Associated with t(6;9)(q22-23;p23-24) translocation creating a fusion gene between MYB proto-oncogene and NFIB transcription factor gene (Mod Pathol 2011;24:1169)
Overall, 56/68 (82%) of adenoid cystic carcinomas expressed MYB-NFIB fusion in a study by Brill et al.; of those 2/5 (40%) were from the larynx (Mod Pathol 2011;24:1169)
This chromosomal rearrangement juxtaposes super enhancers to the MYB locus to create a positive feedback loop elicited when the MYB protein activates these enhancers (Oncotarget 2016;7:66239)
Fusion between MYBL1 and NFIB genes without MYB aberration have been identified, demonstrating that tumor development may also be driven by genetic alterations in different members of the same transcription factor family (Oncotarget 2016;7:66239)
Specific risk factors have not yet been identified, smoking does not affect the incidence unlike squamous cell carcinomas (Acta Otorhinolaryngol Ital 2009;29:279)
May be associated with squamous cell carcinoma, particularly if supraglottic and either high grade or solid variants; these cases are extremely aggressive (Ann Thorac Surg 2004;78:1889)
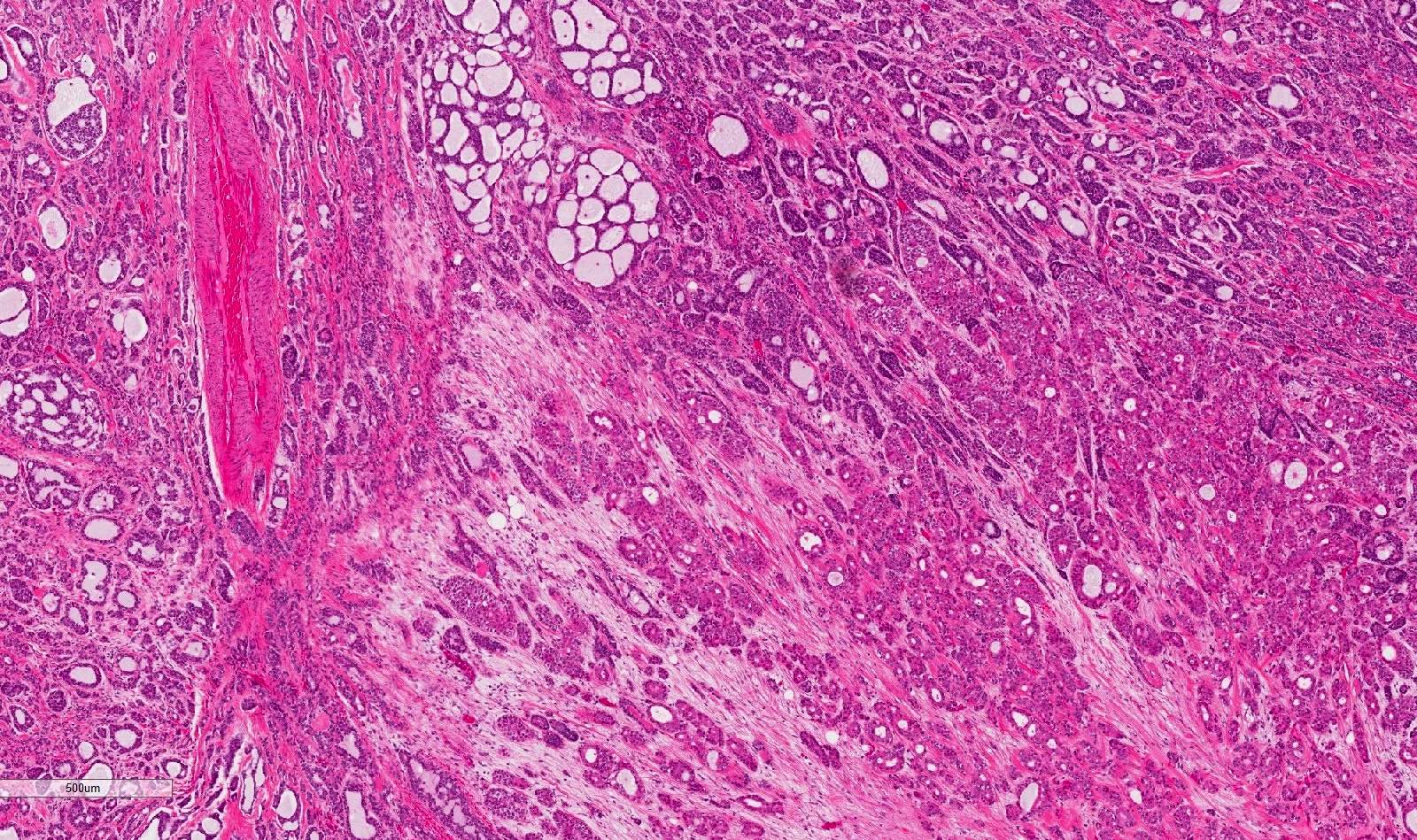
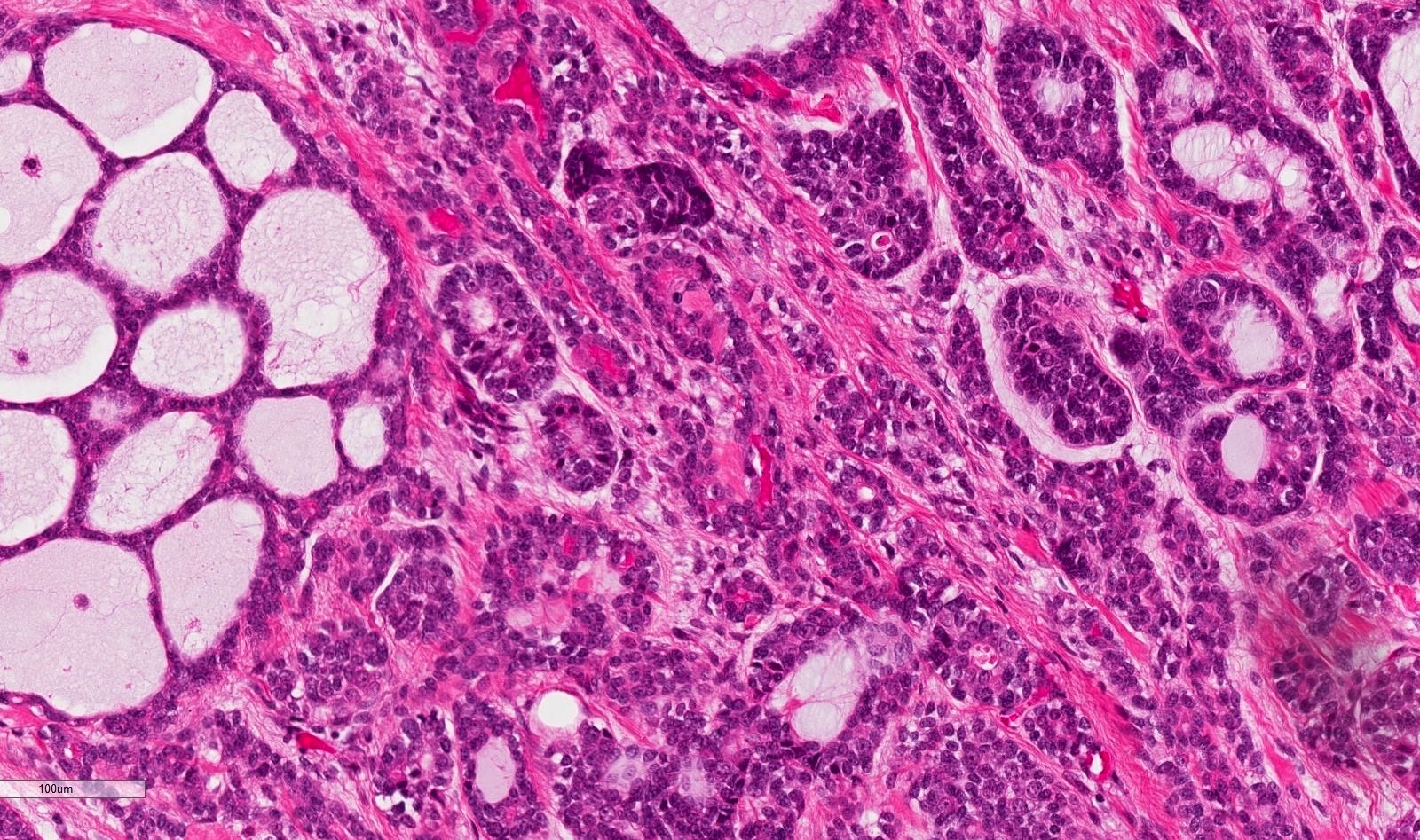
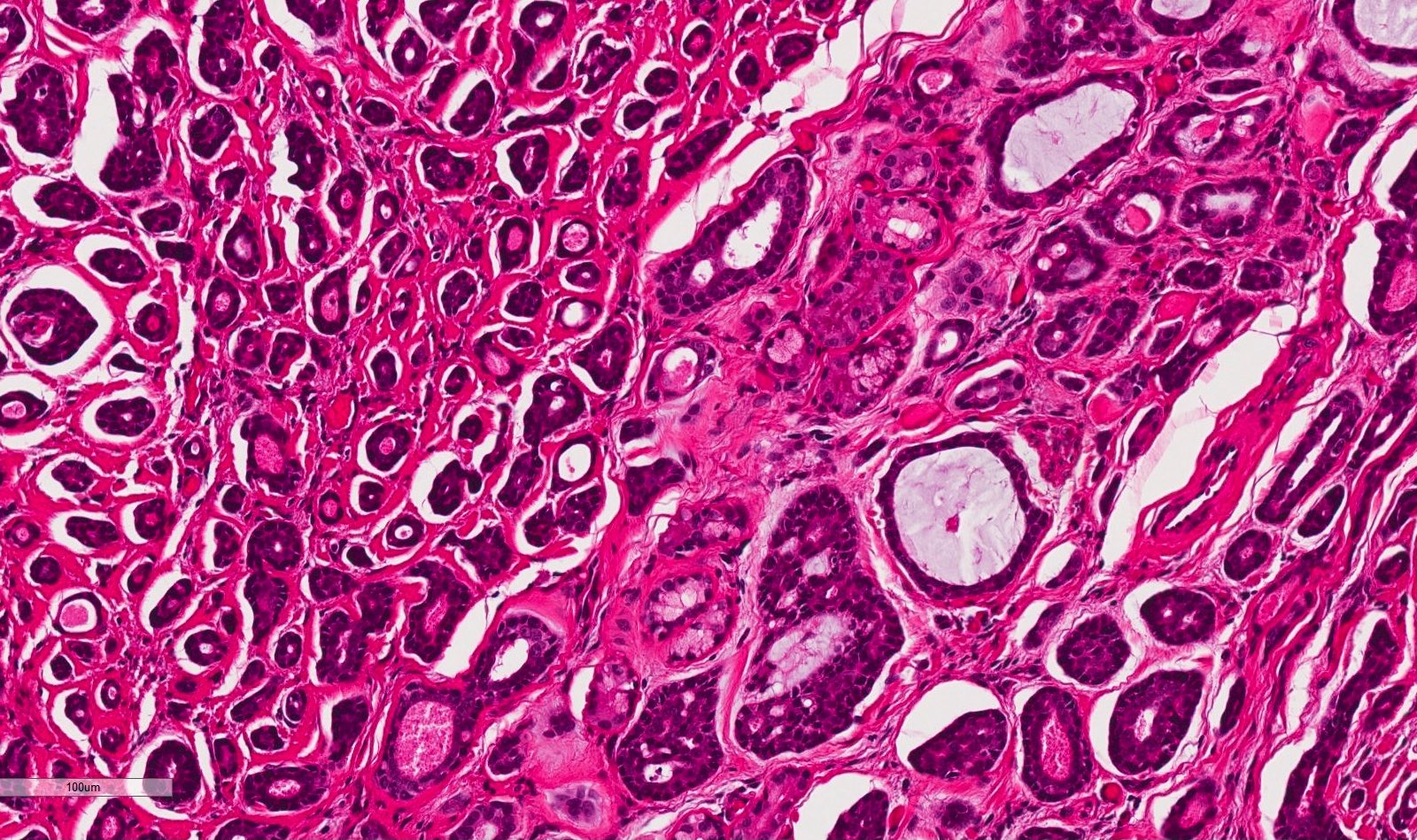
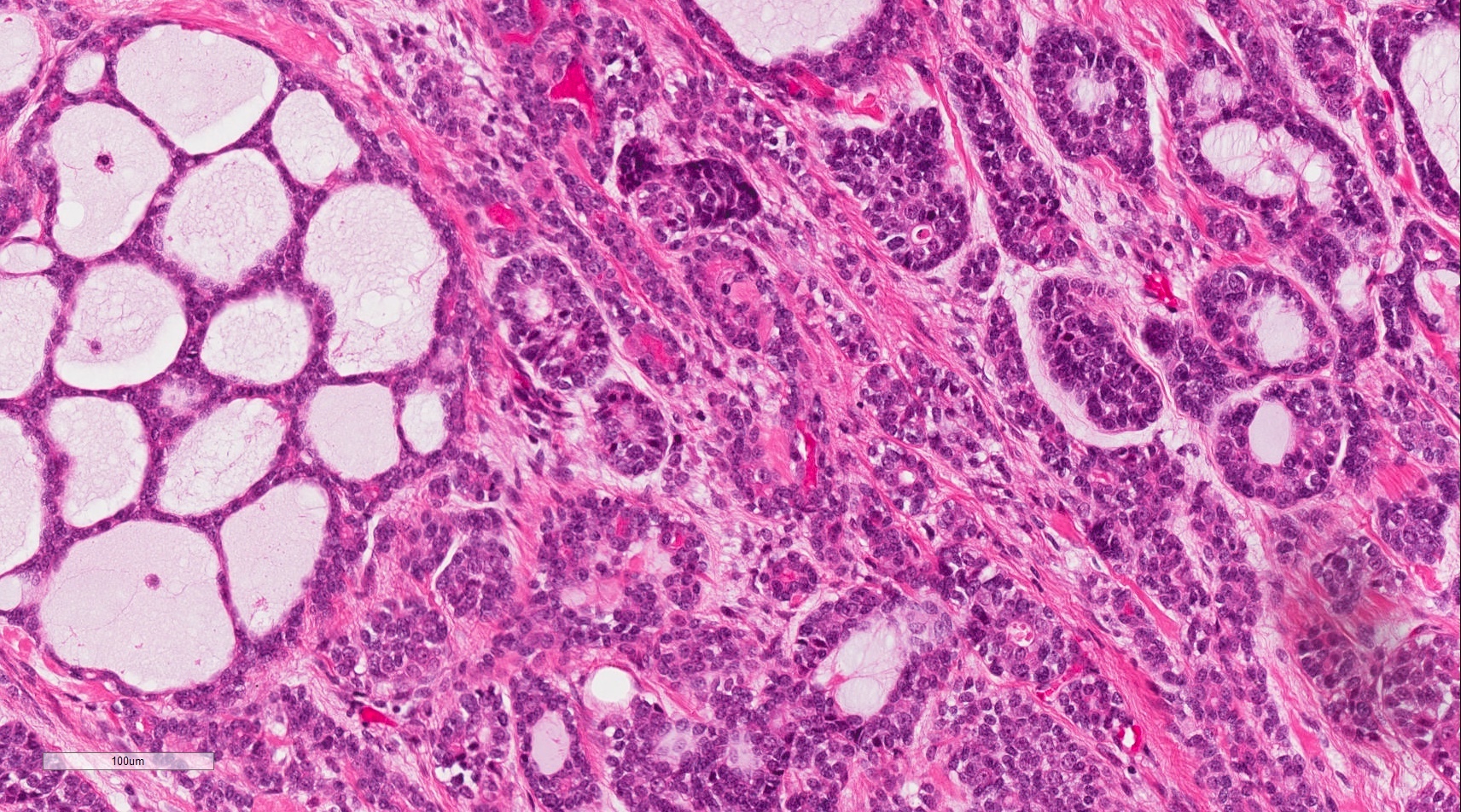
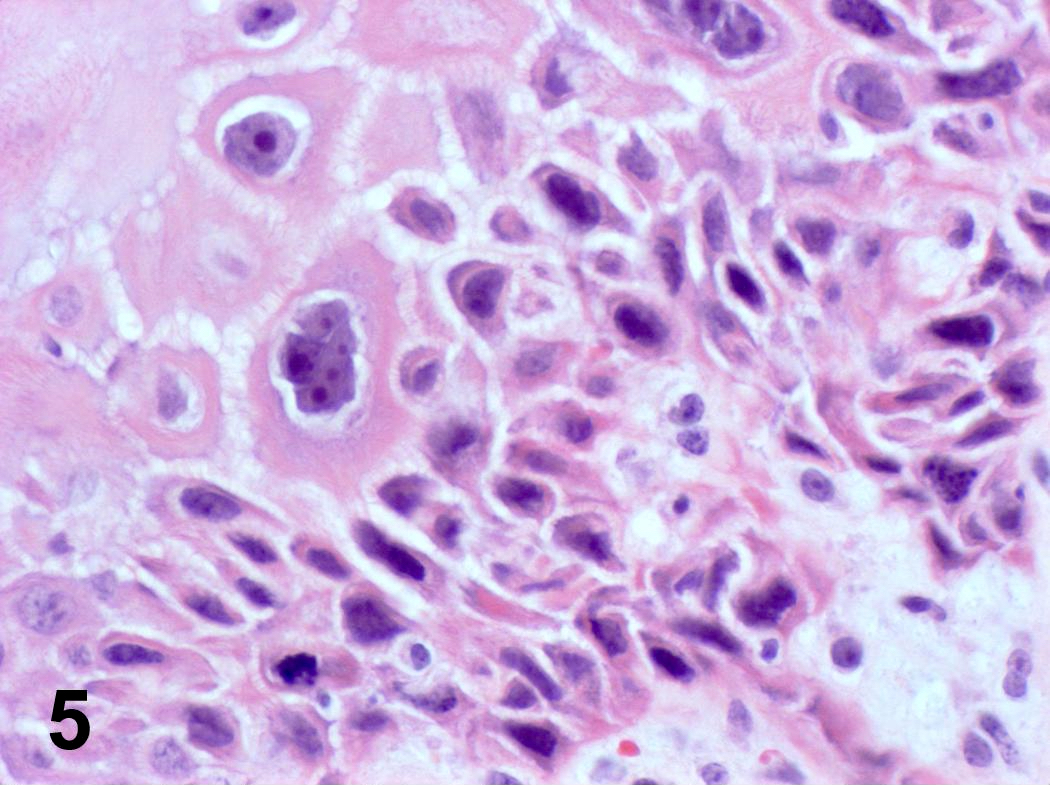
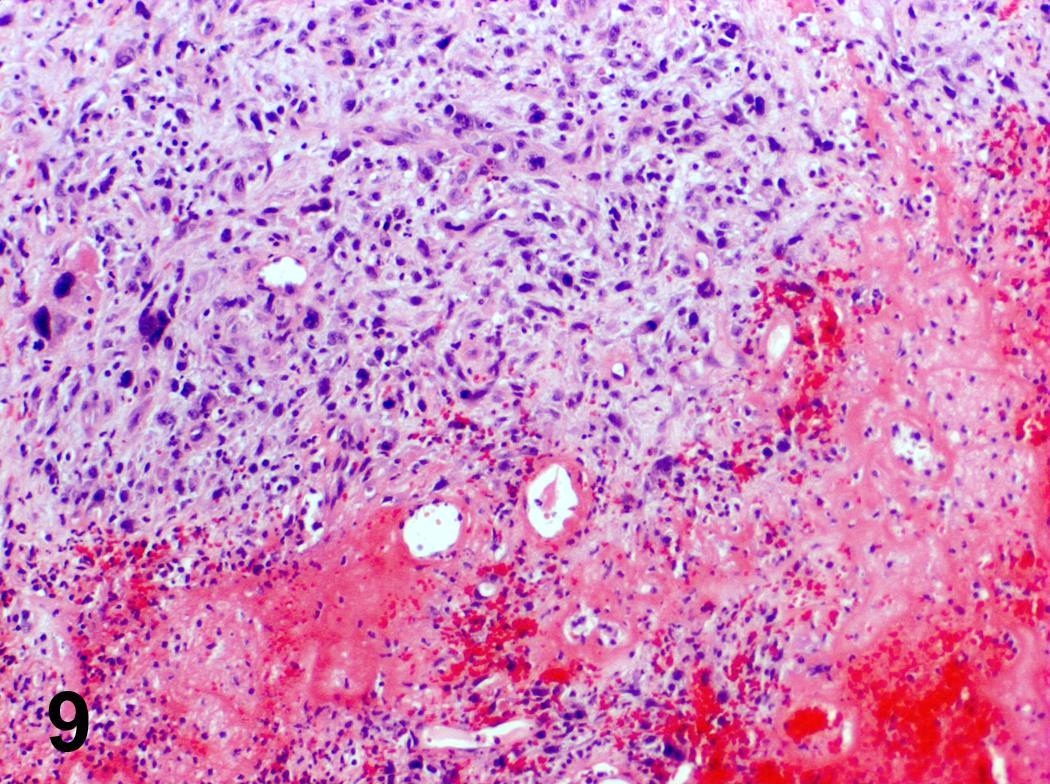
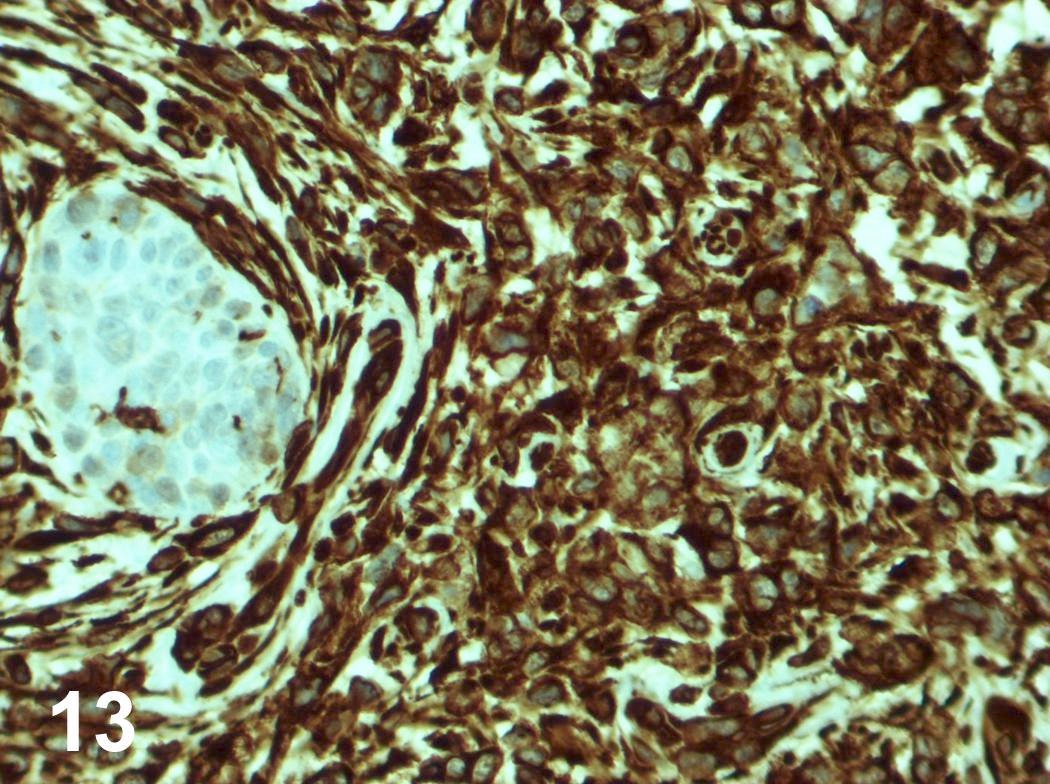
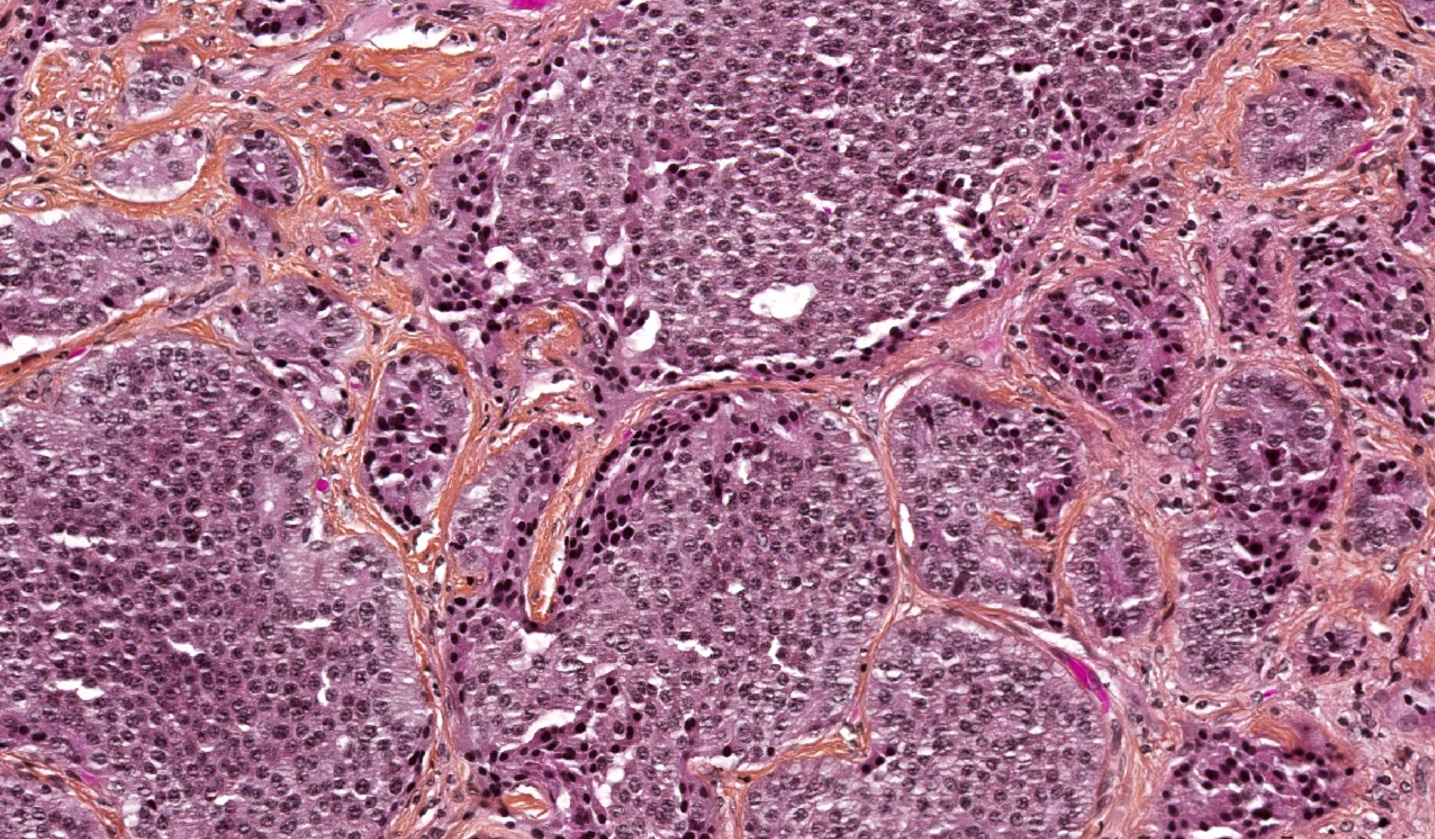
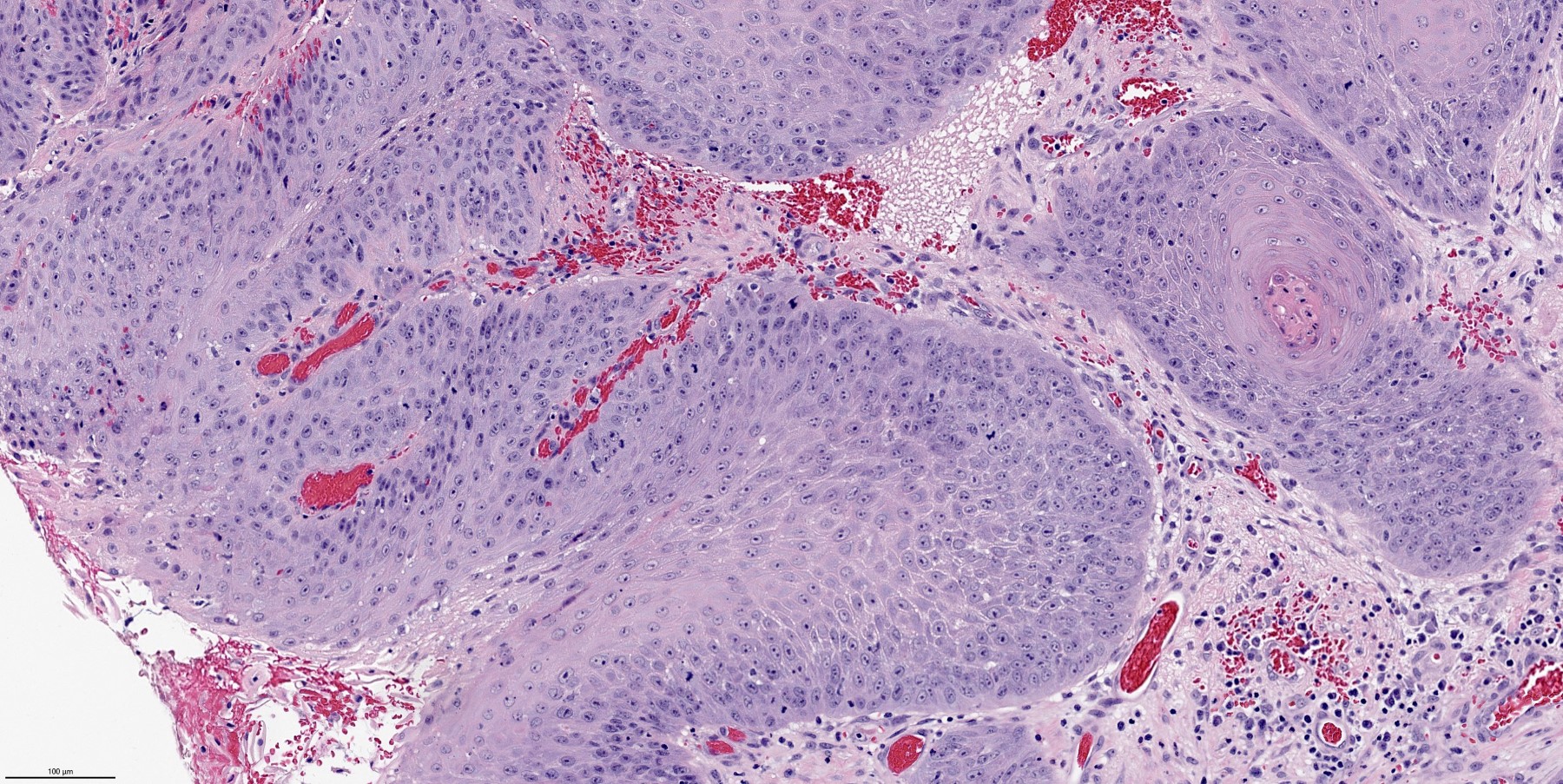
Tubular pattern: multiple duct-to-tubule-like structures lined by multiple layers consisting of ductal or myoepithelial cells or both, uniform small cuboidal tumor cells, few mitotic figures (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:495)
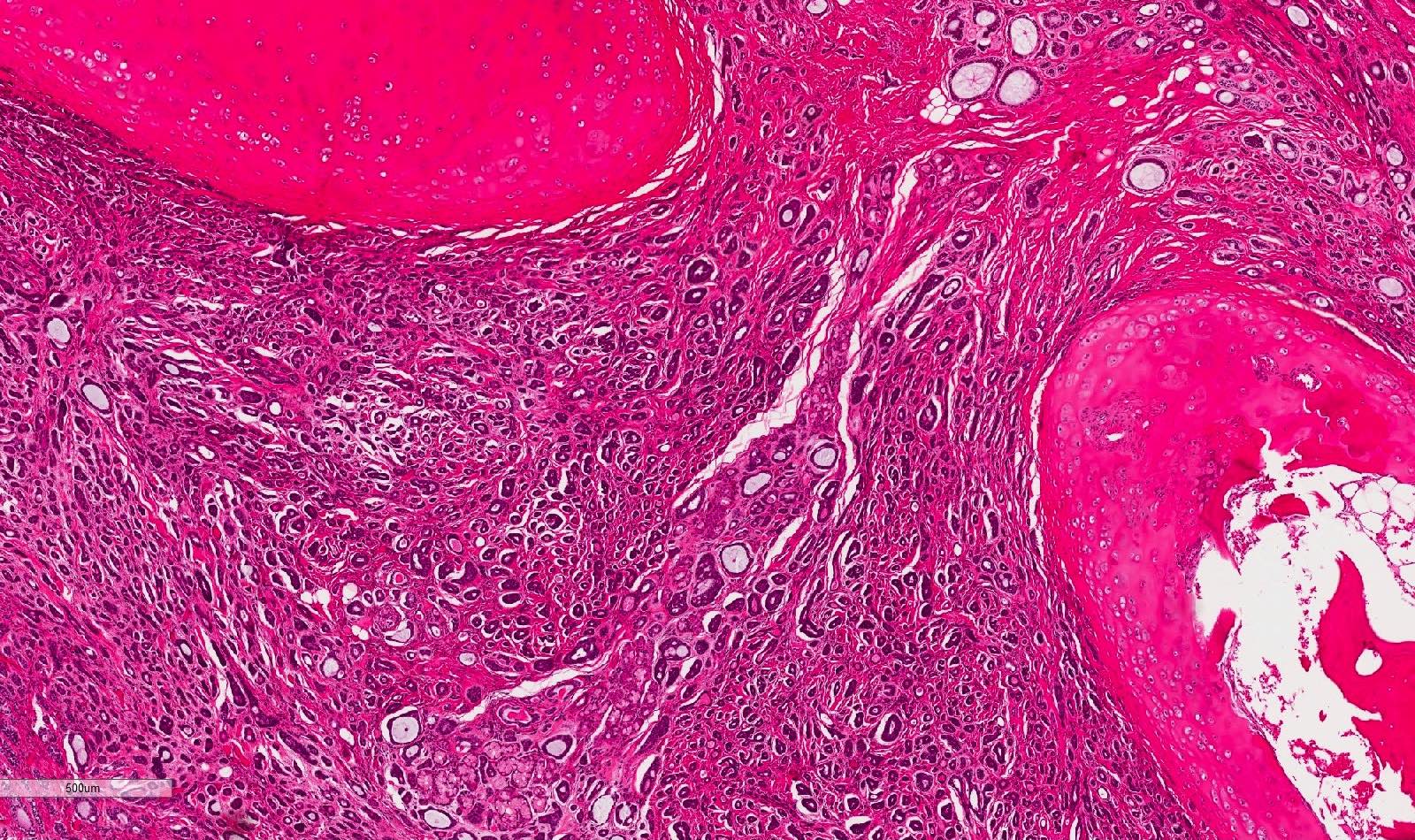
Peripheral palisading around nests with central comedonecrosis surrounded by hyalinized stroma
Board review style question #1
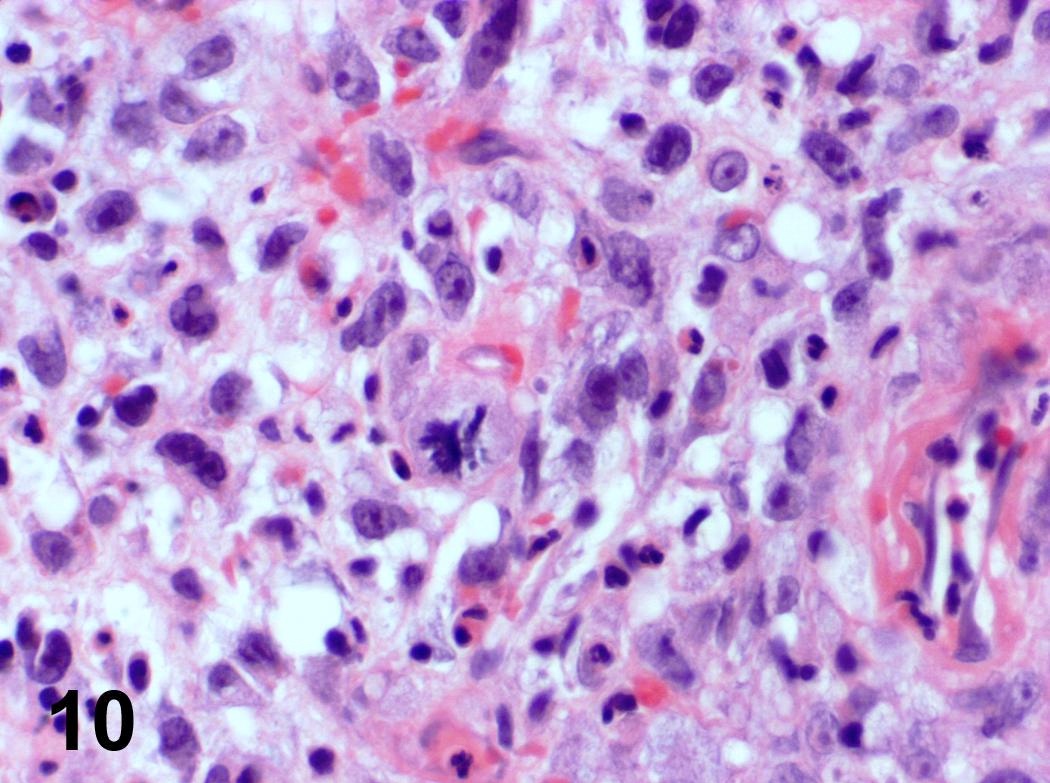
Which of the following is true about this adenoid cystic carcinoma of the larynx?
Immunohistochemical staining for CD117 will be negative in tumor cells
Perineural invasion is extremely rare in this type of tumor
The cystic spaces contain mucoid or hyalinized material
The primary site of laryngeal adenoid cystic carcinoma is the vocal cords themselves
This tumor is clinically aggressive, reflected by the high mitotic rate and basaloid cells
Board review style answer #1
C. The cystic spaces contain mucoid or hyalinized material. These spaces often contain a mildly basophilic mucoid material, a hyalinized eosinophilic product or a combined mucoid hyalinized appearance.
What is the most common malignant minor salivary gland tumor of the larynx?
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Polymorphous adenocarcinoma
Board review style answer #2
B. Adenoid cystic carcinoma. While minor salivary gland tumors of the larynx are rare overall, adenoid cystic carcinoma is the most common malignant entity in this location.
Laser therapy or bronchoscopic removal of deposits, radiation therapy, lung transplant
Gross description
Focal to diffuse nodular thickening of trachea and proximal bronchial walls with patchy mural calcification
Also extensive bronchial stenosis, postobstructive pneumonia, atelectasis
Microscopic (histologic) description
Extensive thickening of submucosa due to irregular nodular masses or sheets of amyloid, reduced submucosal glands, calcification or osseous metaplasia of larger airways
Variable multinucleated, osteoclast-like giant cells and plasma cells within amyloid
Also amyloid deposition within submucosal vessel walls
Microscopic (histologic) images
Images hosted on other servers:
Homogenous proteinous material with calcification under bronchus epithelium is Congo red+
Massive amyloid deposits
69 year old woman with seropositive erosive RA
Positive stains
Congo red (apple green birefringence with polarized light)
Differential diagnosis
Light chain deposition disease
Pulmonary lymphoproliferative disorders
Pulmonary scar tissue
Systemic amyloidosis
Tracheobronchopathia osteochondroplastica:
Submucosal bony and cartilaginous tissue projects into tracheobronchial lumen, no amyloid
Tubular structure between pharynx / root of tongue and trachea at level of cervical vertebrae C4 - C6 in males, somewhat higher in females and during childhood
Composed of cartilaginous tissue that undergoes ossification and may completely replace cartilage by age 20
At puberty, increases in size in males due to enlargement of cartilages
Cartilages are connected by ligaments and moved by numerous muscles
Trachea
Composed of imperfect rings of hyaline cartilage, fibrous tissue, muscular fibers, mucous membranes and glands
Staging anatomy
Larynx and hypopharynx
Anterior limit is anterior or lingual surface of suprahyoid epiglottis, thyrohyoid membrane, anterior commissure and anterior wall of subglottic region (composed of thyroid cartilage, cricothyroid membrane and anterior arch of cricoid cartilage)
Posterior and lateral limits include laryngeal aspect of aryepiglottic folds, arytenoids region, interarytenoid space and posterior surface of subglottic space (mucous membrane covering surface of cricoid cartilage)
Superolateral limits are tip and lateral borders of epiglottis
Inferior limit is plane passing through inferior edge of cricoid cartilage
Structures
Supraglottic portion:
Epiglottis (lingual and laryngeal aspects), false vocal cords (ventricular bands), aryepiglottic folds (laryngeal aspect), arytenoid cartilages and ventricles
Derived from third and fourth branchial pouches
Inferior boundary is horizontal plane passing through lateral margin of ventricle at its junction with superior surface of vocal cord
Glottic portion:
True vocal cords (superior and inferior surfaces) and anterior and posterior commissures
Derived from sixth branchial pouch
Subglottic portion:
Between lower border of true vocal cords and first tracheal cartilage (or lower margin of cricoid cartilage)
Derived from sixth branchial pouch
Anterior commissure:
Convergence of thyroepiglottic, vestibular and vocal ligaments and conus elasticus
Tendon provides anterior attachment for true vocal cords
Tendon also separates glottic and supraglottic parts of larynx
Arytenoid cartilage:
2 hyaline cartilages at upper border of cricoid cartilage at back of larynx that support the vocal cords
Each is pyramidal
Apex is surmounted by small, conical, corniculate cartilage
Conus elasticus:
Extends from superior border of cricoid cartilage to free edge of vocal cord, then thickens to form vocal ligament, which runs length of true vocal cord close to mucosal surface, then continues along floor of ventricle as thyroglottic ligament
Cricoid cartilage:
Hyaline cartilage that is smaller but thicker and stronger than thyroid cartilage
Upper edge is 1 cm below true vocal cords at mid larynx
Forms the only complete trachiobronchial ring with posterior quadrate lamina (deep and broad, 2 - 3 cm high) and anterior arch that is narrow and convex
Articulates with inferior horns of thyroid cartilage
Cuneiform cartilages: 2 small, elongated pieces of cartilage on either side of aryepiglottic fold
Epiglottis: thin, bicycle saddle-like and elastic fibrocartilage
Apex is attached to inner thyroid cartilage just above anterior commissure by thyroepiglottic ligament
Projects up behind tongue and body of hyoid bone, partly covers laryngeal entrance
Sides are attached to arytenoid cartilages by aryepiglottic folds
Upper and anterior surface is free, covered by mucous membrane reflected onto pharyngeal tongue and lateral wall of pharynx to form median and lateral glossoepiglottic folds
Median glossoepiglottic fold divides area between base of tongue and epiglottis into 2 valleculae
Not essential for respiration, phonation or deglutition
Hypopharynx:
Comprises posterolateral pharyngeal wall (from level of floor of valleculae to level of inferior border of cricoid cartilage), postcricoid esophagus (has anterior wall and extends from level of arytenoids cartilages superiorly to inferior border of cricoid cartilage) and pyriform sinuses (lie lateral to and below opening of larynx, each bounded laterally by medial aspect of thyroid lamina and medially by aryepiglottic fold)
Trachea:
Cartilaginous and membranous tube (also called windpipe), extending from lower larynx at C6 to upper border of T5 vertebrae, where it divides into right and left mainstem bronchi
Flattened posteriorly
11 cm long, 2 - 2.5 cm in diameter, diameter greater in men than women, greater in adults than children
Anteriorly: contacts thyroid isthmus, inferior thyroid veins, neck muscles, cervical fascia, anterior jugular veins, manubrium sterni, thymus, left innominate vein, aortic arch, innominate and left common carotid arteries, deep cardiac plexus
Posteriorly: contacts esophagus
Right bronchus appears to be a more direct continuation of trachea and so is the site of most foreign bodies
Supplied by inferior thyroid arteries
Pre-epiglottic space: bounded posteriorly by epiglottic cartilage and thyroepiglottic ligament, anteriorly by thyroid cartilage and thyrohyoid membrane and superiorly by hypoepiglottic ligament; space communicates laterally with paraglottic space above ventricle
Pyriform sinus: not strictly part of larynx; inverted 3 sided pyramid with apex inferiorly at level of cricopharyngeus muscle, bounded superiorly by glossoepiglottic folds, medially by aryepiglottic folds, laterally by pharyngeal wall
Thyroid cartilage:
Largest cartilage of larynx
Shield shaped forming anterior surface of larynx and acute angle in midline of neck (laryngeal prominence, Adam's apple)
Originally only hyaline cartilage but ossifies at age 25 at sites of muscle origin or insertion
Lower edge is 1 cm below anterior commissure
Lymphatics:
Separate systems exist above and below ventricle
Are also subdivided as superficial (mucosal) and deep
Few lymphatics are present in true vocal cord
Pyriform sinus drains laterally into deep cervical nodes, occasionally to paratracheal nodes
Supraglottic lymphatics drain through thyrohyoid membrane into upper cervical and anterosuperior nodes
Subglottic lymphatics drain into prelaryngeal (Delphian) node on cricothyroid membrane, then into pretracheal, paratracheal and supraclavicular nodes
Diagrams / tables
Images hosted on other servers:
Sagittal section
Coronal section
Entrance viewed from above
Laryngoscopic view
Laryngeal cartilages
Vocal cords and muscles
Muscles
Ligaments
Trachea and bronchi
Tracheal bifurcation
Transverse section
Gross images
Images hosted on other servers:
True and false vocal cords
Microscopic (histologic) description
Junction between epithelial types may be abrupt or separated by transitional area; patches of squamous epithelium in respiratory epithelium are common, particularly in smokers
Dendritic melanocytes may be present in basal layer, particularly in blacks
Epiglottis: stratified squamous epithelium similar to oral cavity with modified salivary glands that secrete thick mucous; laryngeal surface also has pits containing mucous glands
Cartilage has full thickness fenestrae that communicate with pre-epiglottic space, which contains fat and areolar tissue
False vocal cords and other supraglottic larynx: ciliated, columnar epithelium extending into ventricle of Morgagni with submucosal modified salivary gland epithelium
Glottis: space between 2 vocal cords
Hypopharynx: covered by nonkeratinizing stratified squamous epithelium; contains mucosal glands, scattered lymphoid aggregates and rich lymphatic plexus
Reinke space: lamina propria of true vocal cord, between base of squamous epithelium and vocal ligament
True vocal cords: stratified squamous epithelium with no / rare submucosal glands
Subglottic larynx: epithelium resembles trachea / major bronchi - ciliated columnar epithelium with submucosal glands
Trachea:
Cartilage:
16 - 20 imperfect rings, with circular cartilaginous defect posterior and replaced by fibrous tissue and muscular fibers
Each cartilage is 4 mm in depth, 1 mm in thickness
Radical surgical excision, radical neck dissection and supplemental radiochemotherapy
Gross description
Firm to hard, tan-white masses, may have central necrosis and up to 6 cm
Microscopic (histologic) description
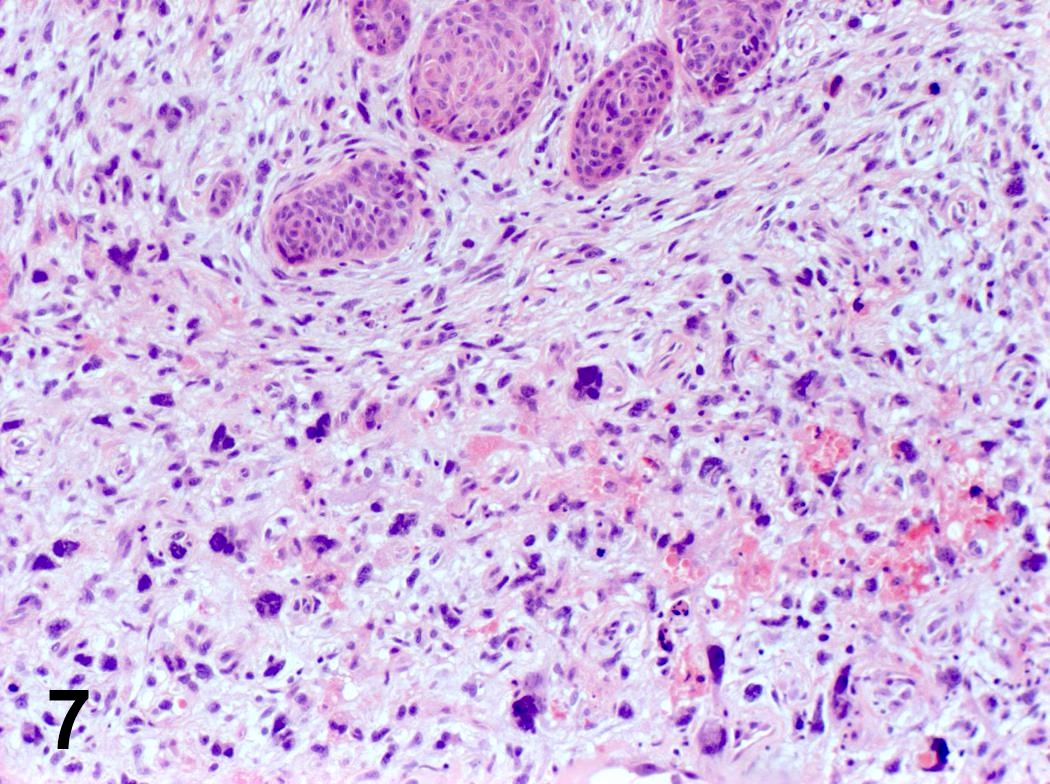
Typical areas of squamous cell carcinoma (invasive and in situ) with nests or cords of small crowded cells with minimal cytoplasm, hyperchromatic nuclei, comedonecrosis, prominent hyalinization and peripheral palisading, small cystic spaces and mitotic activity
Usually 3 cm or more, invasion into bone of ossified laryngeal cartilage
Microscopic (histologic) description
Diagnostic fields often small; have atypical, neoplastic chondrocytes with loss of normal architecture and distribution and invasion of bone; laryngeal cartilage usually has undergone endochondral ossification
Low grade chondrosarcoma: slight increase in cellularity, mild atypia with binucleated chondrocytes within 1 lacuna; difficult to distinguish from chondroma; can report as "cartilaginous tumor without obvious evidence of malignancy, further classification pending removal of entire lesion"
High grade chondrosarcoma: hypercellular with enlarged, binucleated and multinucleated atypical cells with increased nuclear to cytoplasmic ratio, irregular nuclear chromatin, prominent nucleoli, mitotic figures (may be atypical) and variable tumor necrosis
Dedifferentiated chondrosarcoma: also called chondrosarcoma with additional malignant mesenchymal component (Am J Surg Pathol 1988;12:314)
For columnar epithelium, resembles cervical dysplasia
Associated with HPV 16 and p53 expression
Leukoplakia: clinical term describing any white lesion on a mucous membrane; usually associated with mucosal thickening and not dysplasia
Erythroplakia: clinical term describing red lesion on a mucous membrane; usually associated with dysplasia or malignancy; in smokers, for squamous epithelium, features of nuclear pleomorphism, mitotic activity, abnormal mitotic figures and stromal inflammation are associated with progression to invasive carcinoma
Keratosis: increase in surface keratin, often with prominent granular cell layer and orthokeratin (cells without nuclei) mixed with parakeratin (flat keratotic cells with pyknotic nuclei); not related to dysplasia
Dyskeratosis: abnormal keratinization of epithelial cells
Dysplasia: spectrum of abnormal epithelial maturation and cellular atypia that may or may not precede invasive carcinoma
Carcinoma in situ: full thickness dysplasia of mucosa without violation of basement membrane; same as severe dysplasia
Prognostic factors
Overall, low risk of development of invasive squamous cell carcinoma after dysplasia
For mild dysplasia, 7% develop in situ or invasive carcinoma versus 24% with moderate dysplasia versus 25% with severe dysplasia
High risk of progression to invasive carcinoma for severe keratinizing dysplasia versus nonkeratinizing dysplasia
Treatment
Mild / moderate dysplasia may be reversible
Severe dysplasia requires intervention (vocal cord stripping, surgery, radiation therapy, endoscopic laser resection) as well as surveillance of entire upper aerodigestive tract
Gross description
Erythema of involved areas
Microscopic (histologic) description
Mild dysplasia:
Normal or mildly disordered basal layer with retained maturation and stratification of upper layers
Mild nuclear atypia and possibly mitotic figures in basal third of epithelium
No abnormal mitotic figures
Variable keratosis and chronic inflammatory infiltrate
Moderate dysplasia:
Moderate nuclear atypia, usually with prominent nucleoli and mitotic figures, most pronounced in lower two - thirds of epithelium
Cell maturation and stratification are present in upper layer
No abnormal mitotic figures
Variable keratosis
Severe / high grade:
Marked nuclear abnormalities and loss of maturation greater than two - thirds of epithelium
Large atypical nuclei, some bizarre; nuclear pleomorphism is common
May have prominent nucleoli
Mitotic figures high in epithelium, often abnormal
Keratinizing dysplasia:
Defined as lesions in which epithelial alterations are so severe that there is a high probability of progression to invasive carcinoma
Includes dyskeratotic cells and mitotic figures with variable atypical forms above basal zone, variable surface keratinization
Carcinoma in situ:
Full thickness nuclear abnormalities without stromal invasion
Cells are usually keratinized but may be basal-like
Often lumped together with severe dysplasia
May represent peripheral portion of invasive carcinoma
Papillary carcinoma in situ:
Papillary fronds with a fibrovascular core covered by squamous epithelium with marked atypia
Note: invasion may occur by dysplastic cells without full thickness epithelial involvement
Open in midline posteriorly, ink margins, take tissue for special studies
Fix specimen
Remove hyoid bone and inspect pre-epiglottic tissue
Slice larynx (see below) and photograph
For supraglottic and hypopharyngeal carcinomas, blocks should include relationship between tumor and anterior resection margin at base of tongue
For partial laryngectomy specimens, inferior margin is usually most critical
At least one section per 1 cm of tumor for large tumors, including tumor center and periphery and maximum depth of invasion
Submit entire tumor if can do so in 5 sections or less
Submit resection margins
Nonneoplastic mucosa
Bone or cartilage that is grossly involved by tumor
Thyroid gland if present
Lymph nodes
Tracheostomy site
Glottic tumors: show tumor relationship to ventricle, thyroid cartilage and cricoid cartilage by coronal section (plane dividing body into front and back, coronal section of normal larynx)
Epiglottic tumors: determine extent of invasion of preepiglottic space by sagittal sections (plane dividing body into right and left, sagittal section of larynx)
Pyriform sinus tumors: show invasion of supraglottic larynx and thyroid lamina by horizontal sections
Mucus retention cyst caused by obstruction of mucus gland ducts within mucus membrane; represents 75% of all laryngeal cysts
Saccular cyst
Saccule is a membranous sac in the larynx, located between the false vocal cords and the inner surface of the thyroid cartilage, which contains mucous secreting glands
Obstruction of the mucous gland ducts of the laryngeal saccule with subsequent accumulation of secretions results in a submucosal cyst
Represents 25% of all laryngeal cysts; further classified as anterior or lateral
Lateral saccular cysts are predominantly congenital, formed during embryogenesis due to aberrant entrapment of developing saccule by third and fifth brachial arches; these remain quiescent until a trigger such as an upper respiratory tract infection causes expansion of the cyst
Lined by respiratory or squamous epithelium or a flattened epithelium
Epithelial lining may be papillary in architecture
May contain keratin or mucin
May have a lymphoid component in cyst wall
Includes both ductal and saccular cysts; differentiation of ductal from saccular cysts is not possible histologically, so differentiation rests on clinical parameters
Tonsillar cyst
Resembles palatine tonsillar crypt
Lined by stratified squamous epithelium
Lymphoid follicles with germinal centers seen in cyst wall
Oncocytic cyst
Unilocular or multilocular cyst lined by uniform oncocytic epithelial cells
May have prominent intraluminal papillary architecture or hyperplastic solid nests
Unlike Warthin tumor, doesn't have bilayered oncocytes and lymphoid stroma
Oncocytes originate from metaplasia of seromucinous gland ducts in response to aging and chronic smoking resulting in disturbance of mitochondrial enzyme organization
Originates in ventricles or false vocal cords, presents as supraglottic mass
Also called oncocytic papillary cystadenoma, oncocytic adenomatous hyperplasia, oncocytoma
Difficult to distinguish from saccular cyst if deficient in thyroid tissue
Differentiated on basis of exact anatomical location of cyst, as thyroglossal duct cysts are related with the hyoid bone and located in the midline of the neck
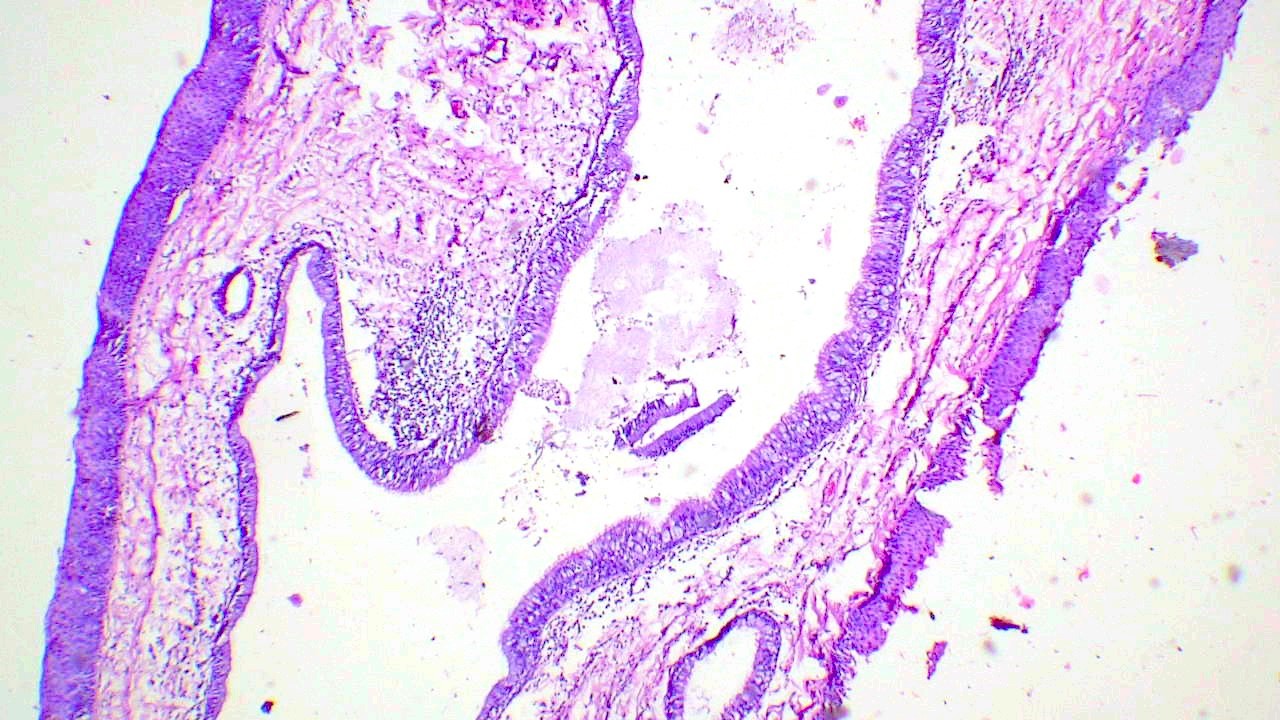
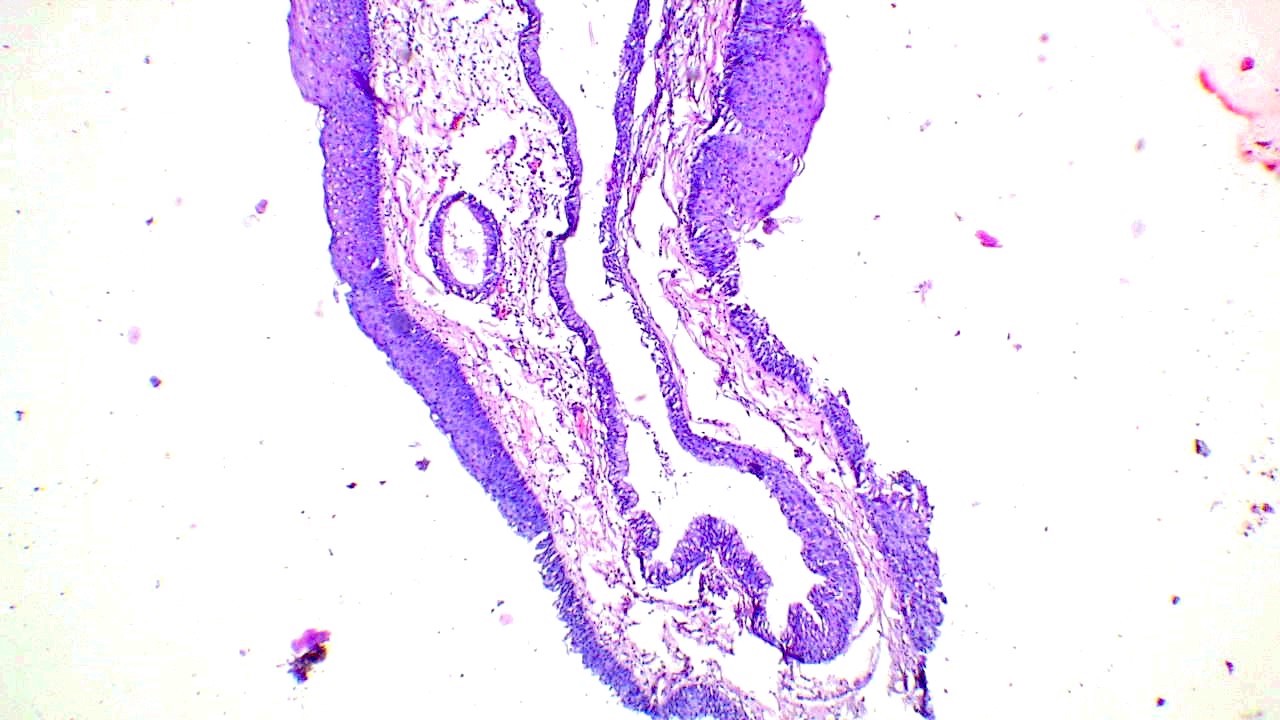
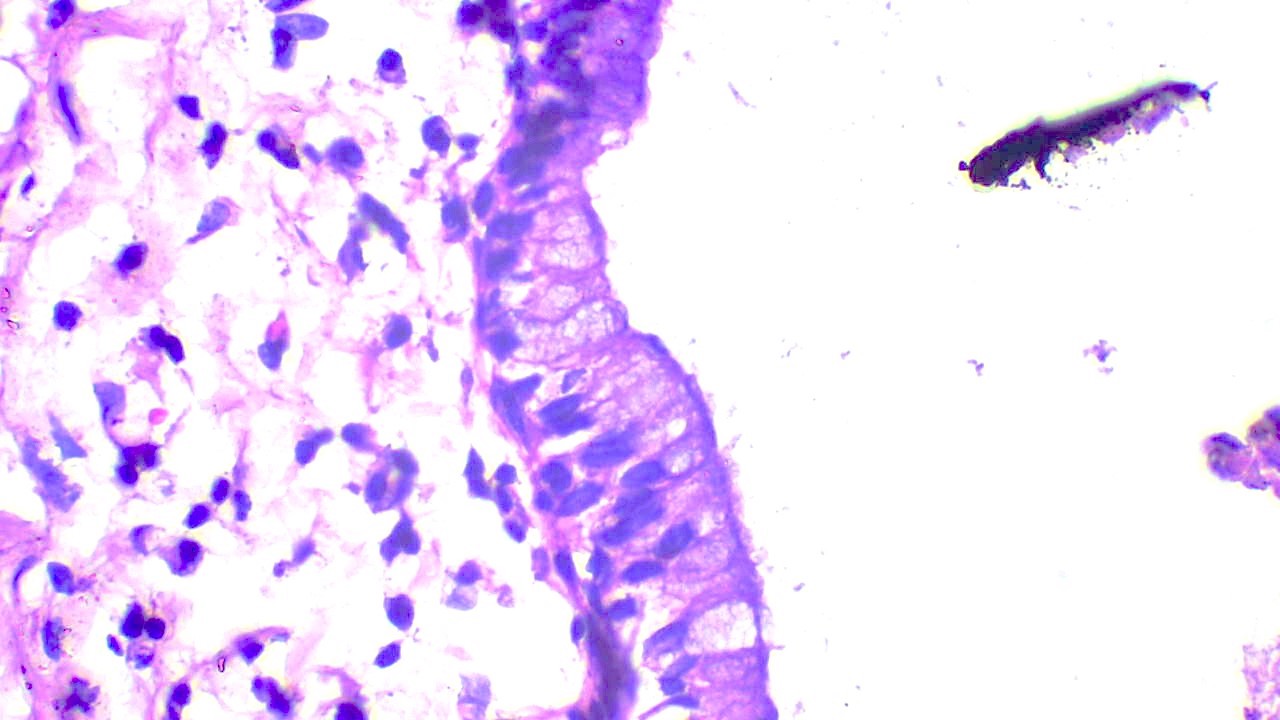
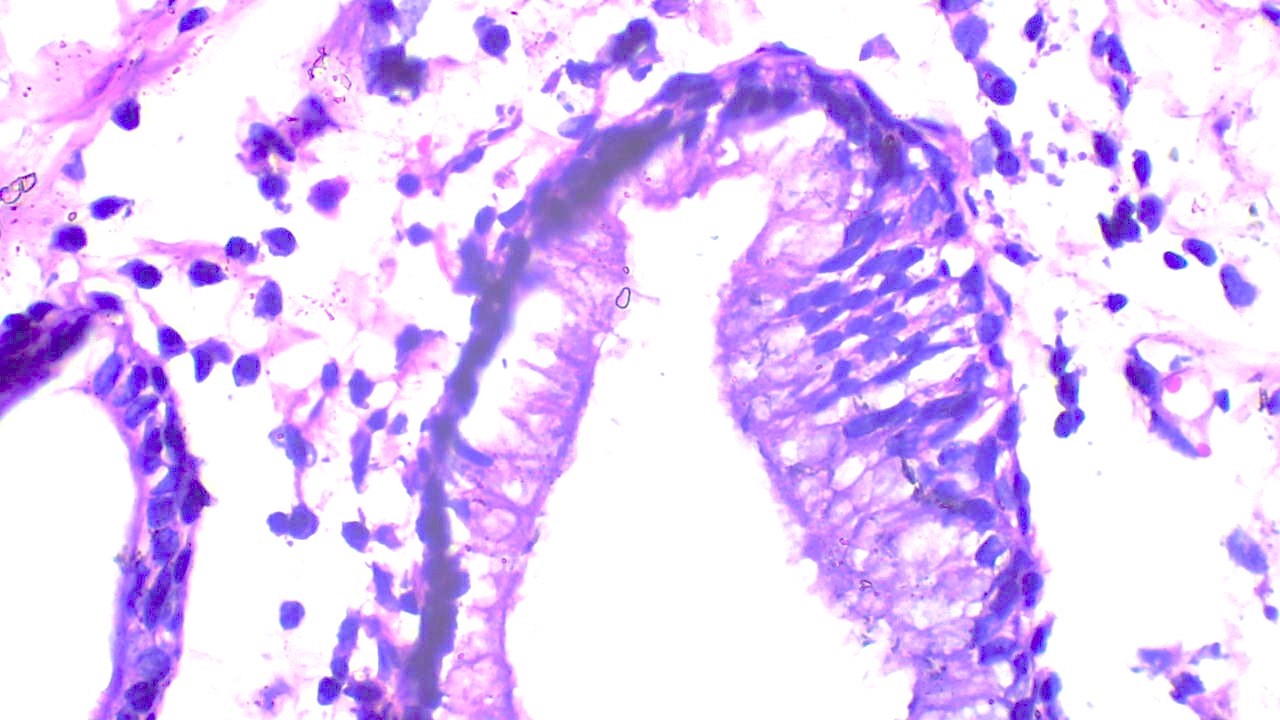
A 61 year old woman presented with hoarseness of voice and was found to have a nodular lesion in the larynx with the microscopy shown above. What is the diagnosis?
Laryngeal epithelial cyst
Laryngocele
Squamous papilloma
Vocal cord polyp
Board review style answer #1
A. Laryngeal epithelial cyst. The section shows a distended cystic lesion lined by columnar epithelial cells with focal squamous metaplasia. The lesion is entirely confined within the larynx with no connection to lumen or dysplasia of overlying squamous epithelium. Answer B is incorrect because laryngocele is an air filled cavity communicating with the laryngeal lumen. Answer C is incorrect because squamous cell papilloma is an exophytic lesion lined by hyperplastic stratified squamous epithelium. Answer D is incorrect because vocal cord nodule / polyp is a surface lesion with no intralaryngeal extension.
Which type of laryngeal cyst needs follow up for a longer period of time after surgical excision?
Ductal cyst
Oncocytic cyst
Saccular cyst
Tonsillar cyst
Board review style answer #2
B. Oncocytic cyst. Oncocytic cysts need longer follow up because of their association with recurrence and multifocality. Anwers A, C and D are incorrect as surgical excision alone is sufficient and these cysts are not known to be associated with recurrence.
Neuroendocrine neoplasms are composed of neuroendocrine epithelial neoplasms that arise in the larynx and are either well differentiated or poorly differentiated (high grade)
Essential features
Laryngeal neuroendocrine neoplasms are divided into 3 categories: well differentiated neuroendocrine neoplasms, poorly differentiated neuroendocrine carcinomas and mixed neuroendocrine - nonneuroendocrine neoplasm
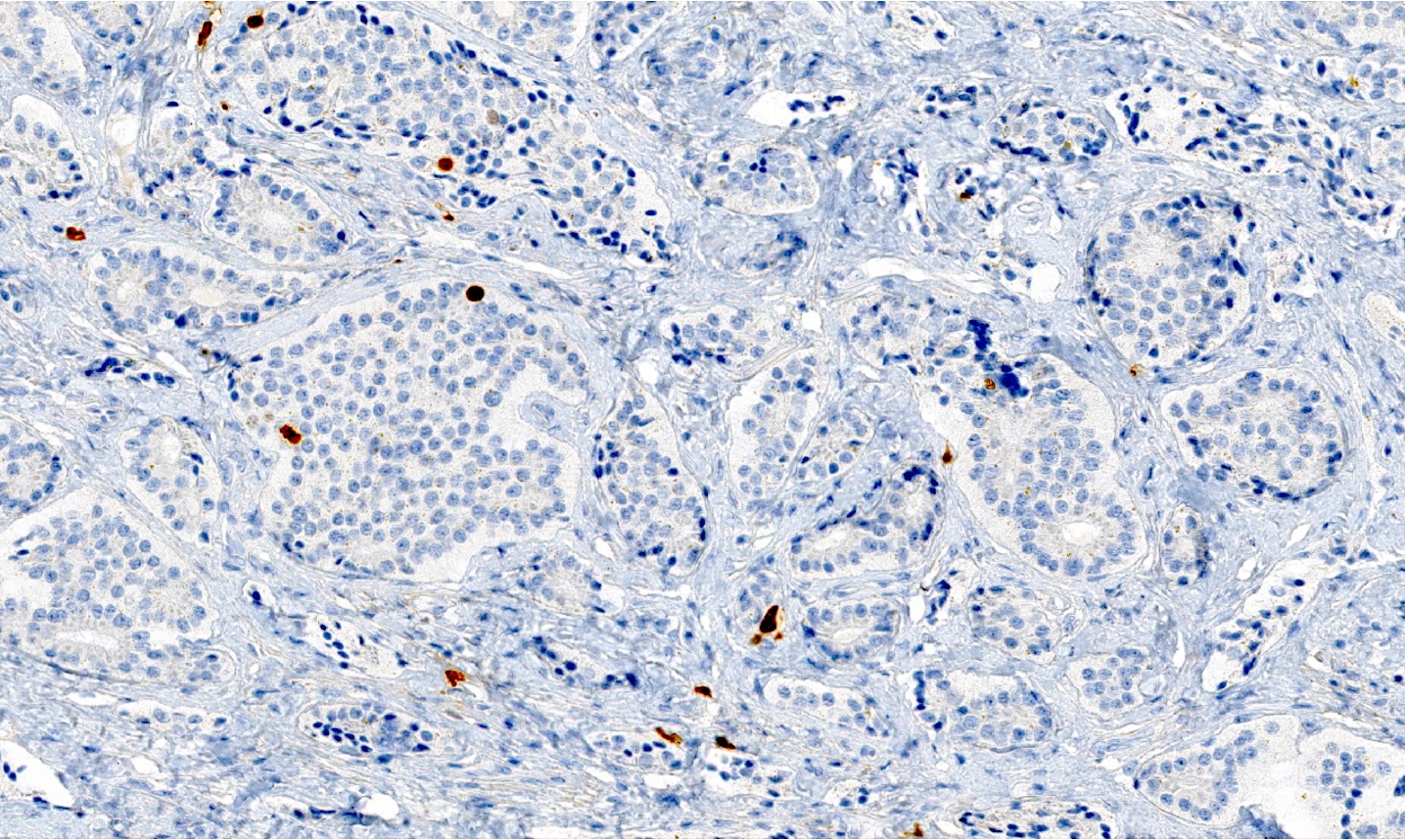
Well differentiated neuroendocrine neoplasm with immunohistochemical evidence of neuroendocrine differentiation and positivity for at least 1 keratin
Ki67 proliferation index
No abnormal p53 staining and no loss of Rb (in selected cases with Ki67 > 20%)
Poorly differentiated neuroendocrine carcinomas
Small cell neuroendocrine carcinoma
High grade carcinoma
Cell size smaller than diameter of 3 lymphocytes
Prominent apoptotic bodies and necrosis
Large cell neuroendocrine carcinoma
High grade malignancy carcinoma
Cell size larger than diameter of 3 lymphocytes
Peripheral palisading, rosette formation or comedo pattern necrosis
Terminology
Neuroendocrine neoplasms (NEN) are subclassified into 2 subtypes
Well differentiated neuroendocrine neoplasms (NET)
Well differentiated neuroendocrine neoplasms: variable prognosis and based on the presence of distant metastasis and lymph node metastases (Head Neck 2015;37:707)
56 year old woman presented with painful subcutaneous skin lesions that were diagnosed as metastatic carcinoma at an outside facility; diagnosed as large cell neuroendocrine carcinoma (J Cutan Pathol 2018;45:229)
59 year old man presented to a community based hospital complaining of a left sided neck mass that has been present for ~1 month; diagnosed as small cell neuroendocrine carcinoma (Ear Nose Throat J 2022;101:NP96)
65 year old man, a smoker, and 63 year old man, a former smoker, presented with well differentiated neuroendocrine tumor (grade moderately differentiated neuroendocrine carcinoma) causing death 13 and 33 months after diagnosis (Arch Pathol Lab Med 1992;116:253)
Treatment
G1 NET: local resection in the sense of either open or transoral endoscopic laser surgical partial laryngectomy is recommended (Laryngorhinootologie 2021;100:S1)
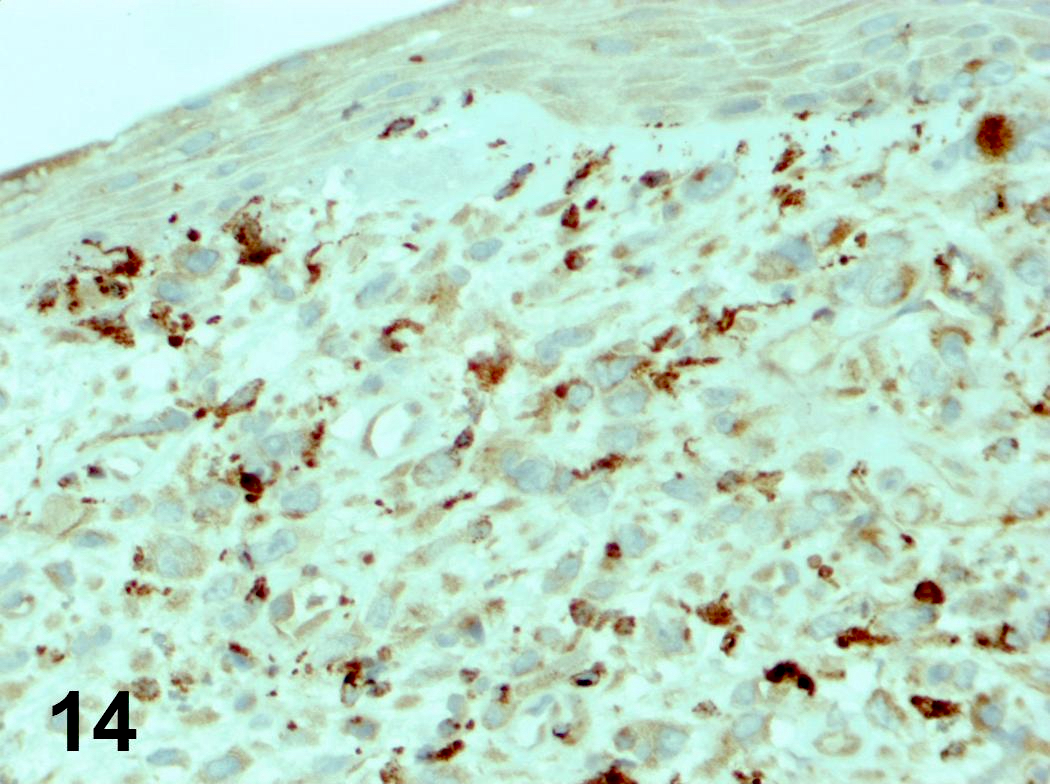
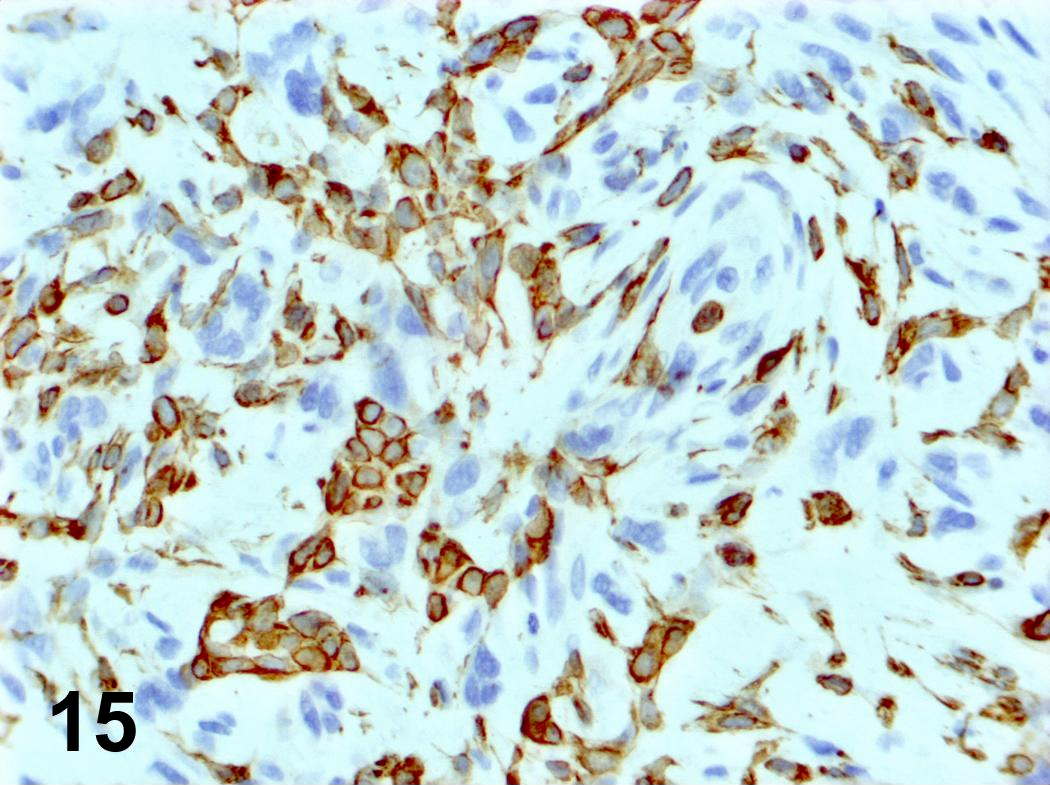
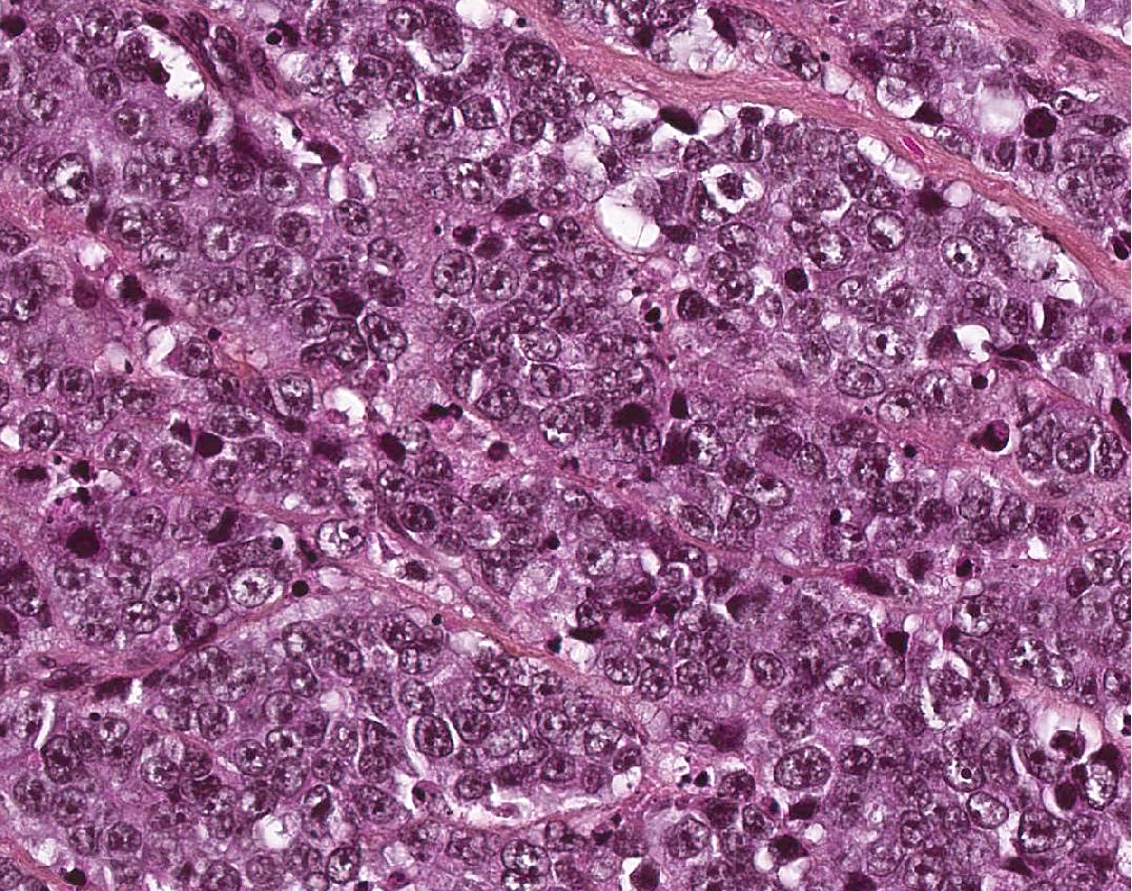
Classical cytomorphology of tumor cells: uniform / monotonous round to oval nuclei, dispersed (salt and pepper) nuclear chromatin and ample granular pale eosinophilic cytoplasm often without distinct cell borders
Uncommon cytomorphology of tumor cells: plasmacytoid, clear, oncocytic and rhabdoid (Head Neck Pathol 2022;16:375)
Mild to focally moderate nuclear pleomorphism
Necrosis, mitotic count and Ki67 proliferation index
Grade 1: no necrosis and < 2 mitoses/2 mm² / Ki67 < 20%
Grade 2: necrosis (often punctate [individual cell] and less commonly, coagulative [confluent foci]) or 2 - 10 mitoses/2 mm² / Ki67 < 20%
Grade 3: > 10 mitoses/2 mm² / Ki67 > 20% without NEC cytomorphology
Well differentiated neuroendocrine tumor, WHO grade 2 (see comment)
Comment: The presence of increased mitotic activity (4 mitoses/2 mm²) on this biopsy combined with the classic morphology of a well differentiated neuroendocrine tumor and positivity of immunohistochemical stains for cytokeratin AE1 / AE3, synaptophysin, chromogranin and 10% for Ki67 proliferative index support the diagnosis of well differentiated neuroendocrine tumor WHO grade 2 (out of 3).
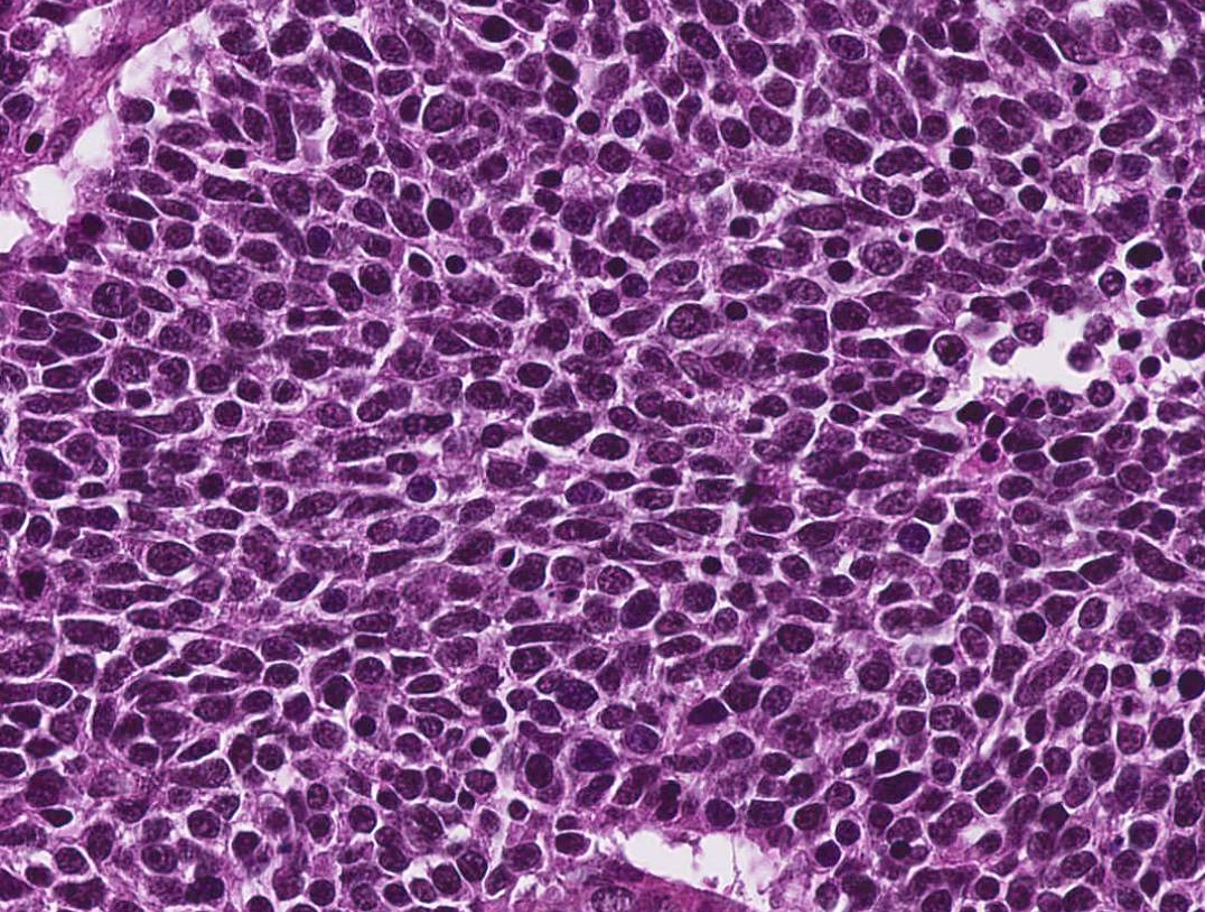
Has different morphology with nuclear pleomorphism, hyperchromatic and peripheral palisading, often with central comedo type necrosis, without expression neuroendocrine markers (focally may be seen)
Which of the following diagnoses regarding neuroendocrine neoplasms of the larynx with 15 mitoses/2 mm² and Ki67 30% without necrosis is correct?
Poorly differentiated neuroendocrine carcinomas
Well differentiated neuroendocrine tumor, grade 1
Well differentiated neuroendocrine tumor, grade 2
Well differentiated neuroendocrine tumor, grade 3
Board review style answer #1
D. Well differentiated neuroendocrine tumor, grade 3 because the diagnostic criteria applied with NET cytomorphology with > 10 mitoses/2 mm² and Ki67 > 20% and most importantly, without NEC cytomorphology.
Which of the following statements regarding differential diagnosis of neuroendocrine neoplasms of the larynx is true?
Adenoid cystic carcinoma is diffusely positive for p16
Basaloid squamous cell carcinoma has the identical morphology as the poorly differentiated neuroendocrine carcinoma
Calcitonin and TTF1 may be expressed in neuroendocrine neoplasms
Paraganglioma could express cytokeratin
Treatment of neuroendocrine carcinomas is different based on the subtype
Board review style answer #2
C. Calcitonin and TTF1 may be expressed in neuroendocrine neoplasms.
Adenoid cystic carcinoma is diffusely positive for p16, as this biomarker can be seen in NEC or adenoid cystic carcinoma (A).
Basaloid squamous cell carcinoma is distinguished from poorly differentiated neuroendocrine carcinoma by its diffuse squamous marker expression (e.g., p40, CK5/6) and lack of neuroendocrine marker (synaptophysin, chromogranin, INSM1) and TTF1 staining (B).
Paraganglioma could not express cytokeratin (D).
Treatment of neuroendocrine carcinomas is not different based on the subtype of small and large cell neuroendocrine carcinoma (E).
Uncommon; exophytic growth pattern, features of carcinoma in situ plus foci of invasion
Mean age in 60s
Usually in larynx, oral cavity, oropharynx, hypopharynx and sinonasal tract
Associated with HPV
Relatively good prognosis; usually T2
Difficult to determine invasion in biopsy specimens, although should consider invasive if clinically appreciable exophytic mass plus marked atypia, even without definitive stromal invasion
Treatment
Surgery
Gross description
Often solitary with exophytic or papillary growth; 2 mm to 4 cm
Microscopic (histologic) description
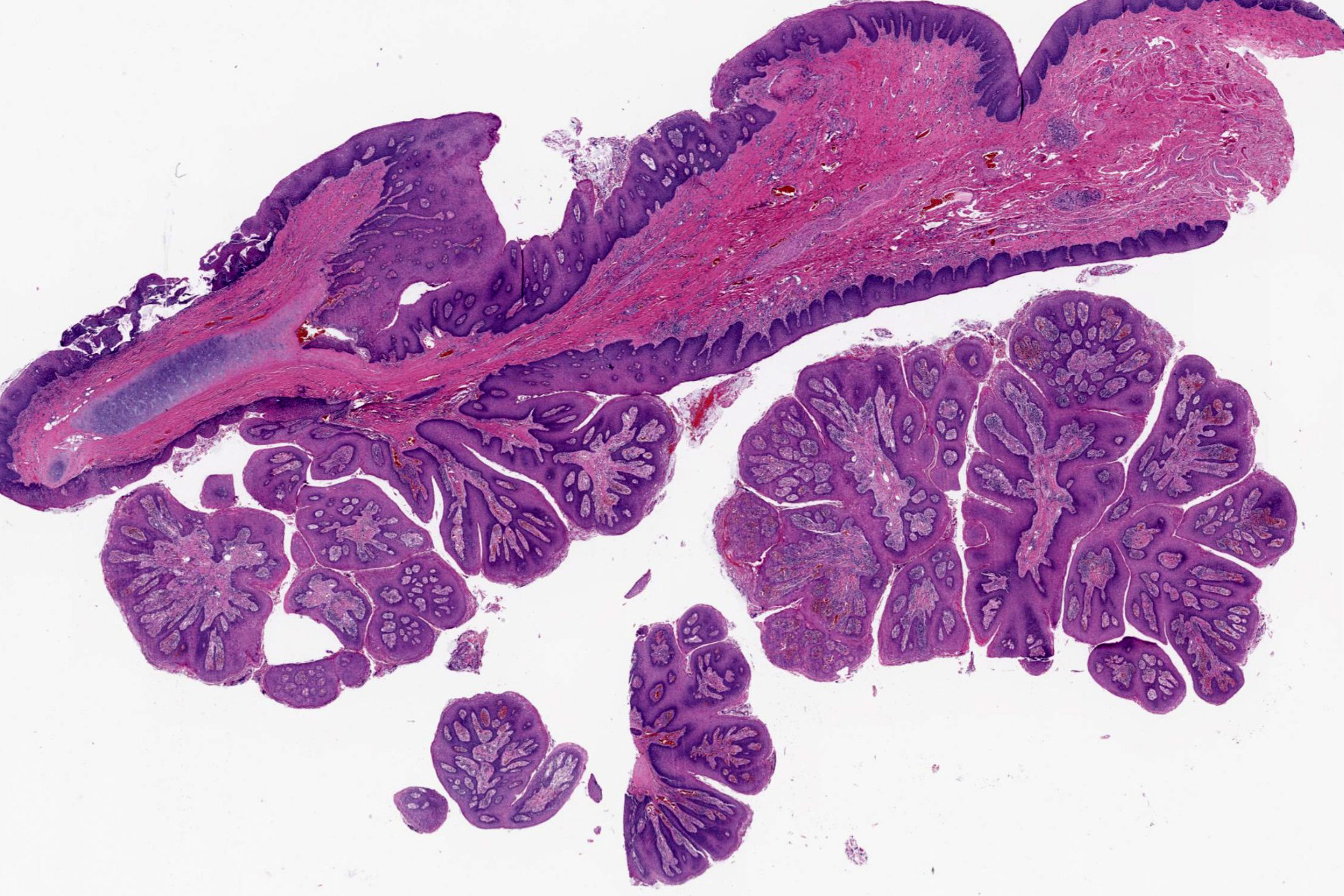
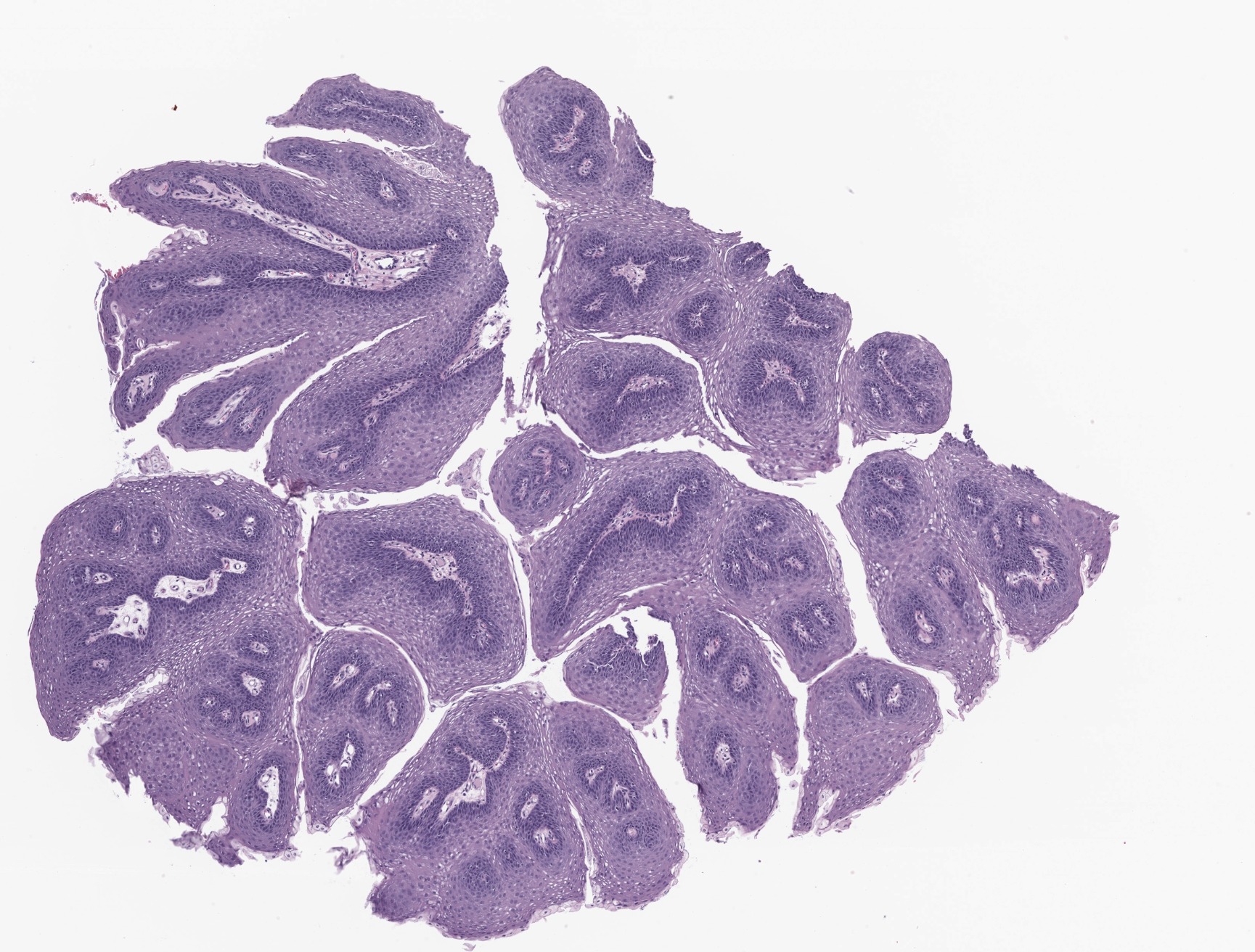
Finger-like projections with fibrovascular cores or broad based bulbous growth with rounded projections and limited fibrovascular cores
Overlying squamous epithelium is malignant; usually no / limited surface keratinization
Differential diagnosis
Laryngeal papillomatosis:
Bland epithelial proliferation with no / minimal atypia
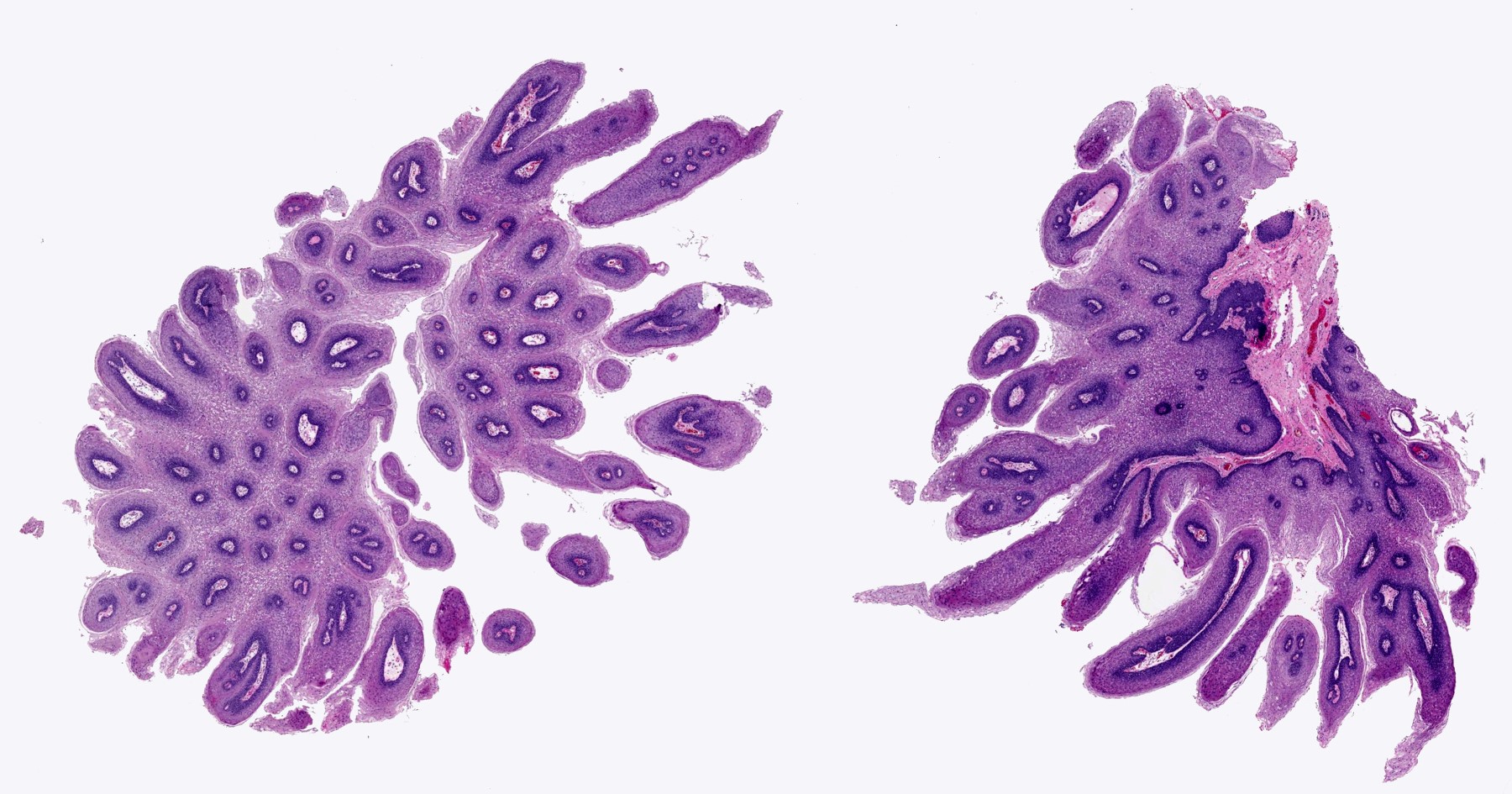
Benign, exophytic squamous epithelial proliferation that is composed of branching papillary fronds with central fibrovascular cores lined by hyperplastic nonkeratinizing squamous epithelium, usually associated with low risk human papilloma virus (HPV) infection; in particular, genotypes 6 and 11
Children: often occurs in < 5 years, no sex predilection
Adults: most frequently impacts patients in their 20s to 40s but may occur at any age; male predominant with M:F = ~3:2
Decreased incidence in children since the introduction of quadrivalent HPV vaccination program (J Infect Dis 2018;217:208)
Sites
Affects sites where ciliated respiratory type and squamous epithelium are juxtaposed
Most frequently occurs in the larynx (involving the true vocal folds and ventricles), followed by the false vocal cords (Laryngoscope 2018;128:138)
May rarely extend to extralaryngeal locations, such as epiglottis, subglottic area, hypopharynx and nasopharynx, tracheobronchial tree and pulmonary parenchyma (Respir Med 2017;126:116)
Adult: sexual contact and reactivation of latent infection from childhood
Unknown etiology in HPV negative papilloma / papillomatosis, which occurs mostly in adult setting and is associated with an increased risk of laryngeal carcinoma (PLoS One 2014;9:e99114)
Clinical features
Can be divided into 4 subtypes: juvenile solitary, juvenile multiple, adult solitary and adult multiple
Children: triad of progressive hoarseness, stridor and breathing difficulty (Respir Med 2017;126:116)
Adverse risk factors associated with aggressive behavior of the lesion (e.g., extralaryngeal spread and recurrence) include: HPV11 infection, younger age of onset, tracheostomy performed to avoid airway obstruction and previous invasive procedures (Viruses 2021;13:1624)
Carcinomatous transformation reported in 3 - 6% of patients; reported to be associated with pulmonary disease, adult onset disease, previous irradiation and smoking (Viruses 2021;13:1624)
Other treatments include antiviral therapy (such as cidofovir) and intralesional injections of anti-angiogenic drugs (such as bevacizumab) (Respir Med 2017;126:116)
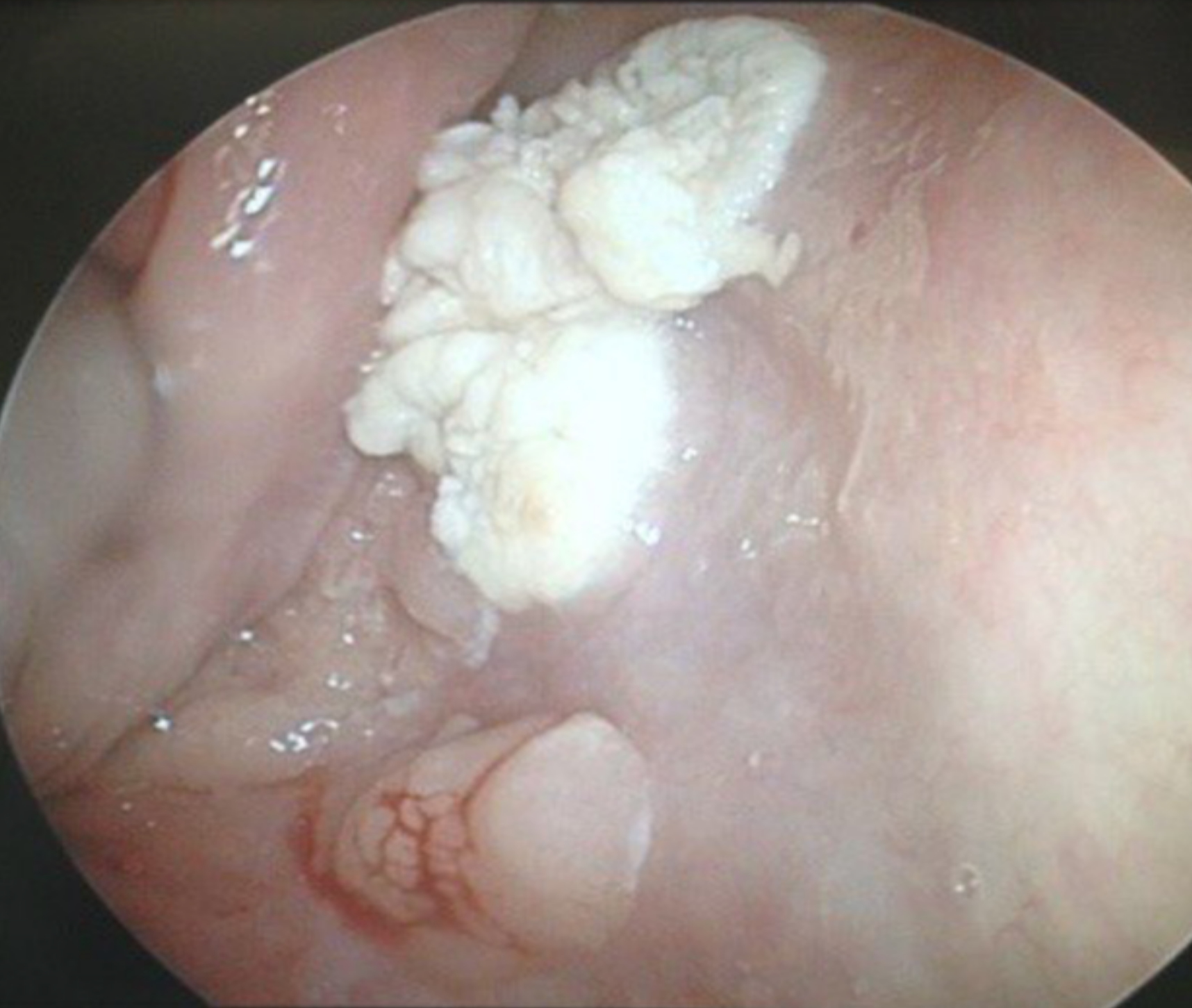
Exophytic cauliflower-like, sessile or pedunculated pinkish-whitish masses with bosselated surfaces
Mucosa appears velvety in microscopic (small) papillomas
Gross images
Images hosted on other servers:
Laryngectomy for massive papillomas
Microscopic (histologic) description
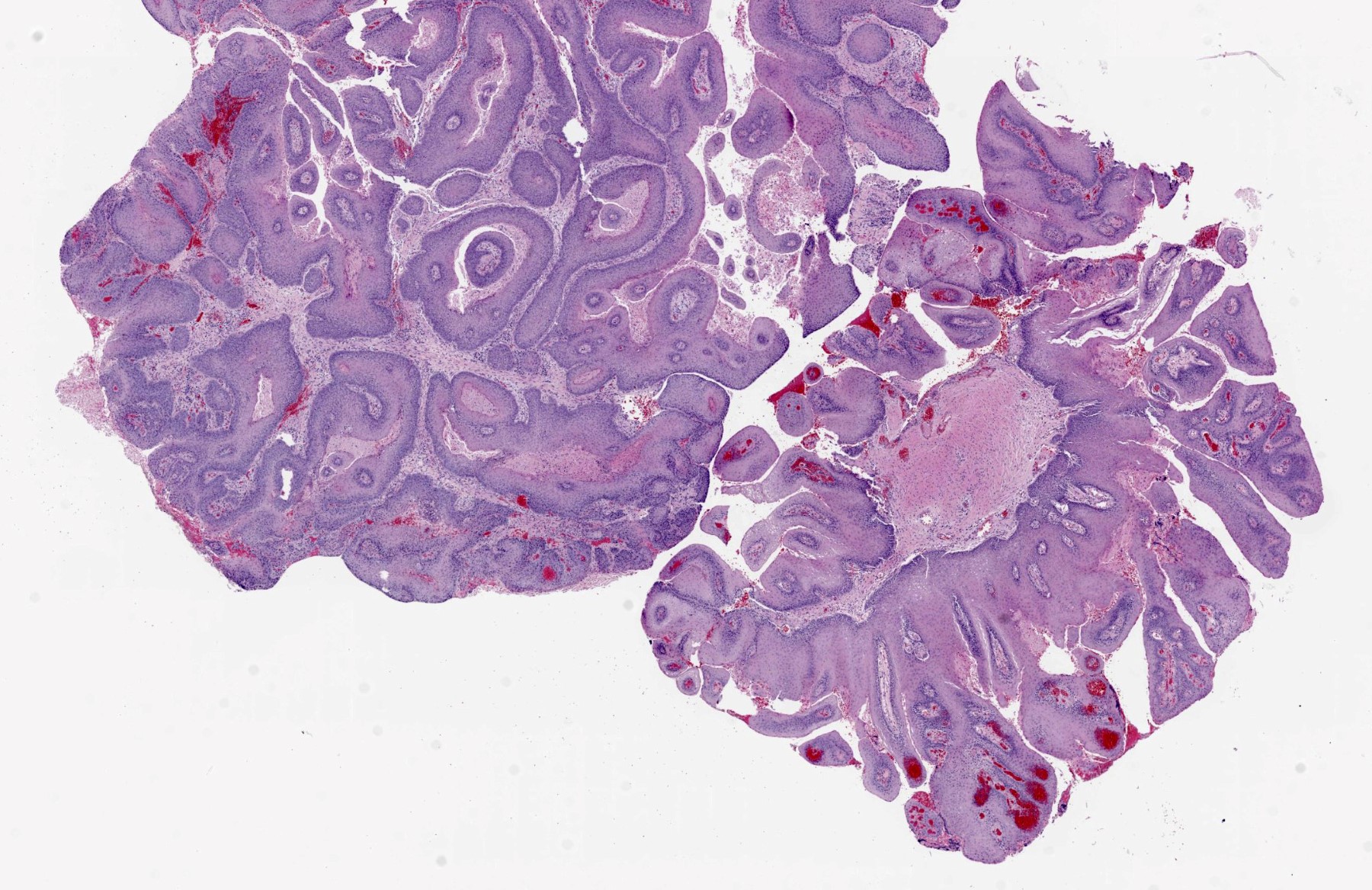
Finger-like projections or multiple fronds with a central fibrovascular core, covered by benign hyperplastic stratified squamous epithelium
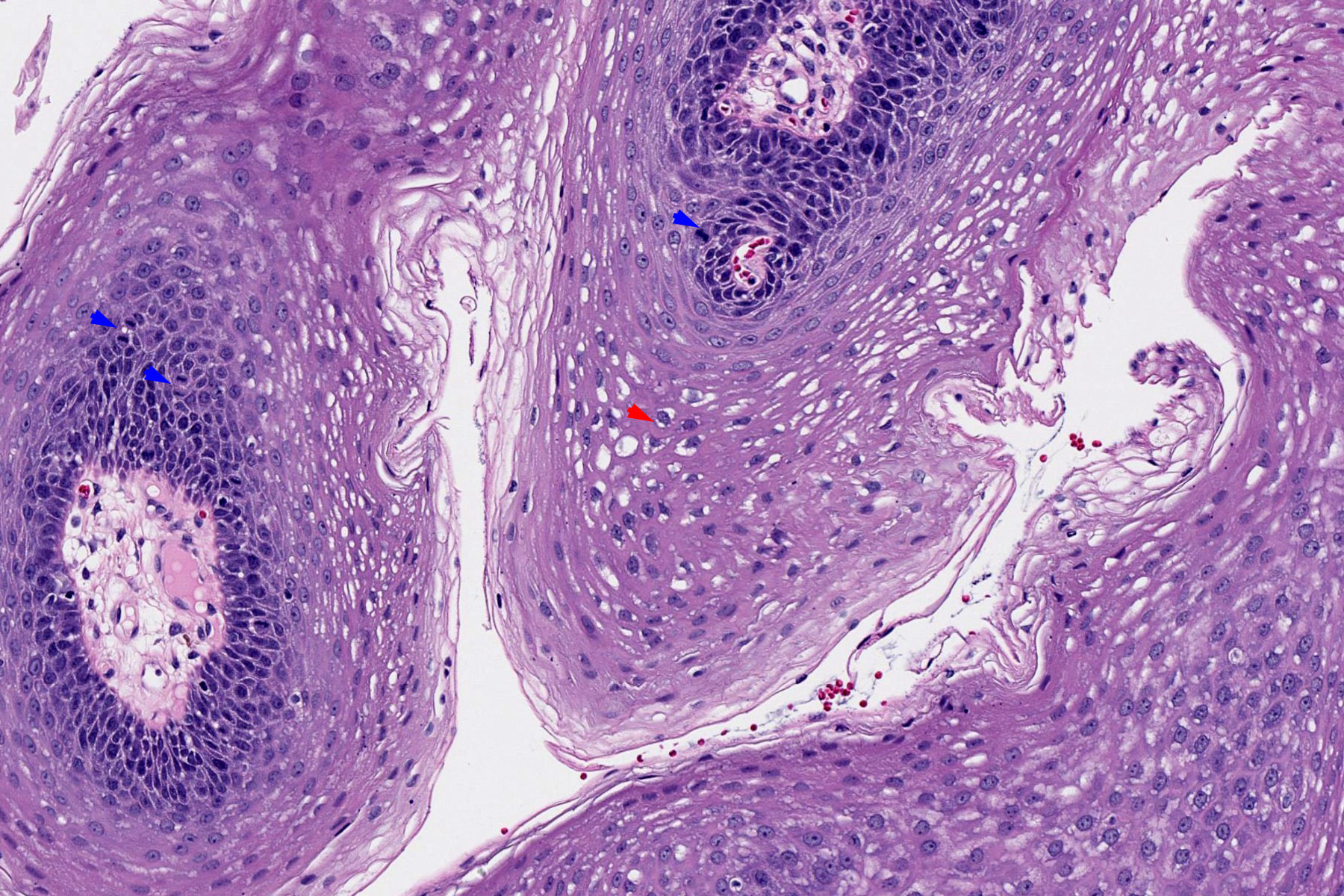
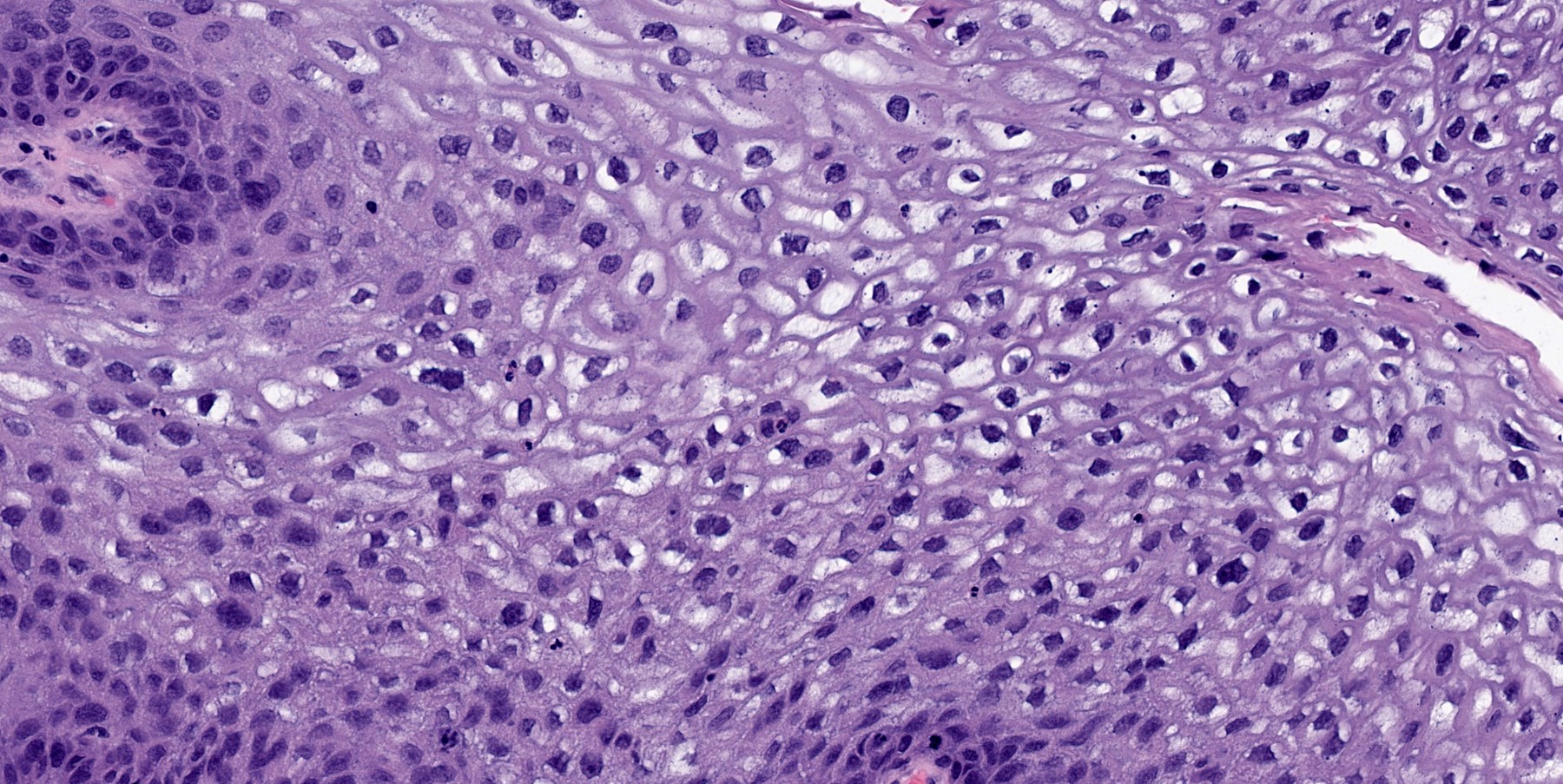
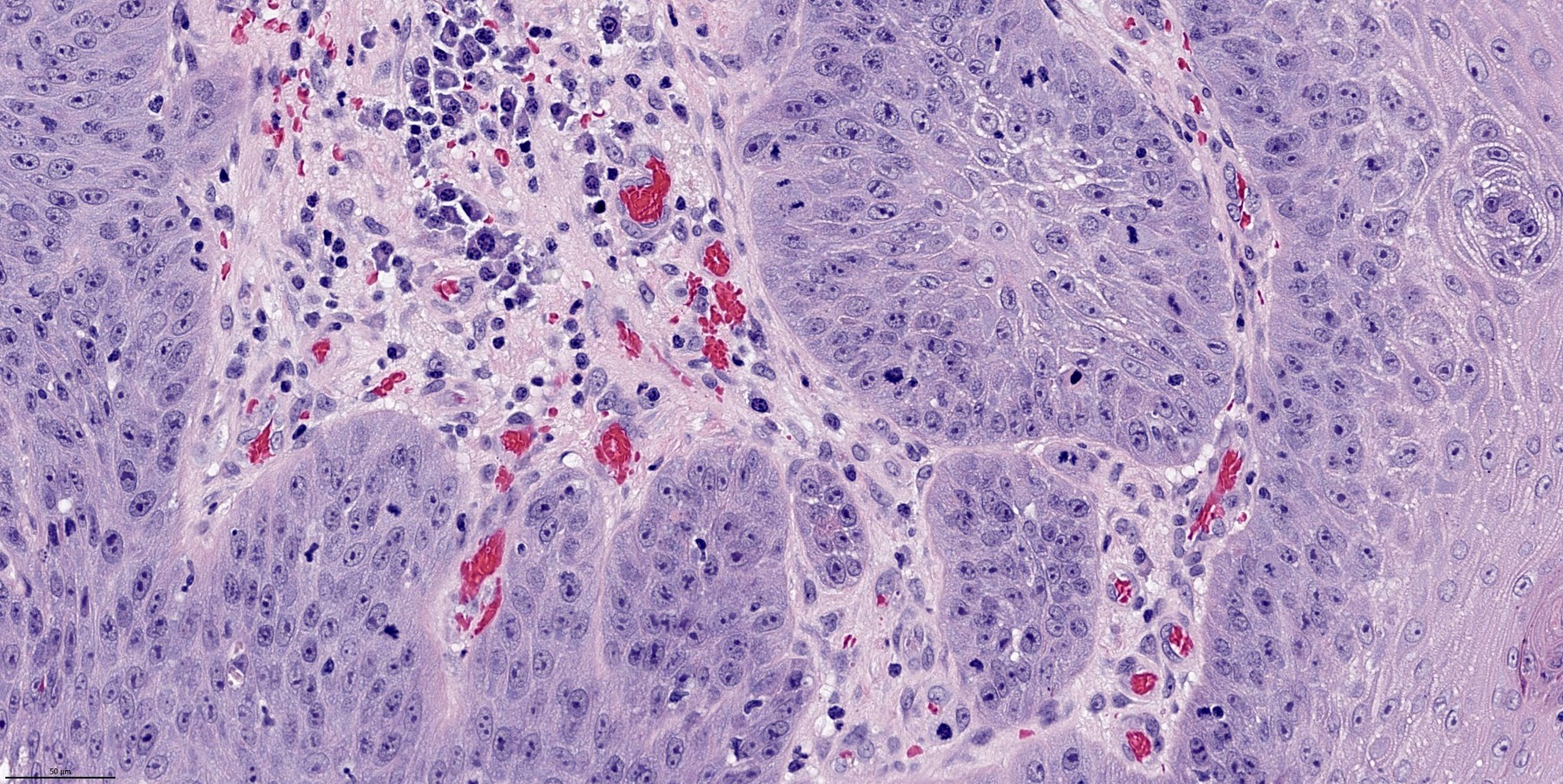
Basal and parabasal hyperplasia
Increased mitotic figures in the basal and parabasal layers
Koilocytic changes in upper layer: may be pronounced or subtle
Surface keratinization: absent to minimal
Malignant transformation is characterized by aberrant (paradoxical) keratinization, marked cytological atypia, focal necrosis, increased mitoses and atypical mitoses not limited to the basal and parabasal layers, as well as invasive growth pattern (Respir Med 2017;126:116)
Microscopic (histologic) images
Contributed by Kavita Umrau, M.B.B.S. and Bin Xu, M.D., Ph.D.
Branching finger-like papillae
Basal and parabasal mitosis
Basal and parabasal hyperplasia
Koilocytic changes
Malignant transformation
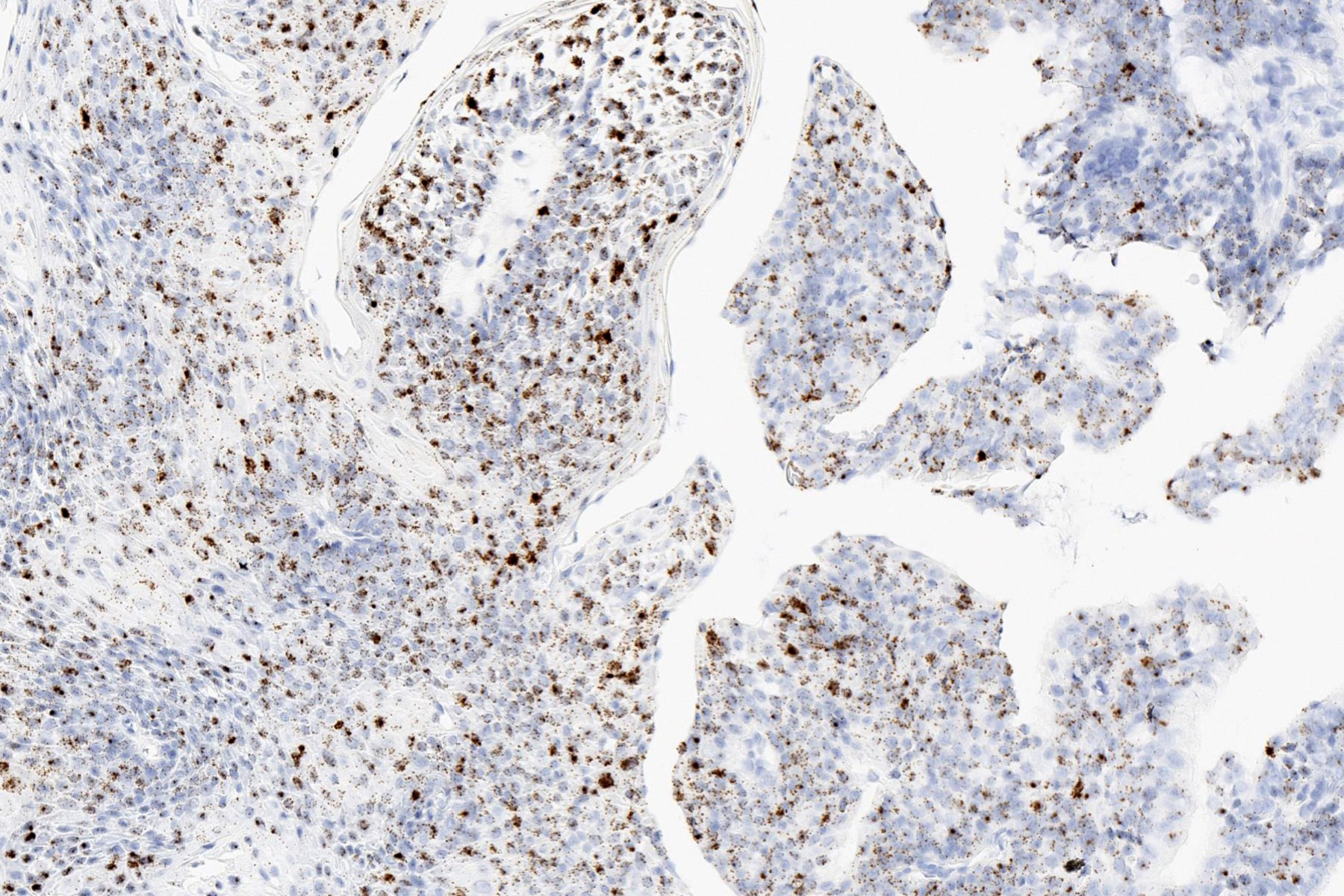
Low risk HPV
Positive stains
RNA or DNA in situ hybridization for low risk HPV is typically positive
Integrated pattern detected by DNA in situ hybridization is associated with increased risk of recurrence in pediatric patients (Head Neck Pathol 2012;6:3)
Usually involves true vocal cords and interarytenoid area
Associated with smokers, singers and others who use voices excessively
Gross description
White thickening of involved areas
Verrucous keratosis if undulating warty configuration
Pachyderma larynges if extensive keratinization
Microscopic (histologic) description
When in respiratory (ciliated columnar) epithelium (false cord, ventricle, subglottic region), initially hyperplasia of reserve cells under epithelium, then replacement of epithelium by full thickness reserve cells, then complete squamous metaplasia; may have hyperkeratotic epithelium
No nuclear abnormalities are present but underlying submucosal glands persist
Pseudoepitheliomatous hyperplasia:
Exuberant reactive overgrowth of squamous epithelium without atypia
Uncommon in larynx; more common elsewhere in upper aerodigestive tract
90% male; mean age 66 years, range 35 - 92 years
Associated with smoking (87%), alcohol (48%) and history of radiation therapy
71% are glottic; 59% are T1
May recur locally (18%) or have distant metastases (14%); 18% die of disease
Nodal metastases may have epithelial or stromal patterns or both
Prognostic factors
Depth of invasion more important than differentiation of spindle component
Treatment
Surgery with or without radiation; 45% recur
Gross description
Polypoid (99%) tumors, mean size 2 cm
Microscopic (histologic) description
Squamous cell carcinoma with spindle cell component (reactive, sarcomatous or variant of squamous cell carcinoma) that is often storiform or pleomorphic, may contain foci of benign or malignant cartilage or bone
Frequent mitotic activity; often squamous cell carcinoma in situ
All carcinomas of the hypopharynx are covered by this staging system
The following topics are not covered: metastatic tumors to the hypopharynx, hematopoietic malignancies, sarcomas of the hypopharynx
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
Terminology
Hypopharynx:
Portion of the pharynx extending from the plane of the superior border of the hyoid bone (or floor of the vallecula) to the plane corresponding to the lower border of the cricoid cartilage
Contents include:
Pyriform sinus (right and left): represents part of the hypopharynx which expands bilaterally and forward around the sides of the larynx, and lies between the larynx and the thyroid cartilage
Lateral and posterior hypopharyngeal walls
Postcricoid region, extending from the level of the arytenoid cartilage and connecting folds to the inferior border of the cricoid cartilage; it connects the 2 piriform sinuses, thereby forming the anterior wall of the hypopharynx
C13.1 - malignant neoplasm of aryepiglottic fold, hypopharyngeal aspect
C13.2 - malignant neoplasm of posterior wall of hypopharynx
C13.8 - malignant neoplasm of overlapping sites of hypopharynx
C13.9 - malignant neoplasm of hypopharynx, unspecified
Primary tumor (pT)
pN: not assigned (no nodes submitted or found)
pN: not assigned (cannot be determined based on available pathological information)
pTis: carcinoma in situ
pT1: tumor limited to one subsite of hypopharynx or ≤ 2 cm in greatest dimension
pT2: tumor invades > 1 subsite of hypopharynx or an adjacent site, or tumor > 2 cm but ≤ 4 cm in greatest dimension without fixation of hemilarynx
pT3: tumor > 4 cm in greatest dimension or with fixation of hemilarynx or extension to esophageal mucosa
pT4a: tumor of any size invading thyroid / cricoid cartilage, hyoid bone, thyroid gland, esophageal muscle or central compartment soft tissue (central compartment soft tissue includes prelaryngeal strap muscles and subcutaneous fat)
pT4b: tumor of any size that invades prevertebral fascia, encases carotid artery or involves mediastinal structures
Regional lymph nodes (pN)
pN: not assigned (no nodes submitted or found)
pN: not assigned (cannot be determined based on available pathological information)
pN0: no regional lymph node metastasis
pN1: metastasis in a single ipsilateral lymph node, ≤ 3 cm and extranodal extension (ENE)-
pN2: metastasis in a single ipsilateral lymph node, ≤ 3 cm in greatest dimension and ENE+; or > 3 cm but ≤ 6 cm in greatest dimension and ENE-; or metastases in multiple ipsilateral lymph nodes, none > 6 cm in greatest dimension and ENE-; or in bilateral or contralateral lymph node(s), none > 6 cm in greatest dimension and ENE-
pN2a: metastasis in either:
Single ipsilateral lymph node that is ≤ 3 cm and ENE+ or
Single ipsilateral lymph node that is > 3 cm but ≤ 6 cm in greatest dimension and ENE-
pN2b: metastasis in multiple ipsilateral lymph nodes, none > 6 cm in greatest dimension and ENE-
pN2c: metastasis in bilateral or contralateral lymph node(s), none > 6 cm in greatest dimension and ENE-
pN3: metastasis in a lymph node > 6 cm in greatest dimension and ENE-; or in a single ipsilateral node > 3 cm in greatest dimension and ENE+; or multiple ipsilateral, contralateral or bilateral nodes, any with ENE+; or a single contralateral node of any size and ENE+
pN3a: metastasis in a lymph node that is > 6 cm in greatest dimension and ENE-
pN3b: metastasis in either:
Single ipsilateral lymph node, > 3 cm and ENE+ or
Multiple ipsilateral, contralateral or bilateral lymph nodes, any with ENE+ or
Single contralateral lymph node of any size and ENE+
Notes:
Per AJCC 8th edition, for pN, a selective neck dissection will include 10+ lymph nodes and a comprehensive neck dissection (radical or modified radical neck dissection) will include 15+ lymph nodes
Negative pathologic examination of a smaller number of nodes still mandates a pN0 designation
Midline nodes are considered ipsilateral nodes
Measurement of tumor metastasis:
Cross sectional diameter of the largest lymph node metastatic deposit (not the lymph node itself) is measured in the gross specimen at the time of macroscopic examination or if necessary, using the histologic slide; may include matted or fused nodes
Extranodal extension (ENE):
AJCC 8th edition introduces the use of ENE in pN categorization
Must be clearly defined as tumor present within the confines of the lymph node and as extending through the lymph node capsule into the surrounding connective tissue, with or without associated stromal reaction
Distant metastasis (pM)
pM1: distant metastasis
Prefixes
y: preoperative radiotherapy or chemotherapy
r: recurrent tumor
AJCC prognostic stage groups
Stage 0:
Tis
N0
M0
Stage I:
T1
N0
M0
Stage II:
T2
N0
M0
Stage III:
T3
N0
M0
or
T1 - 3
Stage IVA:
T4a
N0 - 1
M0
or
T1 - 4a
Stage IVB:
T4b
any N
M0
or
any T
Stage IVC:
any T
any N
M1
Registry data collection variables
Extranodal extension clinical (present versus absent)
Extranodal extension pathological (present versus absent)
Extent of microscopic extranodal extension (distance of extension from the native lymph node capsule to the farthest point of invasion in extranodal tissue)
Perineural invasion
Lymphovascular invasion
p16 / HPV status
Performance status
Tobacco use and pack years
Alcohol use
Depression diagnosis
Histologic grade (G)
GX: cannot be assessed
G1: well differentiated
G2: moderately differentiated
G3: poorly differentiated
Histopathologic type
Carcinoma of the hypopharynx:
Squamous cell carcinoma:
HPV unrelated (negative) squamous cell carcinoma
Variants of squamous cell carcinoma:
Keratinizing
Nonkeratinizing
Acantholytic squamous cell carcinoma
Adenosquamous carcinoma
Basaloid squamous cell carcinoma
Papillary squamous cell carcinoma
Spindle cell squamous cell carcinoma
Verrucous squamous cell carcinoma
Lymphoepithelial carcinoma
Carcinoma of minor salivary gland:
Acinic cell carcinoma
Adenoid cystic carcinoma
Adenocarcinoma, NOS
Basal cell adenocarcinoma
Carcinoma ex pleomorphic adenoma
Carcinoma type cannot be determined
Carcinosarcoma
Clear cell adenocarcinoma
Cystadenocarcinoma
Epithelial myoepithelial carcinoma
Secretory carcinoma
Mucoepidermoid carcinoma
Mucinous carcinoma
Myoepithelial carcinoma
Oncocytic carcinoma
Polymorphous adenocarcinoma
Salivary duct carcinoma
Neuroendocrine carcinoma:
Small cell neuroendocrine carcinoma, HPV-
Small cell neuroendocrine carcinoma, HPV+
Large cell neuroendocrine carcinoma, HPV-
Large cell neuroendocrine carcinoma, HPV+
Clinical images
Contributed by Michael Elliott, M.B.B.S., M.Phil. and Carsten Palme, M.B.B.S.
Ulcerated hypopharyngeal lesion
Keratotic hypopharyngeal lesion
Polypoid ulcerated hypopharyngeal lesion
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
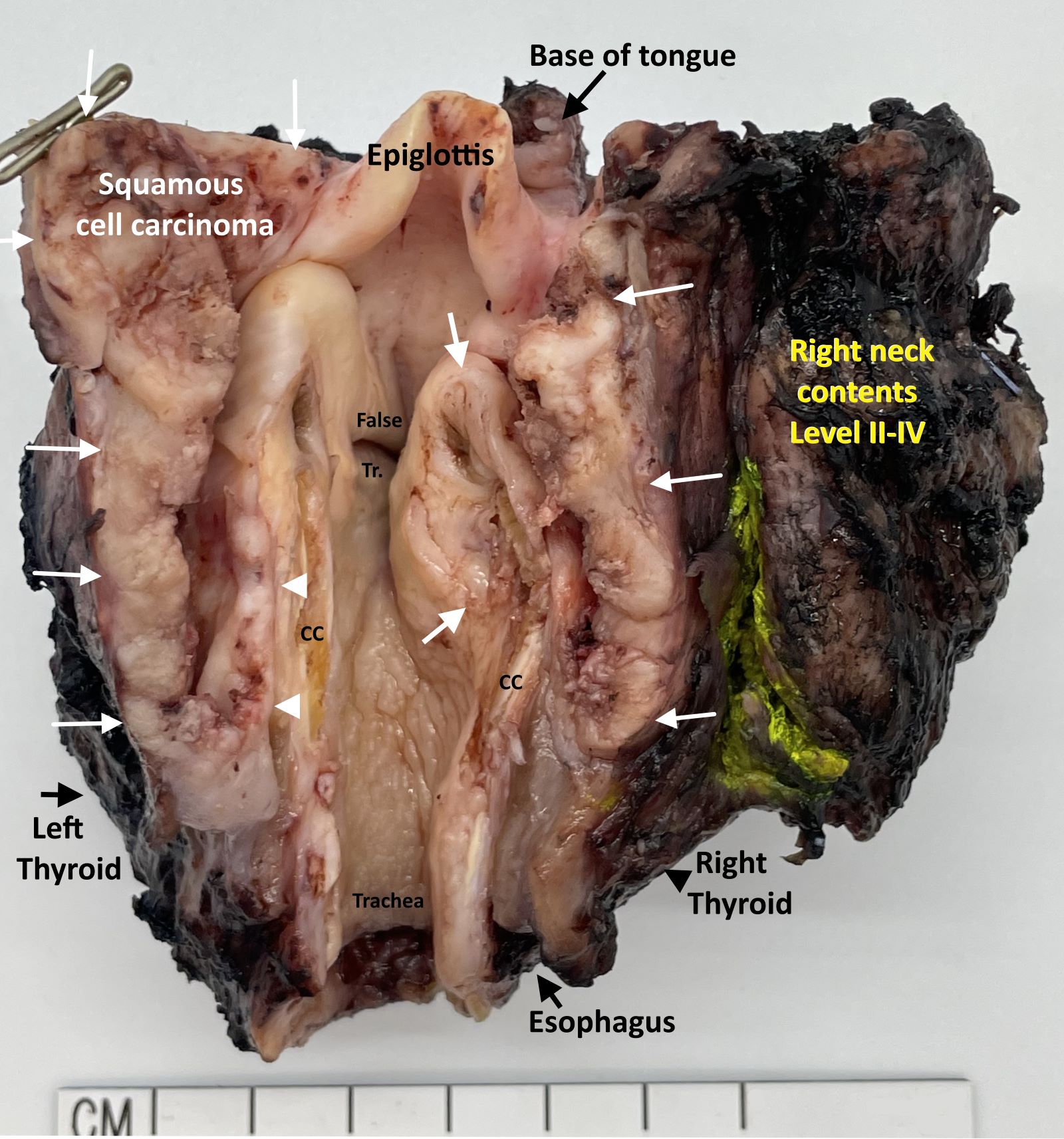
Laryngopharyngectomy, opened posteriorly (pT4a)
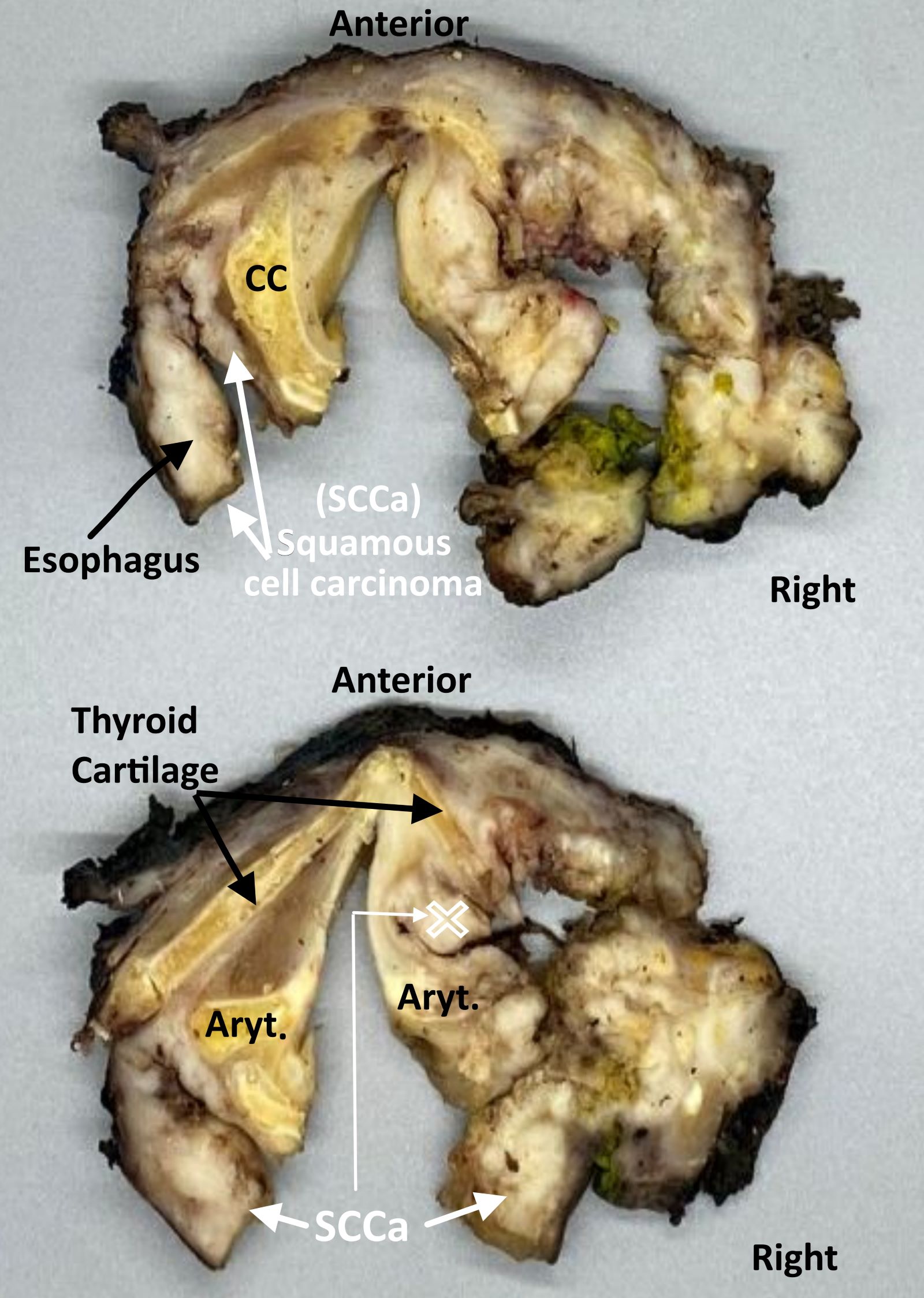
Laryngopharyngectomy, sectioned (pT4a)
Board review style question #1
Which of the following is the pTNM stage (per the AJCC 8th edition) of a 3.1 cm right hypopharyngeal squamous cell carcinoma invading the right thyroid cartilage and true cord, with no lymph node metastases identified?
pT1c N0, stage IC
pT1c N0, stage IVB
pT3b N0, stage IIIB
pT3c N0, stage IVB
pT4a N0, stage IVA
Board review style answer #1
E. pT4a N0, stage IVA. Invasion into the thyroid cartilage, irrespective of tumor size is pT4a.
Staging of definitive resections for carcinoma (squamous cell carcinoma, neuroendocrine carcinoma and minor salivary gland carcinoma) of the supraglottic, glottis and subglottic larynx should use this system
Pyriform sinus represents part of the hypopharynx which expands bilaterally and forward around the sides of the larynx and lies between the larynx and the thyroid cartilage
Cancers of the pyriform sinus are included in the protocol on pharynx cancers
Staging protocols such as those of CAP document procedure, tumor site, transglottic extension, tumor laterality, tumor focality, tumor size, histologic type, histologic grade for squamous cell carcinoma, margin status, lymphovascular invasion, perineural invasion, regional lymph node findings and summarize these pathologic findings using TNM system
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
CAP protocol recommends the TNM staging system of the American Joint Committee on Cancer
There are no significant alterations in the 8th edition to T stage of larynx
However, extranodal extension (ENE) is now included in N stage
In essence, pathologic ENE+ will increase the nodal category by 1
Use of the CAP protocol is not required for recurrent tumors or for metastatic tumors that are resected at a different time than the primary tumor
Use of the CAP protocol is not required for pathology reviews performed at a second institution (i.e., secondary consultation, second opinion or review of outside case at second institution)
Anterior limit of the larynx is composed of the anterior or lingual surface of the suprahyoid epiglottis, the thyrohyoid membrane, the anterior commissure and the anterior wall of the subglottic region, which is composed of the thyroid cartilage, the cricothyroid membrane and the anterior arch of the cricoid cartilage
Posterior and lateral limits include the laryngeal aspect of the aryepiglottic fold, the arytenoid region, the interarytenoid space and the posterior surface of the subglottic space represented by the mucous membrane covering the surface of the cricoid cartilage
Superolateral limits are composed of the tip and the lateral borders of the epiglottis
Inferior limits are made up of the plane passing through the inferior edge of the cricoid cartilage
Paraglottic space is a potential space deep to the ventricles and saccules filled with adipose tissue and connective tissue (see figure 2 in Diagrams / tables)
It is bounded by the conus elasticus inferiorly, the thyroid cartilage laterally, the quadrangular membrane medially and the piriform sinus posteriorly
Pre-epiglottic space, like the paraglottic space, is filled with adipose tissue and connective tissue (see figure 3 in Diagrams / tables)
It is triangular in shape and is bounded by the thyroid cartilage and thyrohyoid membrane anteriorly, the epiglottis and thyroepiglottic ligament posteriorly and the hyoepiglottic ligament at its base (see figures 1 and 2 Diagrams / tables)
Paraglottic and preglottic spaces contain lymphatics and blood vessels but no lymph nodes
Supraglottic squamous cell carcinoma: a squamous cell carcinoma that involves the structures of the supraglottic larynx, including the epiglottis (laryngeal and lingual surfaces), aryepiglottic folds, arytenoids, false vocal cords and ventricles
Glottic squamous cell carcinoma: a squamous cell carcinoma that involves the structures of the glottis, including the true vocal cords and the anterior and posterior commissures
Subglottic squamous cell carcinoma: a squamous cell carcinoma that involves the subglottis, which begins 1 cm below the apex of the ventricle to its inferior border represented by the rim of the cricoid cartilage
Transglottic carcinoma: a carcinoma that crosses the ventricles in a vertical direction arising in either the glottic or supraglottic larynx
pT1: Tumor limited to 1 subsite of supraglottis with normal vocal cord mobility
pT2: Tumor invades mucosa of > 1 adjacent subsite of supraglottis or glottis or region outside the supraglottis (e.g. mucosa of base of tongue, vallecula, medial wall of pyriform sinus) without fixation of the larynx
pT3: Tumor limited to larynx with vocal cord fixation or invades any of the following: postcricoid area, pre-epiglottic space, paraglottic space or inner cortex of thyroid cartilage
pT4a: Moderately advanced local disease: invades through the outer cortex thyroid cartilage or invades tissues beyond the larynx (e.g. trachea, soft tissues of neck including deep extrinsic muscle of tongue, strap muscles, thyroid or esophagus)
pT4b: Very advanced local disease: invades prevertebral space, encases carotid artery or invades mediastinal structure
Primary tumor (pT) - glottis
pTX: Primary tumor cannot be assessed
pTis: Carcinoma in situ
pT1: Tumor limited to the vocal cord(s) (may involve anterior or posterior commissure) with normal mobility
pT1a: Limited to 1 vocal cord
pT1b: Involves both vocal cords
pT2: Tumor extends to supraglottis or subglottis or with impaired vocal cord mobility
pT3: Tumor limited to the larynx with vocal cord fixation or invasion of paraglottic space or inner cortex of the thyroid cartilage
pT4a: Moderately advanced local disease: invades through the outer cortex of the thyroid cartilage or invades tissues beyond the larynx (e.g. trachea, cricoid cartilage, soft tissues of neck including deep extrinsic muscle of the tongue, strap muscles, thyroid or esophagus)
pT4b: Very advanced local disease: invades prevertebral space, encases carotid artery or invades mediastinal structures
Primary tumor (pT) - subglottis
pTX: Primary tumor cannot be assessed
pTis: Carcinoma in situ
pT1: Tumor limited to subglottis
pT2: Tumor extends to vocal cord(s) with normal or impaired mobility
pT3: Tumor limited to larynx with vocal cord fixation or invasion of paraglottic space or inner cortex of the thyroid cartilage
pT4a: Moderately advanced local disease: tumor invades cricoid or thyroid cartilage or invades tissues beyond the larynx (e.g. trachea, soft tissues of neck including deep extrinsic muscles of the tongue, strap muscles, thyroid or esophagus)
pT4b: Very advanced local disease: tumor invades prevertebral space, encases carotid artery or invades mediastinal structures
Pathological regional lymph nodes (pN)
pNX: Regional lymph nodes cannot be assessed
pN0: No regional lymph node metastasis
pN1: Metastasis in a single ipsilateral lymph node ≤ 3 cm in greatest dimension and extranodal extension (ENE)-
pN2a: Single ipsilateral lymph node ≤ 3 cm and ENE+ or single ipsilateral lymph node > 3 cm but ≤ 6 cm in greatest dimension and ENE-
pN2b: Metastases in multiple ipsilateral lymph nodes, none > 6 cm in greatest dimension and ENE-
pN2c: Metastases in bilateral or contralateral lymph node(s), none > 6 cm in greatest dimension and ENE-
pN3a: Metastasis in a lymph node that is > 6 cm in greatest dimension and ENE-
pN3b: Metastasis in either
Single ipsilateral lymph node, > 3 cm and ENE+ or
Multiple ipsilateral, contralateral or bilateral lymph nodes, any with ENE+ or
Single contralateral lymph node of any size and ENE+
Notes:
Designation of "U" or "L" may be used for any N category to indicate metastasis above the lower border of the cricoid (U) or below the lower border of the cricoid (L)
Per AJCC 8th edition, for pN, a selective neck dissection ordinarily will include > 10 lymph nodes and a radical or modified radical neck dissection ordinarily will include > 15 lymph nodes
Negative pathologic examination of a smaller number of nodes still mandates a pN0 designation
Midline nodes are considered ipsilateral nodes
Extranodal extension (ENE)
All macroscopically negative or equivocal lymph nodes should be submitted in toto
Grossly positive nodes may be partially submitted for microscopic documentation of metastasis
Reporting of lymph nodes containing metastasis should include whether there is presence or absence of extranodal extension (ENE), which is now part of N staging
This finding consists of extension of metastatic tumor, present within the confines of the lymph node, through the lymph node capsule into the surrounding connective tissue, with or without associated stromal reaction
Distance of extension from the native lymph node capsule is now suggested (but not yet required) with the proposed stratification of ENE into ENEma (> 2 mm) and ENEmi (≤ 2 mm)
However, pitfalls in the measurement (i.e. in larger, matted lymph nodes, in nodes post fine needle aspiration and in nodes with near total replacement of lymph node architecture) and the disposition of soft tissue deposits are still not resolved
In general, absence of ENE in a large (> 3 cm) lymph node, especially with traversing fibrous bands, should be viewed with skepticism
Soft tissue deposits for lymph node metastases based on limited studies appear to be the equivalent of a positive lymph node with ENE and should be recorded as such
Measurement of lymph node metastasis
Cross sectional diameter of the largest lymph node metastatic deposit (not the lymph node itself) is measured in the gross specimen at the time of macroscopic examination or if necessary, on the histologic slide at the time of microscopic examination
Distant metastasis (pM)
pM0: No distant metastasis
pM1: Distant metastasis
AJCC prognostic stage grouping
Stage 0:
Tis
N0
M0
Stage I:
T1
N0
M0
Stage II:
T2
N0
M0
Stage III:
T3
N0
M0
T1 - 3
N1
M0
Stage IVA:
T4a
N0 - 1
M0
T1 - 4a
N2
M0
Stage IVB:
Any T
N3
M0
T4b
Any N
M0
Stage IVC:
Any T
Any N
M1
Registry data collection variables
ENE clinical (present versus absent)
ENE pathological (present versus absent)
Extent of microscopic ENE (distance of extension from the native lymph node capsule to the farthest point of invasion in extranodal tissue)
For conventional squamous cell carcinoma, histologic grading as a whole does not perform well as a prognosticator
Nonetheless, it should be recorded when applicable as it is a basic tumor characteristic
Selecting either the most prevalent grade or the highest grade for this synoptic protocol is acceptable
Variants of squamous cell carcinoma (i.e. verrucous, basaloid, etc.) have an intrinsic biologic potential and currently do not appear to require grading
Histologic (microscopic) grading of salivary gland carcinomas has been shown to be an independent predictor of behavior and plays a role in optimizing therapy
However, most salivary gland carcinoma types have an intrinsic biologic behavior and attempted application of a universal grading scheme is merely a crude surrogate
Thus, a generic grading scheme is no longer recommended for salivary gland carcinomas
Carcinoma types for which grading systems exist and are relevant are incorporated into histologic type
3 major categories that are amenable to grading include adenoid cystic carcinoma, mucoepidermoid carcinoma and adenocarcinoma, not otherwise specified
In some carcinomas, histologic grading may be based on growth pattern, such as in adenoid cystic carcinoma, for which a histologic high grade variant has been recognized based on the percentage of solid growth
Those adenoid cystic carcinomas showing ≥ 30% of solid growth pattern are considered to be histologically high grade carcinomas
Histologic grading of mucoepidermoid carcinoma includes a combination of growth pattern characteristics (e.g. cystic, solid, neurotropism) and cytomorphologic findings (e.g. anaplasia, mitoses, necrosis)
Adenocarcinomas, not otherwise specified, do not have a formalized grading scheme and are graded intuitively based on cytomorphologic features
Histopathologic type
Predominant cancer is squamous cell carcinoma
Staging guidelines are applicable to all forms of epithelial carcinoma including those arising from minor salivary glands
Other nonepithelial tumors such as lymphoid tissue, bone, cartilage (i.e. lymphoma and sarcoma) are not included
Squamous cell carcinoma (conventional, variants)
Carcinoma of minor salivary gland
Acinic cell
Adenoid cystic
Adenocarcinoma, NOS
Basal cell adenocarcinoma
Carcinoma ex pleomorphic adenoma
Carcinoma type cannot be determined
Carcinosarcoma
Clear cell adenocarcinoma
Cystadenocarcinoma
Epithelial myoepithelial carcinoma
Mammary analogue secretory carcinoma
Mucoepidermoid carcinoma
Mucinous carcinoma
Myoepithelial carcinoma
Oncocytic carcinoma
Polymorphous adenocarcinoma
Salivary duct carcinoma
Non salivary gland adenocarcinoma
Neuroendocrine carcinoma
Well differentiated neuroendocrine carcinoma (typical carcinoid tumor)
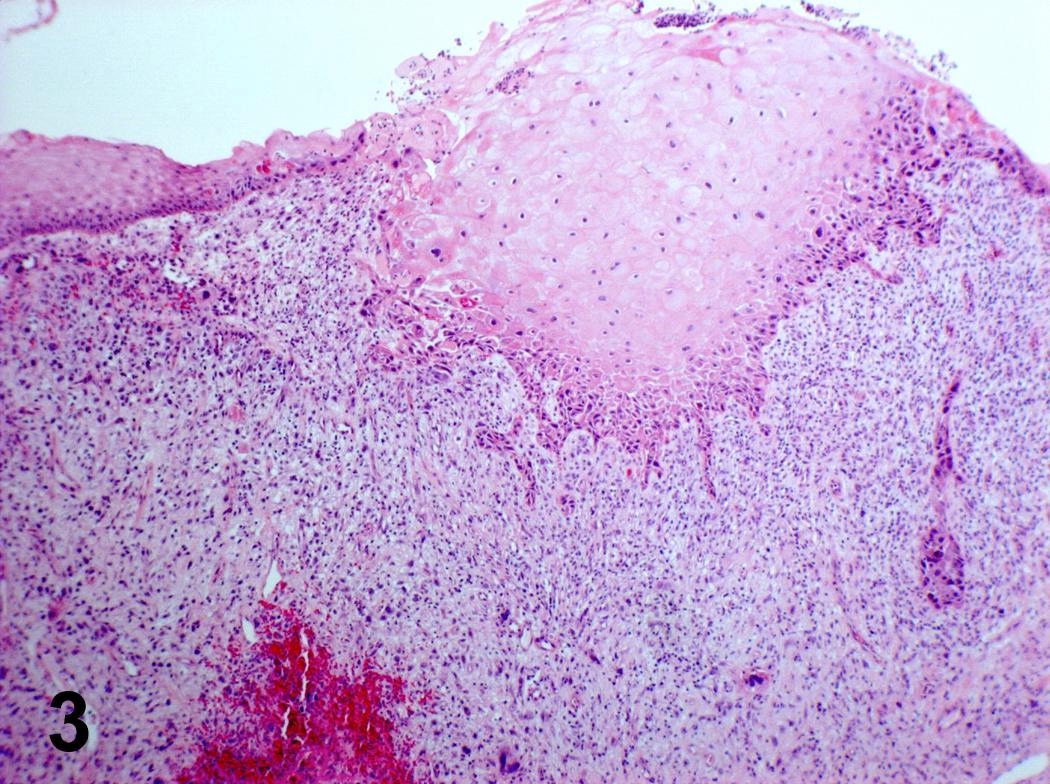
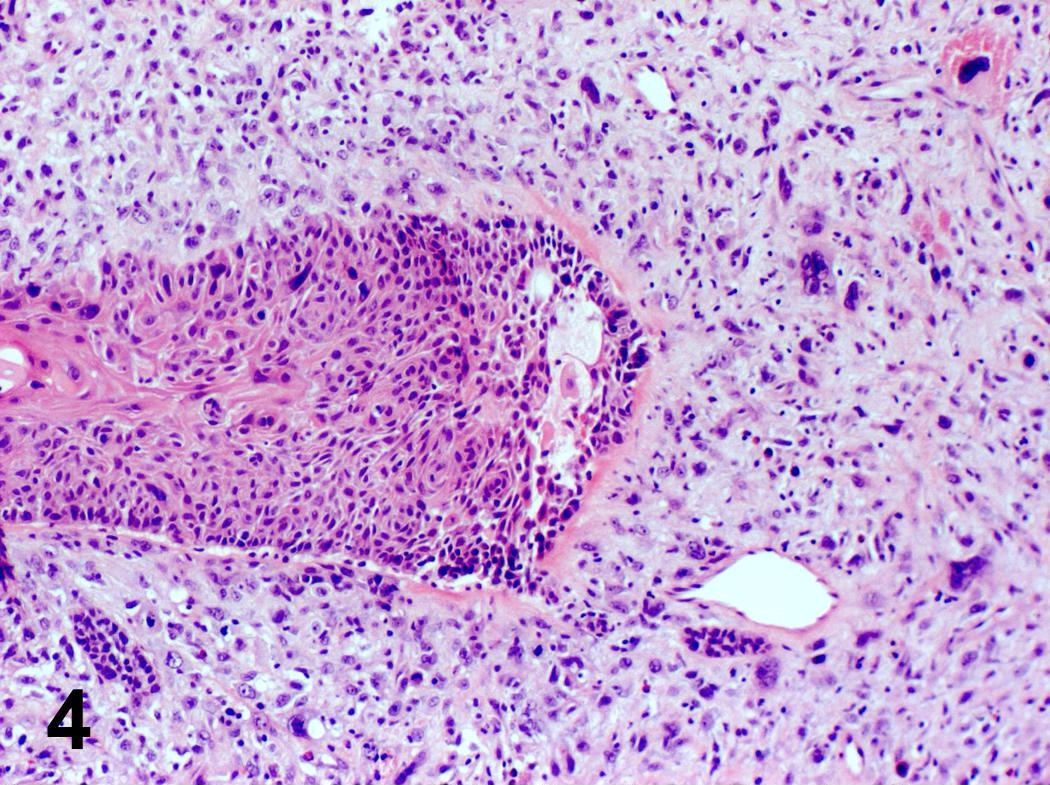
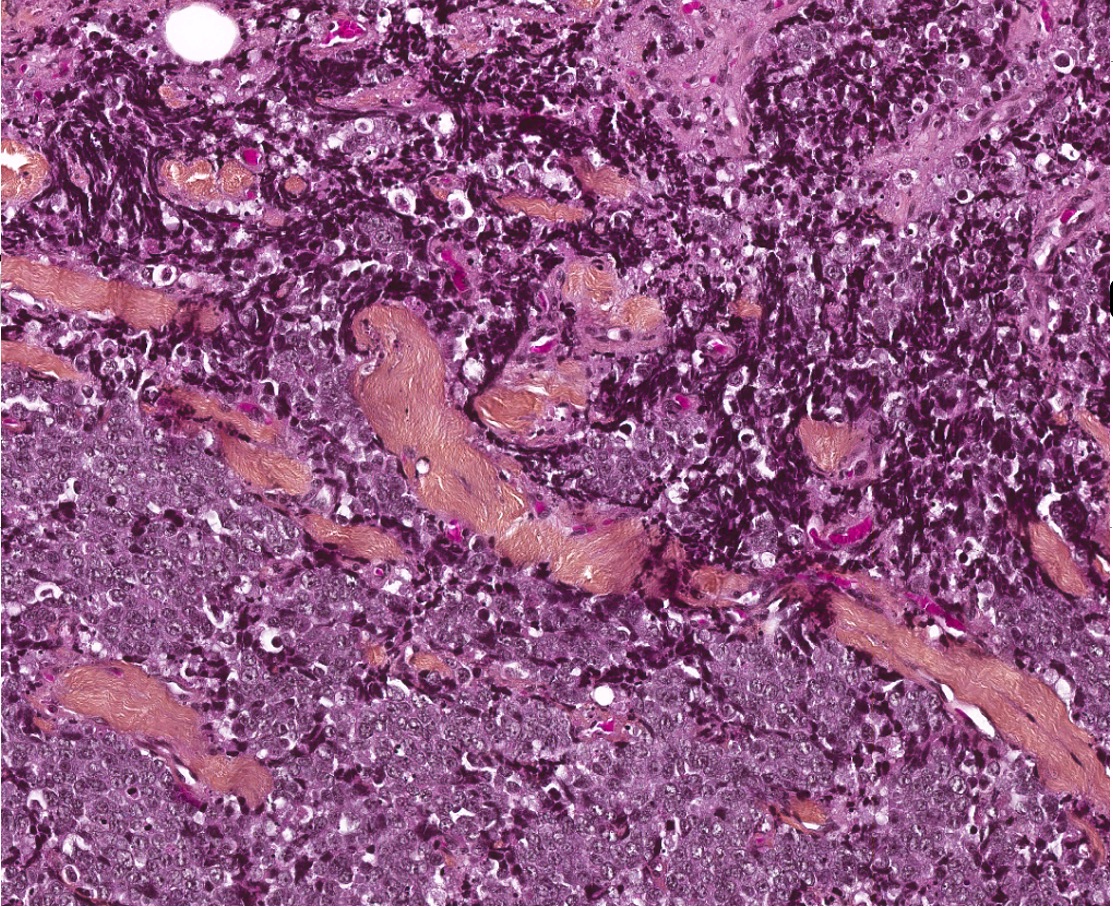
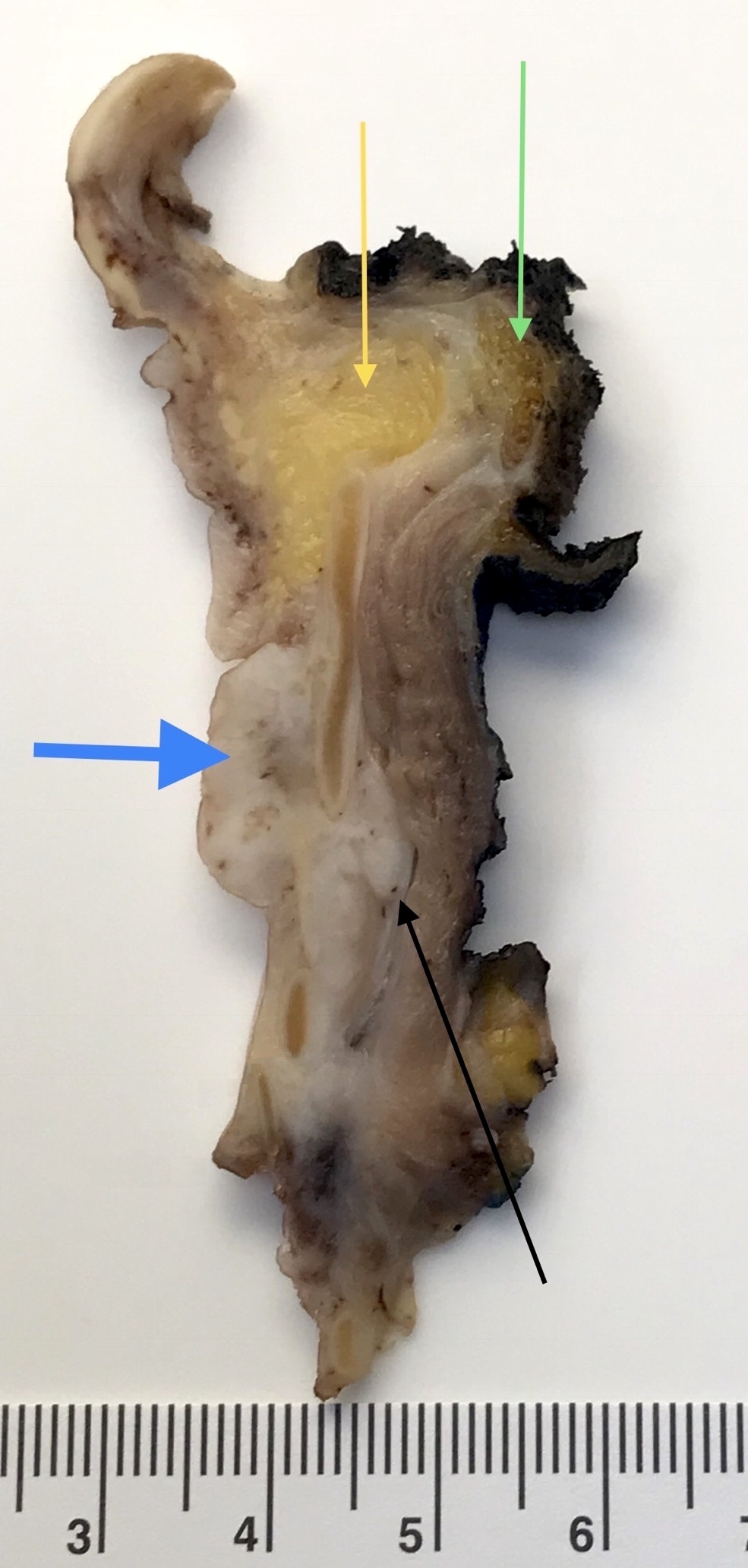
Regarding laryngeal squamous cell carcinoma, which of the pT category criteria in the 8th edition AJCC staging guide is likely to be satisfied by examination of this parasagittal section taken through the right side of a total laryngectomy specimen?
Common benign laryngeal lesion, also known as laryngeal nodule or singer's nodule
Clinical terms: nodule (sessile) versus polyp (pedunculated) (J Voice 2004;18:125)
Essential features
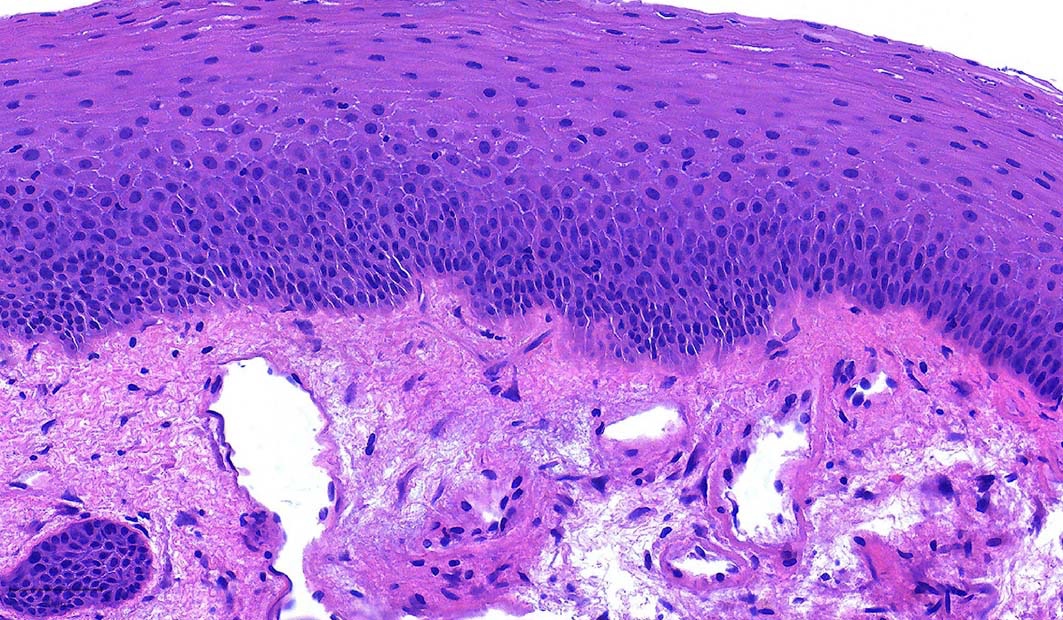
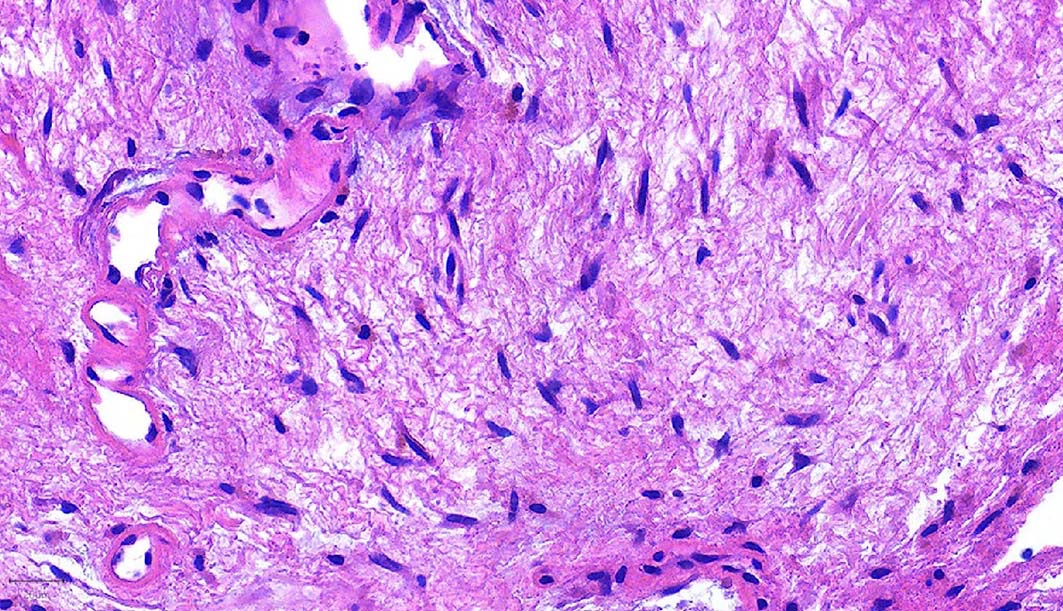
Benign exophytic, pedunculated (polyp) or sessile (nodule) lesion of the vocal cord, frequently related to voice overuse or irritation, lined by unremarkable squamous epithelium or with mild reactive atypia, overlying an edematous, myxoid or hyalinized fibroblastic stroma with telangiectatic vessels
More common in heavy smokers, patients with history of chronic irritant inhalation or singers, due to inflammation, allergic or immunologic causes, possibly secondary to hemorrhage
Frequently presents as vocal cord polyp, atypical subepithelial spindle cells (stains for keratins, p63, p40 can be helpful) with mitotic activity and associated dysplasia of the overlying squamous mucosa (Diagn Pathol 2007;2:1)
Which of the following is the most helpful diagnostic clue in the differential diagnosis of vocal cord polyp from spindle cell carcinoma?
Dysplasia in the superficial squamous mucosa
Immunoreactivity for keratins AE1 / AE3
Presence of atypical stromal cells
Telangiectatic blood vessels in the stroma
Board review style answer #1
A. Dysplasia in the superficial squamous mucosa of a polypoid laryngeal lesion should prompt the differential diagnosis of spindle cell carcinoma. The squamous mucosa of vocal cord polyps is usually unremarkable or can show mild atypia. Nonspecific immunostaining of keratins AE1 / AE3 in stomal fibroblasts or the presence of bizarre stromal cells can be diagnostic pitfalls, especially in the absence of overt dysplasia. Telangiectatic blood vessels can be seen in the stroma of both vocal cord polyps and spindle cell carcinomas.
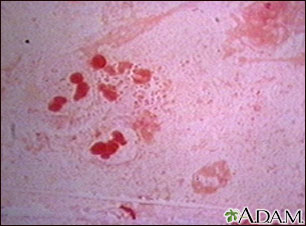
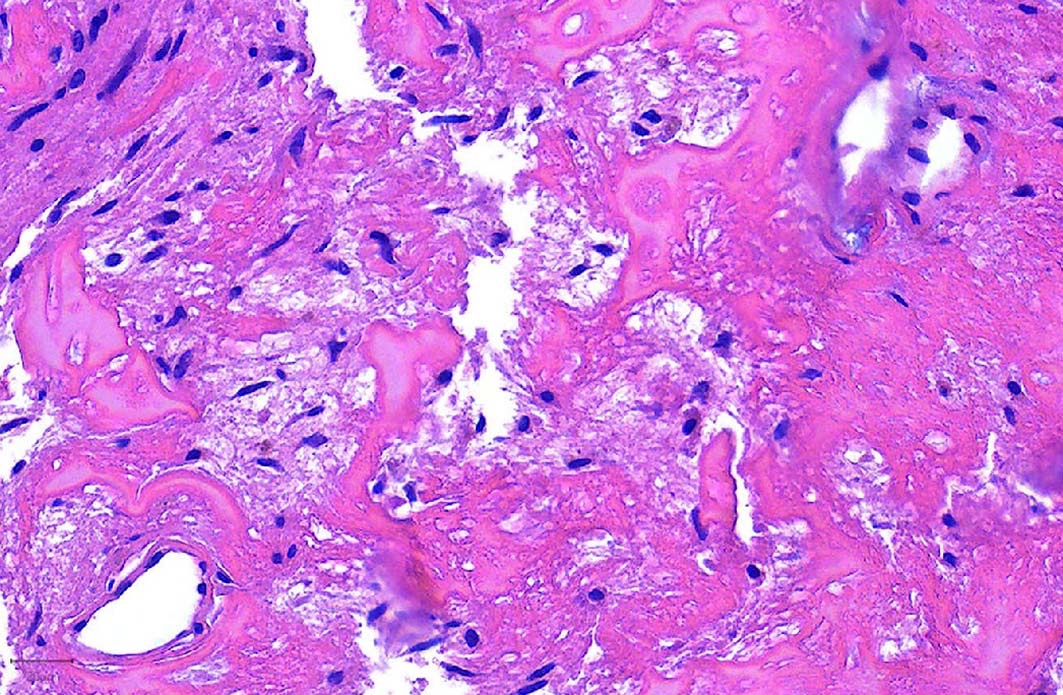
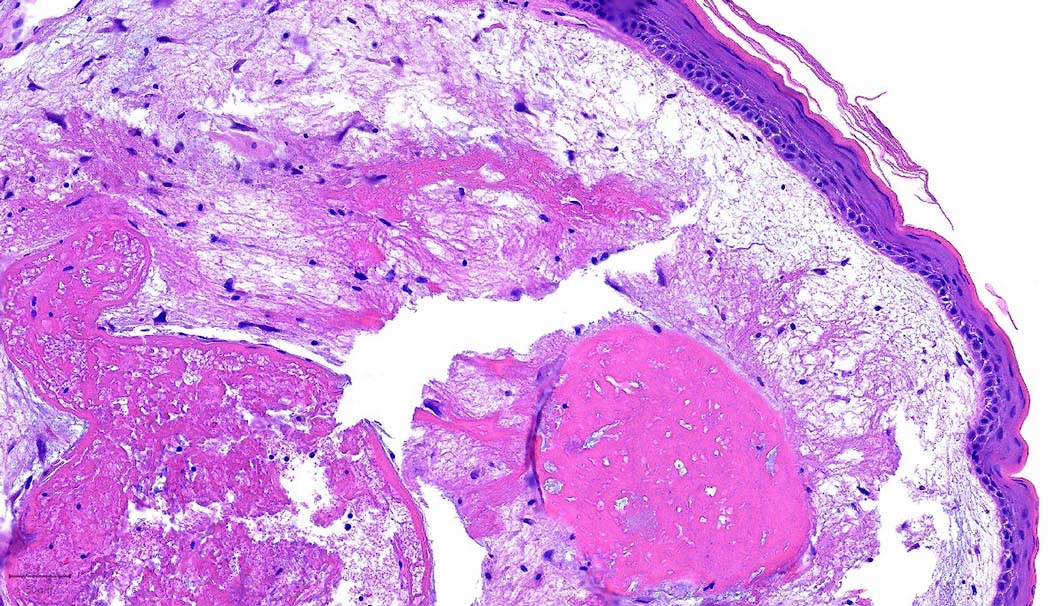
Which of the following ancillary studies is the most cost efficient in further evaluating the amorphous material seen in the laryngeal polyp of the photo?
Amyloid typing by mass spectrometry
Congo red histochemical stain
Immunohistochemistry for A and P components
TTR gene sequencing
Board review style answer #2
B. Congo red histochemical stain is a low cost, sensitive method of screening specimens for amyloid, although interpretation needs the use of special polarizing lenses. The remaining methods, although more specific, are much more expensive and their use should be reserved for the further workup of specimens with confirmed amyloidosis.