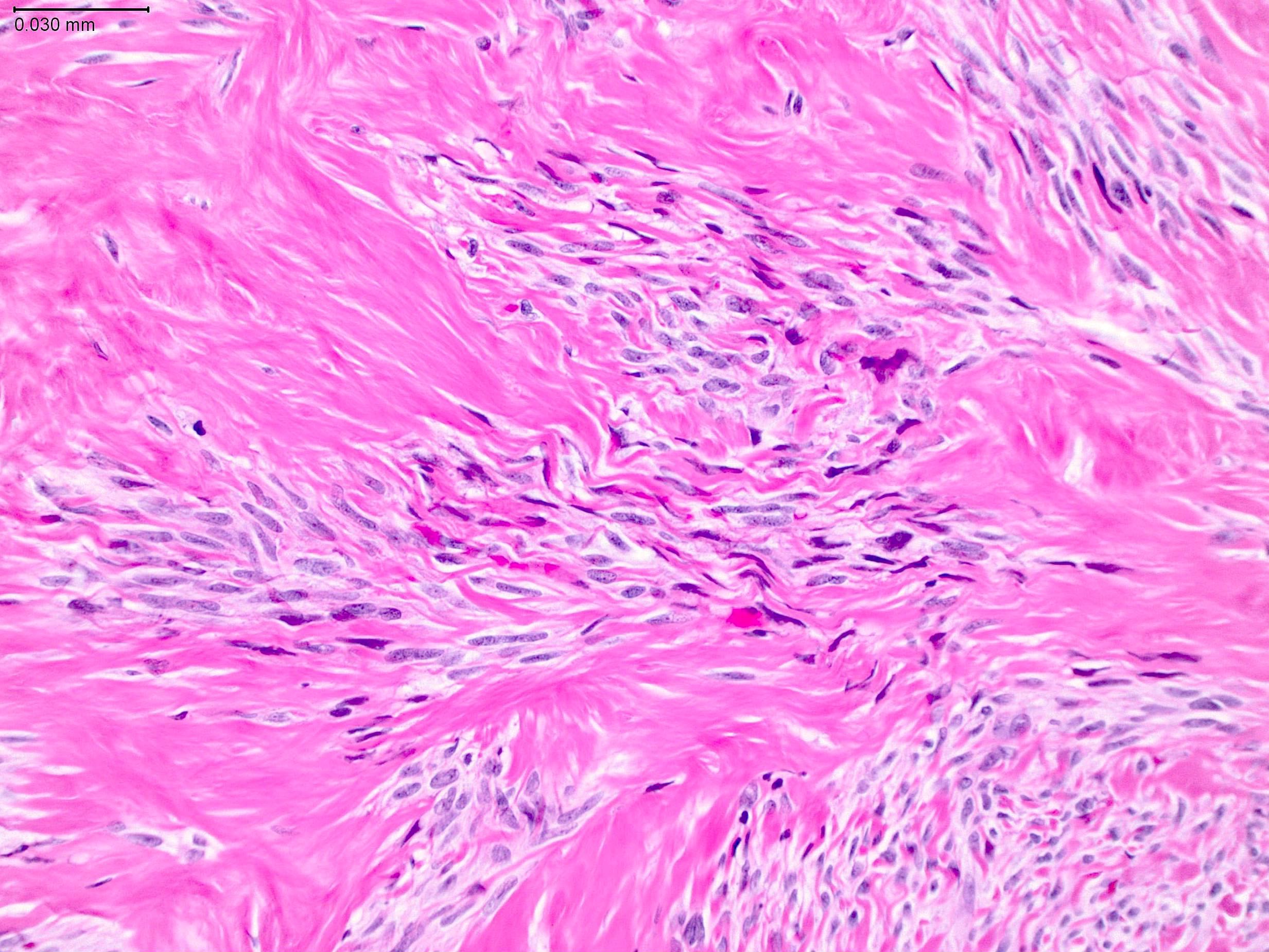
Dense collagen
Cellular spindle cell neoplasm
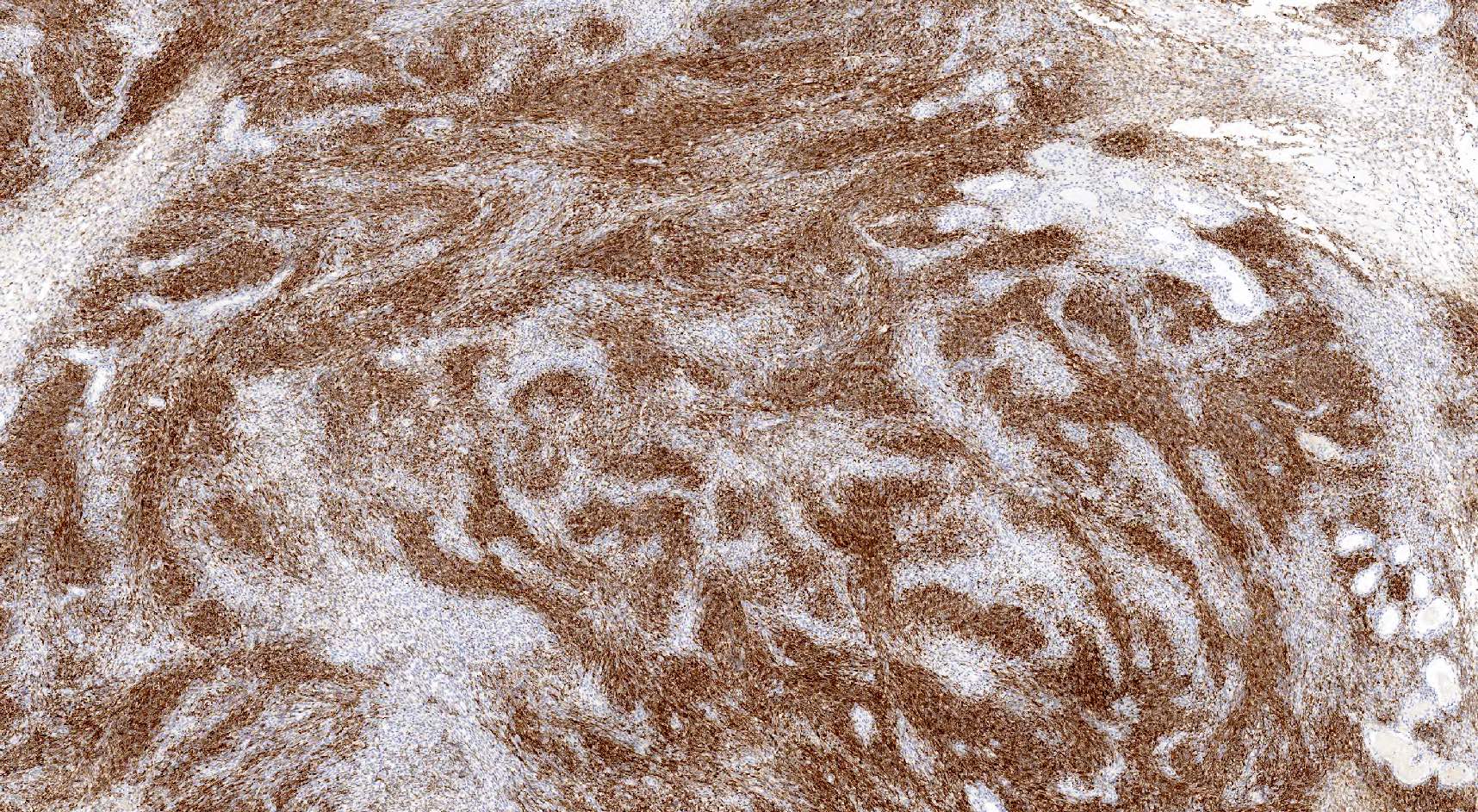
Reticulin
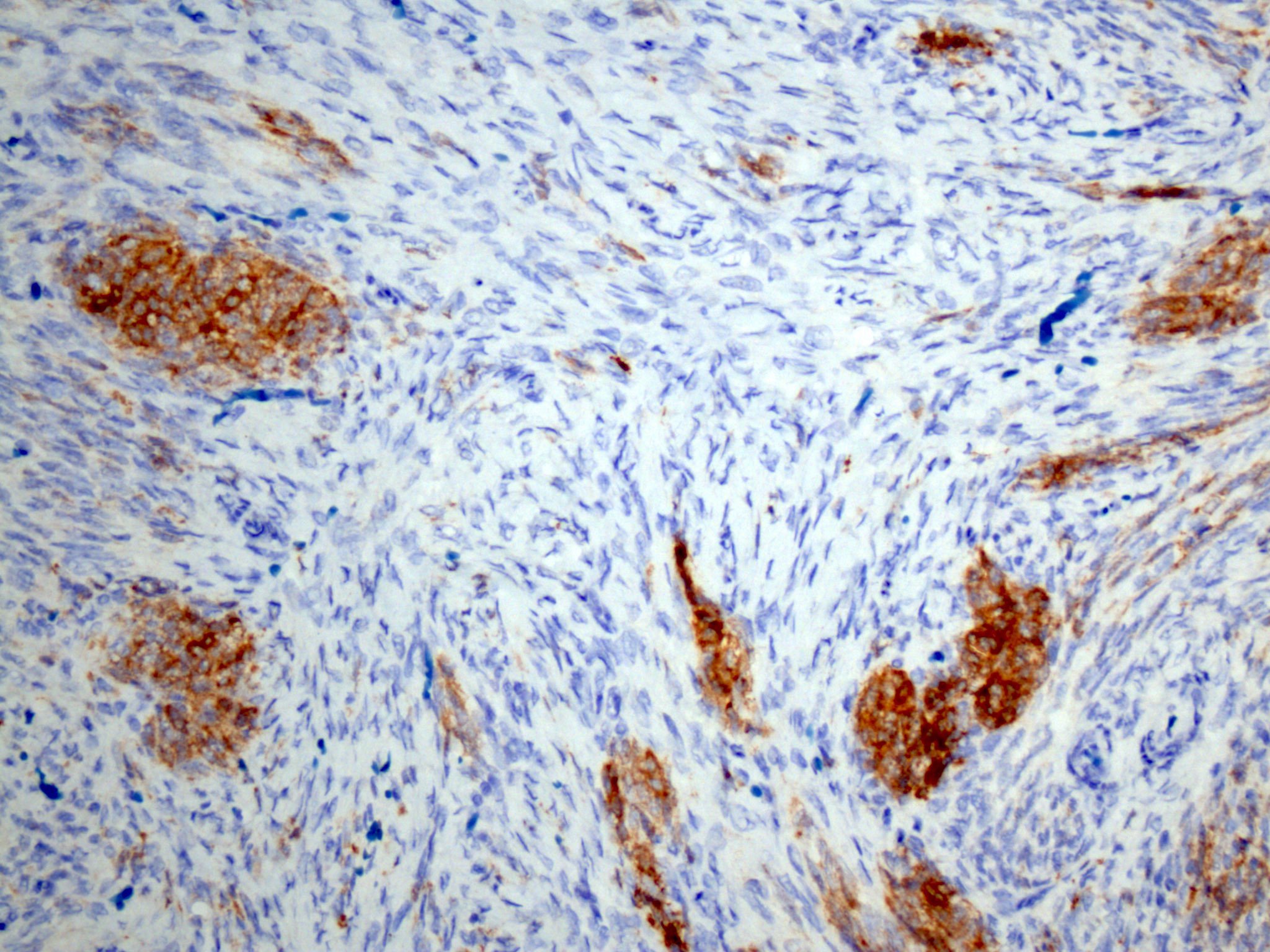
Inhibin
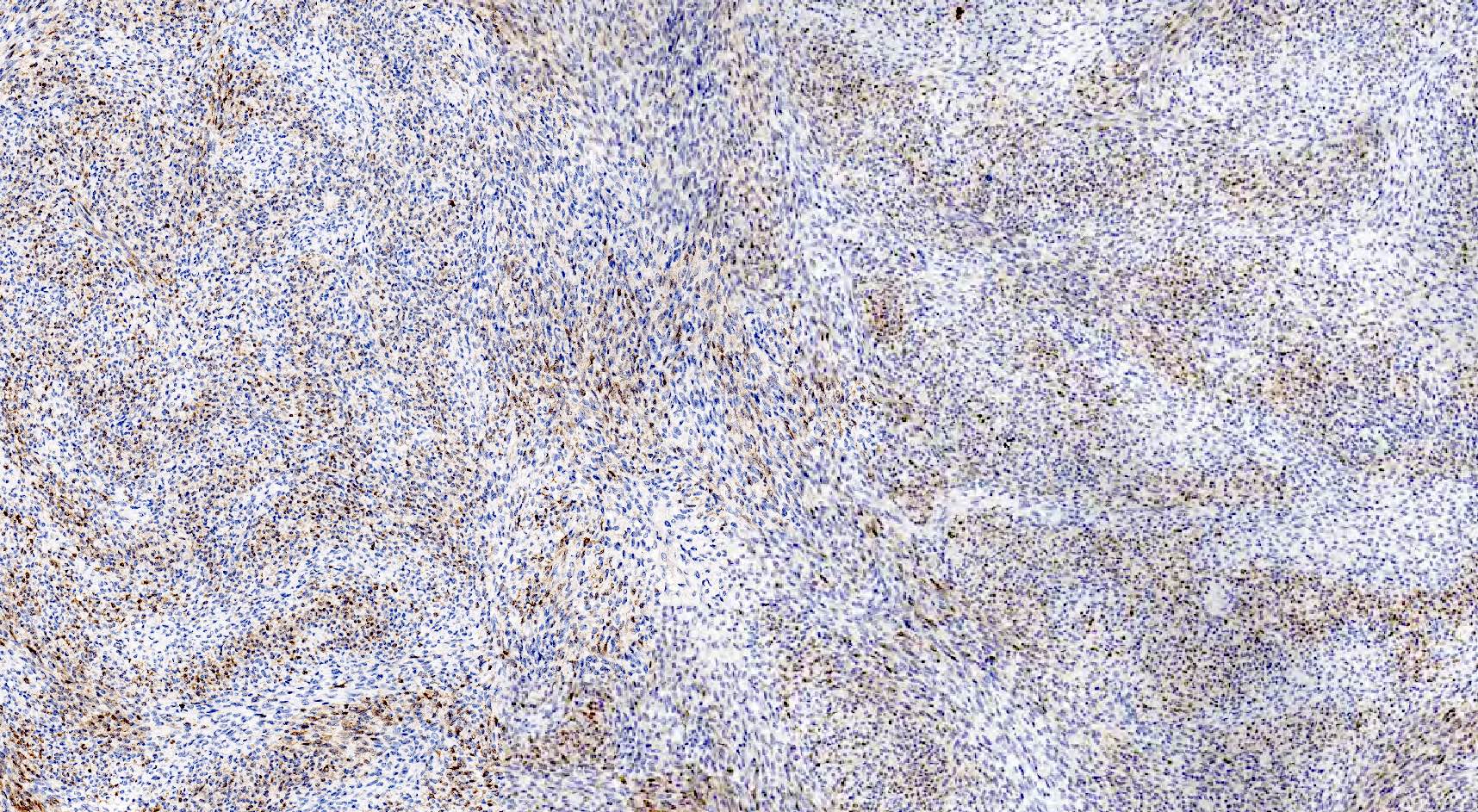
Calretinin
Virtual slides
Images hosted on other servers:

Fibroma (conventional)

Calretinin stain

Inhibin stain
Positive stains
- WT1 (Am J Surg Pathol 2008;32:884)
- SF1 (Am J Surg Pathol 2009;33:354)
- FOXL2 (Am J Surg Pathol 2011;35:484)
- Inhibin: 50% of cases, often focal or weak (Mod Pathol 1998;11:656, Mod Pathol 2003;16:584)
- Vimentin (J Pathol 1987;152:253)
- CD56 (Am J Surg Pathol 2008;32:884)
- ER beta
- PR
- SMA (Am J Surg Pathol 2008;32:884)
- Reticulin: differentiates fibroma (individual pericellular reticulin staining pattern) from diffuse type of adult granulosa cell tumor (nested reticulin staining pattern)
Negative stains
- CD10 (Int J Gynecol Pathol 2007;26:359)
- Desmin
- Caldesmon
- CD99 (Am J Surg Pathol 2009;33:354)
- Calretinin: positive in 25% of cases, often focal or weak (Am J Surg Pathol 2009;33:354, Am J Surg Pathol 2011;35:484)
- S100 and CD34: occasionally positive (Am J Surg Pathol 2008;32:884)
Electron microscopy description
- Numerous thin, elongated cells with intercommunicating cytoplasmic processes admixed with abundant collagen fibrils (Cancer 1971;27:438)
- Fibrils appear grouped in bundles with a crossbanding pattern composed of a light band bound by two thin dark bands (recurring at intervals of 600 Å)
- Cells have indistinct cell borders and are compressed by collagenous stroma
- Elongated and thin nuclei with marked peripheral heterochromatin condensation
- Scant cytoplasm containing few mitochondria and scant endoplasmic reticulum
Molecular / cytogenetics description
- Trisomy or tetrasomy 12 (Ann Pathol 2001;21:393, Genes Chromosomes Cancer 1990;2:48, Gynecol Oncol 1990;38:28)
- Rarely, IDH1 mutations (Histopathology 2013;62:667)
- Loss of heterozygosity at 9q22.3 (PTCH1) and 19p13.3 (STK11) in cellular fibromas (Hum Pathol 2005;36:792)
- No or rare FOXL2 mutations (Am J Surg Pathol 2013;37:1450, Int J Gynecol Pathol 2018;37:305)
Sample pathology report
- Right ovary and fallopian tube, salpingo-oophorectomy:
- Ovary: fibroma
- Fallopian tube: unremarkable
Differential diagnosis
- Diffuse adult granulosa cell tumor (GCT):
- Typically see the other patterns of granulosa cell tumor
- Diffusely positive for inhibin and calretinin
- Nested reticulin staining pattern (Int J Gynecol Pathol 2018;37:305)
- FOXL2 mutations (Am J Surg Pathol 2011;35:484, N Engl J Med 2009;360:2719)
- Thecoma:
- May present with estrogenic manifestations, including endometrial carcinoma
- Diffuse or rarely, lobulated or nested growth
- Uniform tumor cells with abundant pale gray cytoplasm and indistinct cell membranes imparting a syncytial appearance
- Ovoid to round nuclei, with or without nucleoli or nuclear grooves
- None to minimal mitotic activity
- With or without hyaline plaques, calcifications, adipose metaplasia, small clusters of steroid type cells with eosinophilic to clear cytoplasm (Am J Surg Pathol 2014;38:1023)
- Rarely, scattered pleomorphic bizarre nuclei due to degenerative changes (Int J Gynecol Pathol 1983;1:325, Am J Surg Pathol 2014;38:1023)
- Usually positive for inhibin, calretinin and other sex cord markers
- Sclerosing stromal tumor:
- Often occurs in women in their third to fourth decades
- Alternating cellular and paucicellular areas with prominent staghorn vasculature
- Pseudolobulation and biphasic population of cells (luteinized and spindled)
- Usually positive for inhibin and calretinin
- Leiomyoma:
- Endometrial stromal tumor, low grade:
- Typical features of low grade endometrial stromal neoplasia, including permeative growth and arteriole-like vessels
- Diffusely positive for CD10
- With or without characteristic gene fusions such as JAZF1-SUZ12 (Orphanet J Rare Dis 2016;11:15)
- Metastatic gastrointestinal stromal tumor:
- Ovarian stromal hyperplasia:
- Bilateral
- Diffuse or multinodular proliferation of stromal cells
- Lacking collagenous stroma and hyaline plaques
- Massive edema:
- Unilateral or bilateral
- No well defined mass
- Proliferation of stromal cells with marked intercellular edema
- Entrapment of preexisting ovarian structures (follicles, corpora lutea or albicantia)
- Fibromatosis:
- Unilateral or bilateral
- No well defined mass
- Proliferation of stromal cells with abundant dense collagen
- Entrapment of preexisting ovarian structures
- Fibrosarcoma:
- Exceptionally rare and no longer considered a distinct WHO entity
- Hypercellular, composed of disorderly fascicles of spindle cells with scant cytoplasm and moderate to marked nuclear atypia, elevated mitotic activity including atypical forms (Cancer 1981;47:2663)
- Presence of ≥ 4 mitoses per 10 high power fields is not sufficient to diagnose fibrosarcoma in the absence of significant cytologic atypia (Am J Surg Pathol 2006;30:929)
- With or without necrosis and hemorrhage
- Focally positive for calretinin or inhibin, negative for CD10 (Am J Surg Pathol 2002;26:1477, Int J Gynecol Pathol 2007;26:359)
Additional references
Practice question #1
Microscopic examination of an 8 cm unilateral ovarian mass demonstrates a densely cellular neoplasm composed of intersecting fascicles of spindle cells with mild cytologic atypia and approximately 9 mitotic figures per 10 high power fields. Reticulin staining shows pericellular staining pattern and molecular testing is negative for FOXL2 mutation.
What is the most likely diagnosis?
- Fibroma
- Fibrosarcoma
- Leiomyoma
- Leiomyosarcoma
- Mitotically active cellular fibroma
Practice answer #1
Practice question #2
You receive an intraoperative consultation for bilateral multinodular ovarian masses in a 16 year old patient. Microscopic examination demonstrates bland, monomorphic spindled cells within a collagenous stroma.
Mutation of which of the following genes is most likely associated with this entity?
Mutation of which of the following genes is most likely associated with this entity?
- FOXL2
- HMGA2
- JAZF1
- PTCH
- Vimentin
Practice answer #2
D. PTCH. Bilateral ovarian fibroma in a young patient is most likely associated with Gorlin syndrome.
Comment Here
Reference: Fibroma
Comment Here
Reference: Fibroma
