

Cervix
Adenocarcinoma
Clear cell carcinoma
Editorial Board Member: David B. Chapel, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 8 April 2024
Last staff update: 8 April 2024
Copyright: 2018-2024, PathologyOutlines.com, Inc.
PubMed Search: Clear cell carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Agarwal AN, Valente PT. Clear cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixclearcell.html. Accessed April 26th, 2024.
Definition / general
- Malignant glandular neoplasm composed of clear or eosinophilic cells with varying architectural patterns, including solid, tubulocystic or papillary
- Accounts for ~3 - 4% of adenocarcinoma of the cervix
- HPV independent
Essential features
- Multiple architectural patterns with hyalinized stroma and hobnail cells
- Cytoplasm may be clear, eosinophilic or granular and may contain intracytoplasmic hyaline globules
- High nuclear grade, at least focally, contrasting with relatively low mitotic count and mildly increased Ki67
- HNF1β and napsin A positive; ER, PR and p16 negative; normal p53 expression in most cases (Int J Gynecol Pathol 2018;37:388, Am J Surg Pathol 2011;35:633)
- Women with history of in utero exposure to diethylstilbestrol (DES) are at higher risk for developing clear cell adenocarcinoma of the vagina and cervix (Cancer Causes Control 2022;33:1121)
Terminology
- Not preferred: mesonephroid carcinoma
ICD coding
- ICD-O: 8310/3 - clear cell adenocarcinoma, NOS
- ICD-10: C53.0 - malignant neoplasm of endocervix
- ICD-11: 2C77.1 & XH6L02 - adenocarcinoma of cervix uteri & clear cell adenocarcinoma, NOS
Epidemiology
- Accounts for 3 - 4% of adenocarcinoma of cervix
- Bimodal age distribution (J Midlife Health 2015;6:85)
- First peak occurs in women aged 17 - 37 years
- Second peak occurs in women aged 44 - 88 years
- Median age of diethylstilbestrol (DES) related clear cell carcinoma is 19 years, while median age of sporadic (non-DES associated) clear cell carcinoma is 51 years (Gynecol Oncol 2000;76:147)
- Majority of cervical clear cell carcinoma (~60%) is associated with in utero exposure to diethylstilbestrol (DES) (JAAPA 2017;30:49)
Pathophysiology
- Historically associated with intrauterine DES exposure; use declined after U.S. FDA warning in 1971 (NCI: Diethylstilbestrol (DES) Exposure and Cancer [Accessed 16 February 2023])
- Cervical endometriosis might contribute to the occurrence of clear cell carcinoma of the cervix in women without DES exposure (Br J Radiol 2009;82:e20, Int J Gynecol Pathol 2018;37:88)
- Observation of tuboendometrioid metaplasia adjacent to clear cell carcinoma lesions suggests it as a potential precursor lesion (Int J Gynecol Pathol 2022;41:105)
- Not related to high risk HPV infection (Int J Gynecol Cancer 2013;23:1084)
- Clear cell carcinoma in situ may be a precursor lesion to invasive clear cell carcinoma of the cervix (Int J Gynecol Pathol 2023;42:217)
Clinical features
- Abnormal uterine bleeding
- Abdominal pain
- Postcoital bleeding
- Abnormal vaginal discharge
- Physical examination shows polypoid / exophytic lesion, barrel shaped cervix or normal appearing cervix
- Rarely pelvic mass
- Abnormal pap smear
- Reference: Onco Targets Ther 2014;7:111
Diagnosis
- Can be made on a biopsy with classic morphologic patterns, which can be supported by napsin A immunohistochemical stain positivity
Prognostic factors
- Traditional prognostic factors include the following (Gynecol Oncol 2008;109:335)
- FIGO stage, in particular related to
- Lymph node status
- Parametrial involvement
- > One - third cervical stromal involvement
- Positive surgical margins
- Tumor diameter > 4 cm
- Lymph vascular space involvement
- FIGO stage, in particular related to
- DES independent cervical clear cell carcinoma does not seem to have a worse prognosis than squamous cell carcinoma of the cervix, when matched for stage (Gynecol Oncol 2000;76:331, Onco Targets Ther 2014;7:111)
- However, a large study of ~25,000 patients indicated that adenocarcinoma histology negatively impacts survival for both early and advanced stage carcinomas (Gynecol Oncol 2012;125:287)
- Though not statistically significant, patients with DES independent clear cell carcinoma had a worse 5 year survival rate (67%) compared to squamous cell carcinoma (80%) and non-clear cell carcinoma (77%) (Gynecol Oncol 2000;76:331)
- Cervical clear cell carcinoma has similar overall survival and recurrence free survival to gastric type endocervical adenocarcinoma; it also has poorer outcomes than HPV associated endocervical adenocarcinoma (Am J Surg Pathol 2022;46:1317)
- Median time to recurrence is 12 months overall (Gynecol Oncol 2008;109:335, Gynecol Oncol 2000;76:147)
- Common sites of relapse include pelvis, para-aortic lymph nodes and distant sites (Int J Gynecol Cancer 2014;24:S90)
- 3 year overall survival: 91% stage I and II versus 22% advanced stage (Gynecol Oncol 2008;109:335)
- 5 year progression free survival: 85% stage I - IIA and 42% stage IIB - IV
- 5 year overall survival: 90% stage I - IIA and 63% stage IIB - IV (Gynecol Oncol 2008;109:335)
- Lymph node status is a strong predictor of overall survival (80%) and progression free survival (31%) (Gynecol Oncol 2008;109:335, Gynecol Oncol 2000;76:331)
Case reports
- 12 year old girl with vaginal bleeding and no prior exposure of diethylstilbestrol with clear cell carcinoma of cervix (Sichuan Da Xue Xue Bao Yi Xue Ban 2021;52:534)
- 26 year old woman with cesarean radical hysterectomy in a triplet pregnancy complicated by clear cell carcinoma of the cervix (Int J Gynecol Cancer 2012;22:1198)
- 47 year old woman with synchronous invasive squamous cell carcinoma and clear cell carcinoma of the uterine cervix (Gynecol Oncol 2005;97:976)
- 52 year old woman with obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome with uterine didelphys and clear cell carcinoma of the cervix (World J Oncol 2021;12:34)
- 52 year old woman with clear cell carcinoma of the cervix exhibiting choriocarcinomatous differentiation and mismatch repair protein abnormality (Int J Gynecol Pathol 2017;36:323)
- 56 year old woman with clear cell carcinoma of the uterine cervix and cervical endometriosis (Int J Gynecol Pathol 2018;37:88)
Treatment
- Due to rarity of the tumor, treatment guidelines are based on common cervical cancers (e.g., squamous cell carcinoma)
- Early stage (IA, IB1 and selected IIA1): surgery or radiation therapy or concurrent chemoradiation (NCCN: Clinical Practice Guidelines in Oncology - Cervical Cancer, Version 3.2019 [Accessed 17 February 2023])
- Surgery
- Fertility sparing: cone biopsy or radical trachelectomy with or without pelvic lymph node dissection
- Nonfertility sparing: simple or radical hysterectomy with sentinel lymph node mapping / pelvic lymph node dissection + para-aortic lymph node dissection
- Radiation therapy (RT): pelvic beam external beam RT (EBRT) with brachytherapy
- Surgery
- Advanced disease (IB2, II, III and IVA): platinum containing chemotherapy and EBRT
Clinical images
Images hosted on other servers:

Vascularized, indurated lesion
Gross description
- In non-DES exposure cases, the tumor arises in ectocervix or endocervix
- In DES exposure cases, the tumor most commonly arises in the ectocervix
- Tumor median size is 3.4 cm (Obstet Gynecol Int 2019;2019:9465375)
- Variable presentation: exophytic mass, barrel shaped cervix or normal appearing cervix (Onco Targets Ther 2014;7:111)
Gross images
Contributed by Philip T. Valente, M.D.

Tan-white lesion
Images hosted on other servers:

Exophytic mass on the posterior lip of cervix

Didelphys uterus with a cervical mass
Frozen section description
- Variable mix of patterns: tubulocystic, papillary and solid forms seen with clear to eosinophilic cytoplasm
Frozen section images
Contributed by Apeksha N. Agarwal, M.B.B.S., M.D.

Tubulocystic pattern

Eosinophilic cytoplasm, high N:C ratio
Microscopic (histologic) description
- 3 major patterns
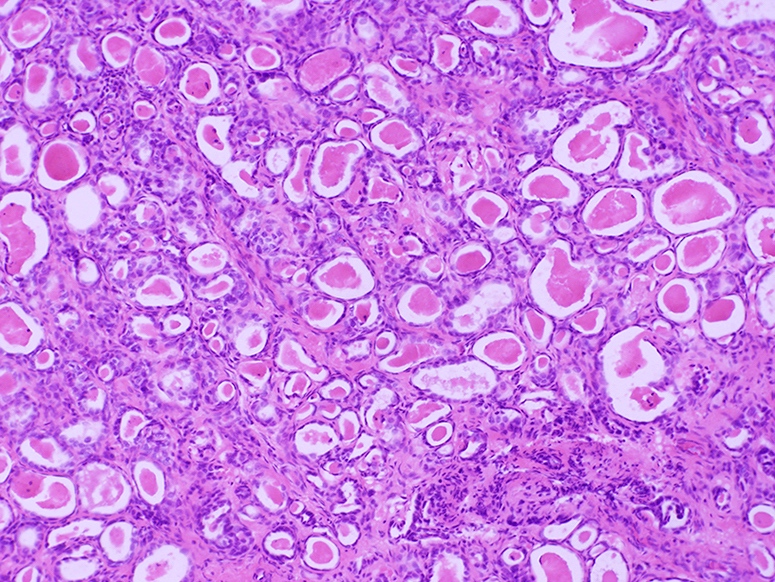
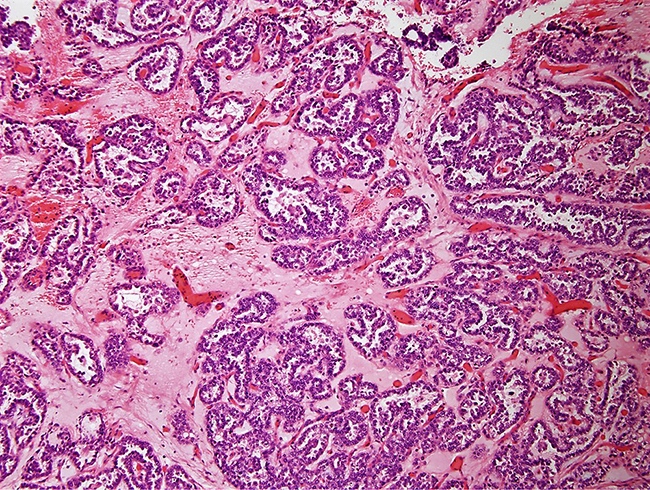
- Tubulocystic pattern (most common): tubules lined by a single layer of bland cells or prominent hyperchromatic nuclei project into the apical cytoplasm forming hobnail appearance
- Papillary pattern (least common): papillae with central hyaline fibrous tissue cores lined by hobnail cells with hyperchromatic nuclei
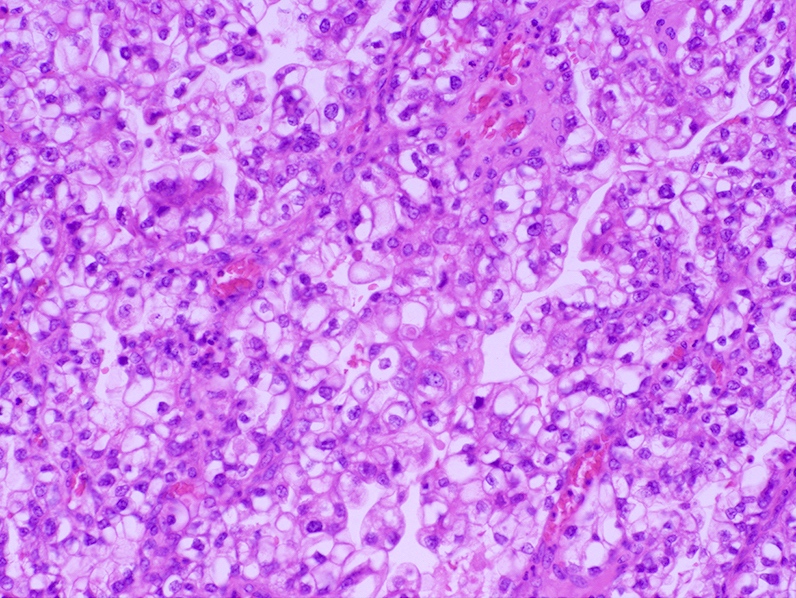
- Solid pattern: nests of cells with clear to pale eosinophilic cytoplasm, notable nuclear atypia, focal gland formation and variable sized cytoplasmic vacuoles, simulating signet ring cell differentiation; appears to be more common in clear cell carcinoma of the cervix (Int J Gynecol Pathol 2018;37:388)
- Intracytoplasmic hyaline globules, especially in solid pattern
- Extensive stromal hyalinization may be present
- May be associated with abundant plasma cells and psammoma bodies
- Morphologic spectrum is comparable to that of endometrial and ovarian counterparts with few differences (Int J Gynecol Pathol 2018;37:388)
- Low mitotic index (0 - 5/10 high power fields) often encountered in cervical (85%) compared to endometrial and ovarian cases (72% and 50%, respectively)
- Necrosis or psammoma bodies are usually absent in endocervical cases (present in 38% and 6% in ovarian clear cell carcinoma and 59% and 5% endometrial clear cell carcinoma, respectively, without statistical significance)
Microscopic (histologic) images
Contributed by Nadia Hameed, M.D.
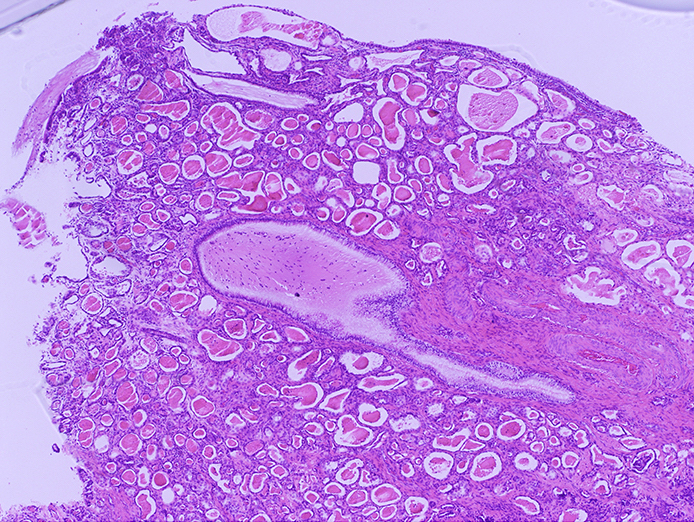
Tubulocystic pattern
Tubulocystic pattern
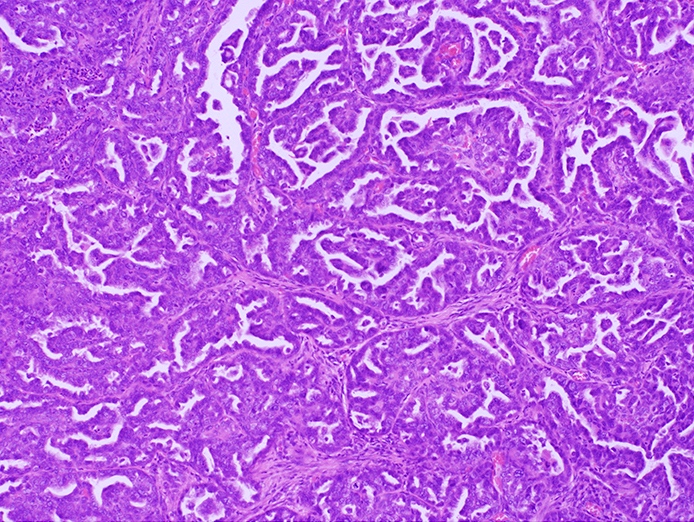
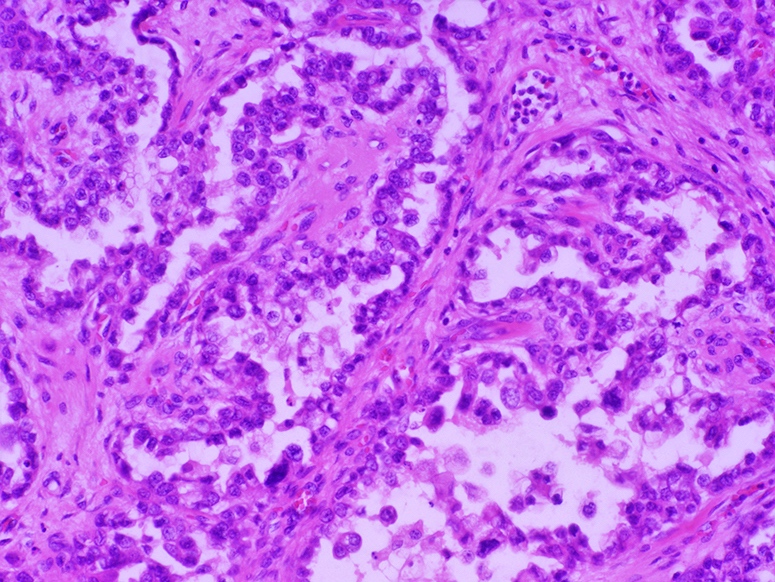
Papillary pattern
Papillary pattern
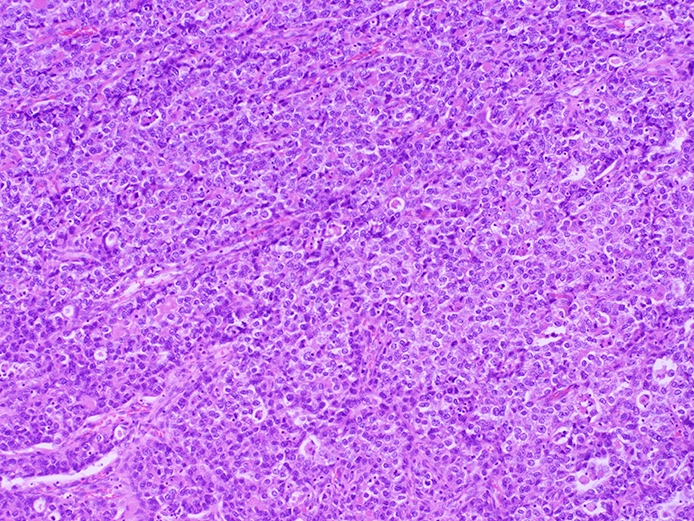
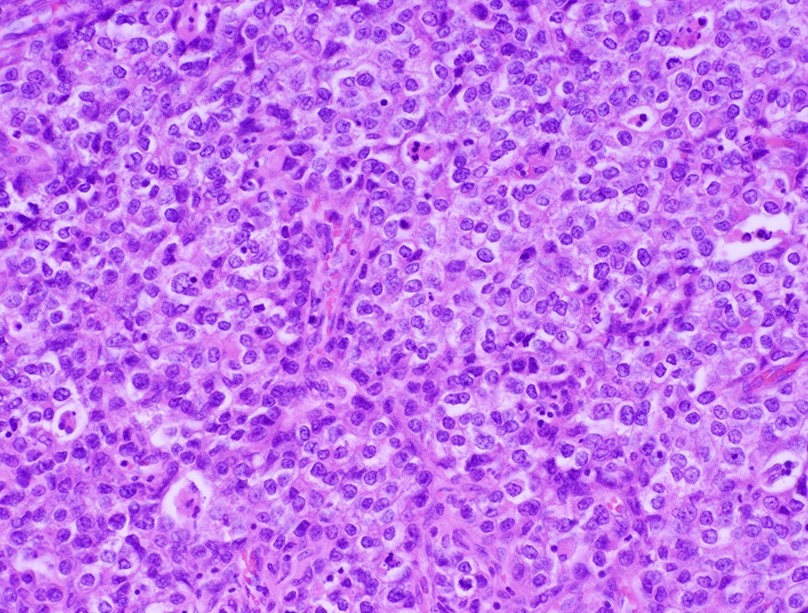
Solid pattern
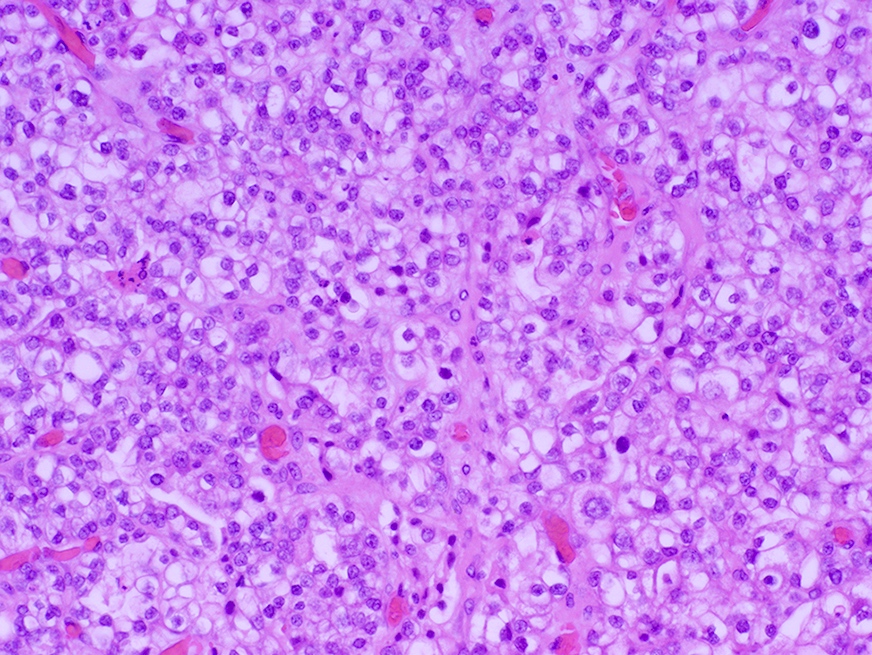
Solid pattern
Rare intracytoplasmic eosinophilic globules
Cytology description
- Pap test
- Cells arranged in sheets, clusters or papillae
- Cells have delicate, vacuolated, glycogen rich cytoplasm or finely granulated cytoplasm, naked nuclei and a tigroid background
- Nuclei are large, pale and round with prominent nucleoli
- Reference: Diagn Cytopathol 2020;48:804
Cytology images
Contributed by Nadia Hameed, M.D.
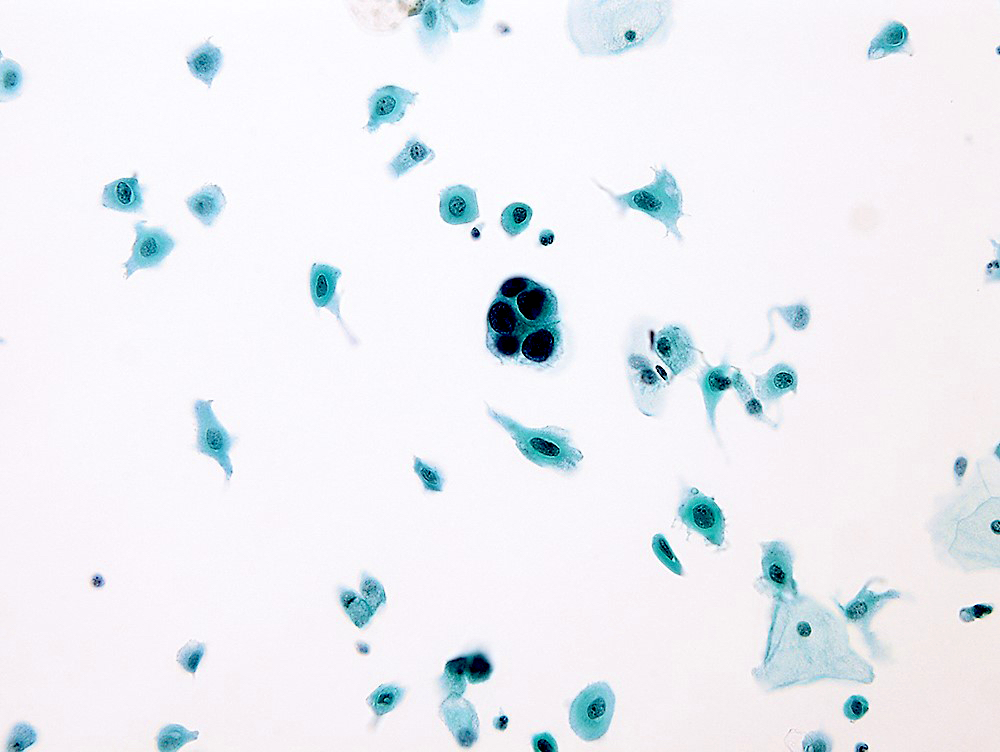
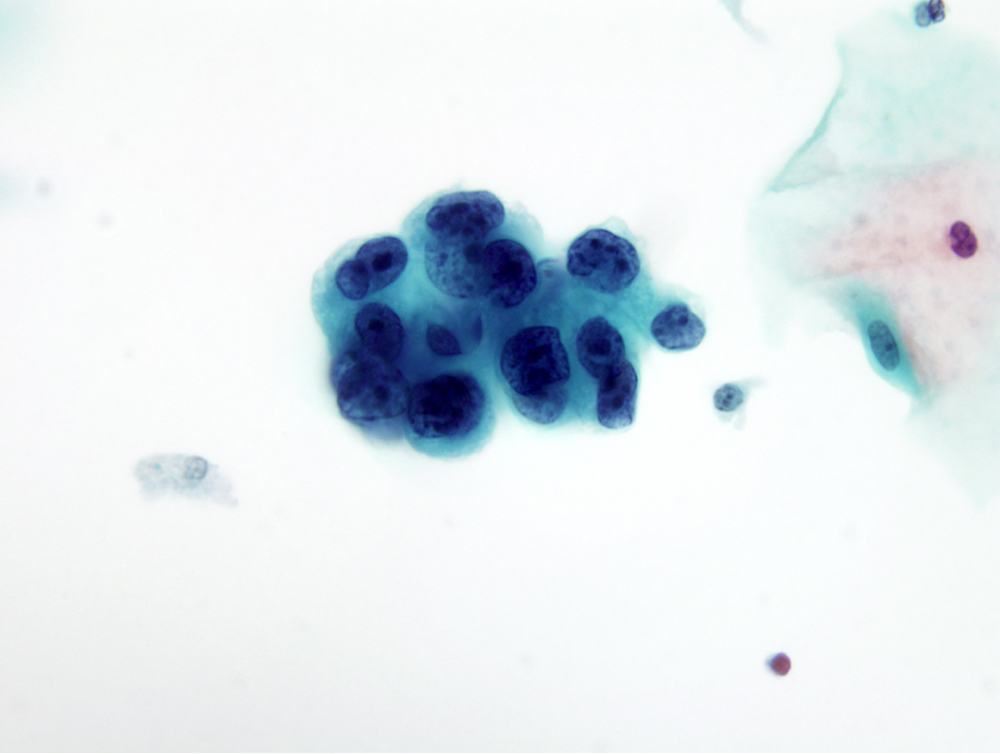
SurePath Pap test
Positive stains
- Pancytokeratin (AE1 / AE3, CAM5.2)
- CK7, CK8, CK18, CK19
- HNF1β (97%)
- Napsin A (74%)
- Racemase / AMACR (diffuse)
- p16 (focally positive in tumor cells)
- Ki67 index (~50%) (Int J Gynecol Pathol 2018;37:388)
- Epithelial membrane antigen (EMA)
- References: Technol Cancer Res Treat 2023;22:15330338221149297, Virchows Arch 2019;475:537, Int J Environ Res Public Health 2022;19:16652
Negative stains
- CK20
- High molecular weight CK 34 beta E12
- GATA3
- ER, PR (rarely focally expressed)
- Vimentin, SMA, desmin
- Chromogranin, synaptophysin, CD56, NSE
- CAIX
- CEA, unlike most other types of cervical adenocarcinoma
- p53 (14% have strong, diffuse mutant pattern staining) (Int J Gynecol Pathol 2018;37:388)
Electron microscopy description
- Continuous lamina densa, numerous mitochondria and rough endoplasmic reticulum, abundant glycogen and blunt microvilli
- Vesicular aggregates in nucleoplasm, perinuclear cytoplasm or between membranes of nuclear envelope (Acta Cytol 1976;20:262)
Electron microscopy images
Images hosted on other servers:

Mitochondria and rough endoplasmic reticulum
Molecular / cytogenetics description
- Rare case has been associated with Lynch syndrome (Int J Mol Sci 2018;19:979)
- Rare cases of clear cell carcinomas of endocervical origin may be associated with POLE mutation (Gynecol Oncol Rep 2019;28:15)
- Pathogenic genetic alterations in the Hippo signaling pathway (including recurrent somatic mutations in WWTR1 S89W) have been identified in patients with cervical clear cell carcinoma (J Pathol 2022;257:635)
Videos
Clear cell neoplasms of the gynecologic tract
Sample pathology report
- Cervix, 12:00, biopsy:
- Clear cell adenocarcinoma (see comment)
- Comment: Depth of invasion is at least 2 mm. Immunohistochemical stains for mismatch repair proteins show retained nuclear expression of MLH1, PMS2, MSH2 and MSH6.
Differential diagnosis
- Benign entities:
- Arias-Stella reaction:
- History of intrauterine or ectopic pregnancy, progestin treatment or gestational trophoblastic disease
- Hypersecretory glands; may be striking and produce a papillary or cribriform pattern
- Decidual change in stromal cells
- Focally enlarged, hyperchromatic nuclei that typically protrude into the gland lumen, giving the cell a hobnail appearance; nuclei may be smudged and have pseudoinclusions
- No / rare mitosis (low Ki67 index), no infiltration
- Microglandular hyperplasia:
- Small, markedly crowded glands lined by a single layer of bland cuboidal cells and usually associated with squamous metaplasia
- Has 2 distinct cell layers (luminal and basal / reserve cell); p63 highlights the basal / reserve layer or squamous metaplasia
- May present with sheets of clear cells
- Small bland nuclei and low mitotic activity should distinguish it from clear cell carcinoma
- Arias-Stella reaction:
- Malignant entities:
- Alveolar soft part sarcoma:
- Mesonephric adenocarcinoma:
- Develops deep in the lateral wall of the cervix (corresponding to the location of mesonephric duct remnants); invades the wall of the cervix
- Lacks clear cells and hobnails cells
- Does not display the admixture of tubulocystic, papillary and solid patterns
- Positive for CK7, EMA, CD10, calretinin and GATA3
- Metastatic clear cell renal cell carcinoma:
- Non-clear cell carcinomas of endometrial origin:
- May be difficult to differentiate on biopsy specimens
- Squamous cell carcinoma:
- Urothelial carcinoma:
Additional references
Board review style question #1
Which of the following statements regarding clear cell adenocarcinoma of the cervix is true?
- All cases are linked to perinatal exposure of diethylstilbestrol (DES)
- Histologically, there are cords of cells with abundant eosinophilic cytoplasm
- Immunohistochemical profile of this neoplasm includes positivity for CK7, AE1 / AE3, CAM 5.2, HNF1β and napsin A
- Median age of diagnosis is 5 years
Board review style answer #1
C. Immunohistochemical profile of this neoplasm includes positivity for CK7, AE1 / AE3, CAM 5.2, HNF1β and napsin A. Answer A is incorrect because not all cases are linked to DES exposure. Answer B is incorrect becauase cytoplasm in clear cell carcinoma of the cervix may be clear, eosinophilic or granular. Answer D is incorrect because the median age of diethylstilbestrol (DES) related clear cell carcinoma is 19 years and the median age of sporadic (non-DES associated) clear cell carcinoma is 51 years.
Comment Here
Reference: Cervix - Clear cell carcinoma
Comment Here
Reference: Cervix - Clear cell carcinoma
Board review style question #2
H&E of a cervical biopsy is shown above. What immunohistochemical markers should be included in the panel?
- CDX2, CA 19-9 and TTF1
- MelanA, GFAP and S100
- p63, napsin A and PAX8
- Synaptophysin, chromogranin and Ki67
Board review style answer #2
C. p63, napsin A and PAX8. Clear cell carcinoma of the cervix is negative for p63 and PAX8 while positive for napsin A. Answer B is incorrect because MelanA, GFAP and S100 are markers for melanoma and glial origin markers. Answer A is incorrect because it includes markers for gastrointestinal tract, pancreatic and lung origin markers. Answer D is incorrect because synaptophysin, chromogranin and Ki67 are neuroendocrine markers.
Comment Here
Reference: Cervix - Clear cell carcinoma
Comment Here
Reference: Cervix - Clear cell carcinoma
